
Vaccines & Autism
{kind=link}
The ScienceBasedMedicine.org Reference Pages are reviews of topics relevant to science and medicine. Each consists of a concise overview of the topic from a scientific perspective, an index of the most relevant posts here on SBM, links to some external resources we recommend, and our summaries of the most interesting and important research. These pages are a work in progress, and we are actively developing them over the summer and fall of 2013, starting with acupuncture, chiropractic, homeopathy, and vaccines & autism.
Overview of Vaccines & Autism
Vaccines are generally considered to be the most successful public health intervention ever devised. And yet there have been opponents of vaccines ever since there have been vaccines. So-called antivaccinationists have claimed over the years that vaccines do not work, despite the overwhelming evidence that they do. They often spread misinformation about vaccine, such as the notion that vaccines weaken the immune system, when in fact they work by strengthening the immune response against the target infection.
In recent years the antivaccine movement has focused on the claim that vaccines are linked to neurological injury, and specifically to the neurological disorder autism, now referred to as autism spectrum disorder (ASD). However the scientific evidence overwhelmingly shows no correlation between vaccines in general, the MMR vaccine specifically, or thimerosal (a mercury-based preservative) in vaccines with ASD or other neurodevelopmental disorders.
The primary argument made for an association between thimerosal and ASD is that the rate of diagnosis of ASD has been steadily increasing since the early 1990s. At that time also the routine vaccine schedule was increasing, resulting in an increasing total dose of thimerosal. The antivaccinationists then assume causation from correlation to blame rising ASD rates on thimerosal.
However, by 2002 thimerosal was completely removed from the routine vaccine schedule, and now remains only in some flu vaccines. The total dose of thimerosal exposure is far below 1990 levels, before ASD diagnoses began to rise. Antivaccinationists predicted that ASD rates would fall dramatically in the years following the removal of thimerosal from most vaccines – but rates have continued to rise without even the slightest change in the rate of increase. This is a powerful refutation of the thimerosal-autism hypothesis, and has been replicated in other countries.
Further, the best epidemiological evidence suggests that the rise in the diagnosis rate of ASD is an artifact of broadening the definition of autism, diagnostic substitution, and increased surveillance. Therefore there isn’t really an autism “epidemic” just a change in the definition and efforts to make the diagnosis.
Undaunted, the antivaccinationists have changed their claims to blame any number of “toxins” in vaccines. However, their claims have no scientific validity.
Index of SBM Posts about Vaccines & Autism
- What are words for? Mark Crislip, Sep 20 ’13
- Another antivaccine zombie meme: polio vaccine and SV40 and cancer, oh, my! David Gorski, Sep 9 ’13
- I refute it thus Mark Crislip, Sep 6 ’13
- MMR and Autism Rises from the Dead Steven Novella, Sep 4 ’13
- Sharyl Attkisson and CBS News: An epic fail in reporting on the murder of autistic teen Alex Spourdalakis David Gorski, Sep 2 ’13
- Danger Zones of Parental Vaccine Refusal John Snyder, Sep 1, 2013
- Preventing autism? Not so fast, Dr. Mumper… David Gorski, Aug 26, 2013
- Autism and Induced Labor Steven Novella, Aug 14 ’13
- TA favorite tactic of the antivaccine movement: When science doesn’t support you, use the law David Gorski, Aug 5, 2013
- Prenatal Mercury and Autism Steven Novella, Jul 24 ’13
- The murder of autistic teen Alex Spourdalakis by his mother and caregiver: What happened? David Gorski, Jun 16 ’13
- The final nail in the coffin for the antivaccine rallying cry “Too many too soon”? David Gorski, Apr 1 ’13
- Blame and magical thinking: The consequences of the autism “biomed” movement David Gorski, Feb 25 ’13
- One Flu Into the Cuckoo’s Nest* Mark Crislip, Jan 25 ’13
- The antivaccine movement and “autism biomed” versus “outgrowing” autism David Gorski, Jan 21 ’13
- An Alternative “Truth” About Flu Shots Harriet Hall, Dec 25 ’12
- Another blow to the anti-vaccine movement as legislation change forces a name change Rachael Dunlop, Dec 23 ’12
- The antivaccine lie that just won’t die: The claim that shaken baby syndrome is really due to “vaccine injury” David Gorski, Oct 8 ’12
- The problem of nonmedical exemptions to school vaccine mandates David Gorski, Sep 23 ’12
- Protect Yourself Mark Crislip, Sep 21 ’12
- The problem of waning pertussis immunity David Gorski, Sep 17 ’12
- Holding the Polio Vaccine Hostage Steven Novella, Jul 18 ’12
- Steve Novella vs. Julian Whitaker on vaccines at FreedomFest David Gorski, Jul 16 ’12
- Drinking from the Fire Hose: Odds and Ends on the Gasping Oppression Mark Crislip, Apr 6 ’12
- Whooping Cough Epidemic Steven Novella, Apr 4 ’12
- Autism prevalence: Now estimated to be one in 88, and the antivaccine movement goes wild David Gorski, Apr 2 ’12
- Anti-anti-vax: Getting to the gist Scott Gavura, Mar 29 ’12
- California Bill AB 2109: The Antivaccine Movement Attacks School Vaccine Mandates Again David Gorski, Mar 26 ’12
- An antivaccine tale of two legal actions David Gorski, Mar 12 ’12
- SANE Vax adopts Dr. Hanan Polansky’s “microcompetition” as its own. Hilarity ensues. David Gorski, Feb 20 ’12
- Ringing in 2012 with…antivaccine propaganda? David Gorski, Dec 28 ’11
- What Is an Antivaxer? Steven Novella, Dec 28 ’11
- Vaccination mandate exemptions: gimme that ol’ time philosophy Jann Bellamy, Dec 15 ’11
- HPV Vaccine for Boys Harriet Hall, Nov 22 ’11
- Pediatrics & “CAM” II: just wrong Jann Bellamy, Dec 1 ’11
- The Greater Good: Pure, unadulterated anti-vaccine propaganda masquerading as a “balanced” documentary David Gorski, Nov 7 ’11
- Pox parties taken to the next (illegal) level David Gorski, Nov 6 ’11
- Random Flu Thoughts Mark Crislip, Nov 4 ’11
- Return of an old foe Peter Lipson, Nov 1 ’11
- Alternative Vaccination Schedules Mark Crislip, Oct 21 ’11
- Quoth the anti-vaccine group SANE Vax: Beware HPV DNA in Gardasil! David Gorski, Sep 8 ’11
- Varicella Vaccination Program Success Steven Novella, Jul 27 ’11
- On the Orwellian language and bad science of the anti-vaccine movement: “SmartVax” versus “MaxVax”? David Gorski, Jul 25 ’11
- Anti-vaccine propaganda in The Baltimore Sun David Gorski, Jul 11 ’11
- Vaccine Confidence: Attitudes and Actions Scott Gavura, Jul 7 ’11
- Another Anti-Vaccine Book Harriet Hall, Jun 7 ’11
- Anti-vaccine warriors vs. research ethics David Gorski, Jun 2 ’11
- Measles outbreaks, 2011 David Gorski, May 30 ’11
- Smallpox and Pseudomedicine Kimball Atwood, May 27 ’11
- When you can’t win on science, invoke the law… David Gorski, May 11 ’11
- Vaccines and infant mortality rates: A false relationship promoted by the anti-vaccine movement David Gorski, May 9 ’11
- “Motivated reasoning,” alternative medicine, and the anti-vaccine movement David Gorski, May 2 ’11
- The curious case of Poul Thorsen, fraud and embezzlement, and the Danish vaccine-autism studies David Gorski, Apr 25 ’11
- Anti-vaccine propaganda from Sharyl Attkisson of CBS News David Gorski, Apr 4 ’11
- Triskaidekaphobia times two. Mark Crislip, Mar 11 ’11
- Supreme Court Saves Nation’s Immunization Program John Snyder, Feb 24 ’11
- Vaccination as “rape”: Meryl Dorey and the Australian Vaccination Network Rachael Dunlop, Feb 19 ’11
- The Flu Vaccine and Narcolepsy Steven Novella, Feb 9 ’11
- Mothering magazine: Peddling dangerous health misinformation to new mothers David Gorski, Jan 10 ’11
- “Piltdown medicine” and Andrew Wakefield’s MMR vaccine fraud David Gorski, Jan 6 ’11
- Deadly Choices about vaccination David Gorski, Jan 3 ’11
- Vaccines are a pain: What to do about it Scott Gavura, Dec 23 ’10
- Freeways, autism, and correlation versus causation David Gorski, Dec 20 ’10
- Ososillyococcinum and other Flu bits. Mark Crislip, Dec 17 ’10
- Be thankful: No anti-vaccine propaganda at the movies this weekend David Gorski, Nov 25 ’10
- Improving Our Response to Anti-Vaccine Sentiment Scott Gavura, Nov 6 ’10
- Homeopathic Vaccines. Mark Crislip, Nov 5 ’10
- A Shot in the Dark Revisited Steven Novella, Nov 3 ’10
- Journal Club Debunks Anti-Vaccine Myths Harriet Hall, Nov 2 ’10
- What does “anti-vaccine” really mean? David Gorski, Nov 1 ’10
- High Dose Flu Vaccine for the Elderly Harriet Hall, Oct 19 ’10
- Joe Mercola and Barbara Loe Fisher declare November 1-6, 2010 “Vaccine Awareness Week”? Not so fast! David Gorski, Oct 18 ’10
- Some Flu Vaccine Updates Steven Novella, Oct 6 ’10
- When (Anti-Vax) Politics Intrudes Steven Novella, Sep 29 ’10
- Using attacks on science by the anti-vaccine movement as a “teachable moment” David Gorski, Sep 20 ’10
- The final nail in the mercury-autism hypothesis? David Gorski, Sep 13 ’10
- A pox on your bank account: failure to vaccinate and its legal consequences Jann Bellamy, Aug 27 ’10
- How to make a difference – Responsible vaccine advocacy Joseph Albietz, Aug 20 ’10
- Pertussis Epidemic 2010 Steven Novella, Aug 18 ’10
- Terrible Anti-Vaccine Study, Terrible Reporting Steven Novella, Jul 16 ’10
- Shingles Vaccine (Zostavax) Confirmed Safe Harriet Hall, Jul 6 ’10
- Medical Voices: Always in Error, Never in Doubt Mark Crislip, Jun 18 ’10
- The genetics of autism David Gorski, Jun 14 ’10
- Mumps Mark Crislip, Jun 4 ’10
- Nine differences between “us and them,” nine straw men burning David Gorski, May 31 ’10
- Andrew Wakefield Fights Back Harriet Hall, May 28 ’10
- Stand up for science-based medicine against anti-vaccine fear mongering in Chicago today David Gorski, May 26 ’10
- Autism One: The yearly antivaccine autism “biomed” quackfest begins David Gorski, May 24 ’10
- “Medical Voices” on vaccines: Brave, brave Sir Robin… David Gorski, May 20 ’10
- Nine Questions, Nine Answers. Mark Crislip, May 7 ’10
- Dr. Jay Gordon: Full of sound and fury, signifying nothing Joseph Albietz, Apr 30 ’10
- The Vaccine War David Gorski, Apr 29 ’10
- The Other Anti-Vaccinationists Steven Novella, Apr 28 ’10
- Social Factors in Autism Diagnosis Steven Novella, Apr 14 ’10
- Steven Higgs: Another antivaccine reporter like Dan Olmsted in the making? David Gorski, Apr 12 ’10
- Outbreaks Mark Crislip, Apr 9 ’10
- Mercola, Gardasil, and Toyota? Joseph Albietz, Apr 2 ’10
- “Vaccines didn’t save us” (a.k.a. “vaccines don’t work”): Intellectual dishonesty at its most naked David Gorski, Mar 29 ’10
- Vaccinations and autism: are we number 1? Peter Lipson, Mar 25 ’10
- J.B. Handley and the anti-vaccine movement: Gloating over the decline in confidence in vaccines among parents David Gorski, Mar 22 ’10
- Just the Facts Mark Crislip, Mar 12 ’10
- A Welcome Upgrade to a Childhood Vaccine – PCV 13 Joseph Albietz, Mar 5 ’10
- The fall of Andrew Wakefield David Gorski, Feb 22 ’10
- Autism Onset and the Vaccine Schedule – Revisited Steven Novella, Feb 19 ’10
- The General Medical Council to Andrew Wakefield: “The panel is satisfied that your conduct was irresponsible and dishonest” David Gorski, Feb 1 ’10
- You can’t hide in the herd Joseph Albietz, Jan 22 ’10
- The anti-vaccine movement strikes back against Dr. Paul Offit David Gorski, Jan 4 ’10
- Measles Mark Crislip, Dec 18 ’09
- An Influenza Recap: The End of the Second Wave Joseph Albietz, Dec 11 ’09
- Yet another nail in the coffin of the myth that the MMR vaccine causes autism David Gorski, Dec 7 ’09
- A temporary reprieve from legislative madness John Snyder, Dec 2 ’09
- Naturopaths and the anti-vaccine movement: Hijacking the law in service of pseudoscience David Gorski, Nov 30 ’09
- Why Universal Hepatitis B Vaccination Isn’t Quite Universal Joseph Albietz, Nov 27 ’09
- The autism “biomed” movement: Uncontrolled and unethical experimentation on autistic children David Gorski, Nov 23 ’09
- Yes, But. The Annotated Atlantic. Mark Crislip, Nov 7 ’09
- J.B. Handley of the anti-vaccine group Generation Rescue: Misogynistic attacks on journalists who champion science David Gorski, Oct 31 ’09
- A Not-So-Split Decision John Snyder, Oct 26 ’09
- An epidemic of fear: The anti-vaccine movement’s war on science David Gorski, Oct 20 ’09
- “Oh, come on, Superman!” (Part II): Bill Maher meets Kryptonite over vaccines and “Western medicine” David Gorski, Oct 19 ’09
- More Nonsense from Dr. Jay Gordon Steven Novella, Oct 15 ’09
- H1N1 Update Steven Novella, Oct 14 ’09
- Flu Vaccine Efficacy Mark Crislip, Oct 9 ’09
- Monkey business in autism research, part II David Gorski, Oct 8 ’09
- Confusing correlation with causation David Gorski, Oct 3 ’09
- The price of anti-vaccine fanaticism: Case histories David Gorski, Sep 28 ’09
- The HPV Vaccine (Gardasil) Safety Revisited Joseph Albietz, Sep 18 ’09
- Even with the H1N1 pandemic flu strain going around, you should still be vaccinated against the seasonal flu David Gorski, Sep 17 ’09
- More Flu Woo For You, Boo Boo Mark Crislip, Sep 11 ’09
- Swine Flu Vaccine Fearmongering Harriet Hall, Sep 8 ’09
- Vaccines and the Media: No Room for Balance John Snyder, Sep 2 ’09
- The perils and pitfalls of doing a “vaccinated versus unvaccinated” study David Gorski, Aug 24 ’09
- A Defense of Childhood Influenza Vaccination and Squalene-Containing Adjuvants; Joseph Mercola’s “Dirty Little Secret” Joseph Albietz, Aug 21 ’09
- Cashing In On Fear: The Danger of Dr. Sears John Snyder, Jul 30 ’09
- Vaccines and Autism: A Deadly Manufactroversy Harriet Hall, Jun 9 ’09
- Herd Immunity Mark Crislip, Jun 5 ’09
- Will The Real, Silent Majority Please Stand Up – To Oprah and Jenny McCarthy? Val Jones, Jun 4 ’09
- Should Vaccines Be Compulsory? Steven Novella, Jun 3 ’09
- The Oprah-fication of medicine David Gorski, Jun 1 ’09
- Does the Flu Vaccine Increase Hospitalizations? Steven Novella, May 27 ’09
- Chemical castration for autism: After three years, the mainstream media finally notices David Gorski, May 25 ’09
- Hostility Towards Scientists And Jenny McCarthy’s Latest Video Val Jones, May 21 ’09
- Georgia on my mind John Snyder, May 6 ’09
- 14 Studies Later Mark Crislip, Apr 24 ’09
- J.B. Handley, Generation Rescue, and attacks on critics David Gorski, Apr 23 ’09
- More on Fourteen Studies Steven Novella, Apr 15 ’09
- Generation Rescue, the anti-vaccine propaganda machine, and “Fourteen Studies” David Gorski, Apr 13 ’09
- The Jenny and Jim antivaccine propaganda tour has begun David Gorski, Apr 6 ’09
- In Jenny McCarthy’s Own Words David Gorski, Apr 1 ’09
- Pockets of Vaccine Noncompliance in California Steven Novella, Apr 1 ’09
- Where’s The Outrage? John Snyder, Mar 26 ’09
- The Incredible Shrinking Vaccine-Autism Hypothesis Shrinks Some More David Gorski, Mar 2 ’09
- 2009: Shaping Up to be a Really Bad Year for Antivaccinationists David Gorski, Feb 23 ’09
- Antivaccine hero Andrew Wakefield: Scientific fraud? David Gorski, Feb 8 ’09
- Since when did an apologist for the antivaccination movement, Dr. Jay Gordon, become an “expert” in vaccine law? David Gorski, Feb 2 ’09
- More Data on Vaccine Safety Amid New Outbreaks Steven Novella, Jan 28 ’09
- The Alleged Autism Epidemic Steven Novella, Jan 14 ’09
- Animal Vaccinations David Ramey, Jan 11 ’09
- Paul Offit Takes on Robert Sears Steven Novella, Jan 7 ’09
- The $150,000 Vaccine Challenge Harriet Hall, Dec 30 ’08
- Influenza Deaths Mark Crislip, Dec 19 ’08
- “I Reject Your Reality” – Germ Theory Denial and Other Curiosities Harriet Hall, Dec 9 ’08
- Dr. Jay Gordon – “Anti-Vaccination” Steven Novella, Dec 3 ’08
- The Infection Schedule vs the Vaccination Schedule Mark Crislip, Nov 21 ’08
- “It’s Just A Theory” Mark Crislip, Nov 7 ’08
- Dr. Jay Gordon and me: Random encounters with an apologist for the antivaccine movement David Gorski, Oct 20 ’08
- When Compassion Outshines Ignorance Peter Lipson, Oct 20 ’08
- Autism’s False Prophets Revealed David Gorski, Sep 29 ’08
- Sometime Ethics and Science Win Out David Gorski, Sep 18 ’08
- Yet Another Study Fails to Find a Link Between the MMR Vaccine and Autism David Gorski, Sep 8 ’08
- Thanks, Jenny McCarthy! Thanks for the Measles David Gorski, Aug 24 ’08
- Peruvian Hamsters and Autism: Cui Bono? Harriet Hall, Aug 19 ’08
- Amanda Peet Is My Hero Mark Crislip, Aug 14 ’08
- Autism and Vaccines: Responding to Poling and Kirby Steven Novella, Jul 23 ’08
- When Investigative Reporting Becomes Anti-Vaccine Propaganda David Gorski, Jul 14 ’08
- Should We Study Chelation for Autism? Steven Novella, Jul 9 ’08
- Why the Latest Geier & Geier Paper is not Evidence that Mercury in Vaccines Causes Autism David Gorski, Jun 16 ’08
- Jenny McCarthy, Jim Carrey, and “Green Our Vaccines”: Anti-vaccine, not “pro-safe vaccine” David Gorski, Jun 9 ’08
- The Media and Vaccines Steven Novella, May 28 ’08
- Monkey Business in Autism Research David Gorski, May 19 ’08
- Mercury Emissions from Coal-Burning Power Plants and Autism: Is There a Connection? David Gorski, May 5 ’08
- The Increase in Autism Diagnoses: Two Hypotheses Steven Novella, Apr 16 ’08
- The Hannah Poling case and the rebranding of autism by antivaccinationists as a mitochondrial disorder David Gorski, Mar 10 ’08
- Toxic Myths About Vaccines David Gorski, Feb 18 ’08
- Mercury in vaccines as a cause of autism and autism spectrum disorders ASDs): A failed hypothesis (David Gorski, Jan 7 ’08
Outside Resources about Vaccines & Autism
- Anti-Anti-Vax (Todd W.)
- The Anti-Vaccine Movement (Steven Novella, November 2007)
- Autism Watch (Edited by James R. Laidler, M.D.)
- Brian Deer’s investigation of Andrew Wakefield
- Every Child by Two – Vaccine Safety Page
- Fear Not: Vaccines Do Not Cause Autism (Steven Novella, June 2005)
- Institute of Medicine – Immunization Safety Review: Vaccines and Autism (May 17 2004)
- Thimerosal and Autism (Paul Offit)
- Vaccines & Autism: A Dangerous Manufactroversy (Harriet Hall, June 2009)
- Why Does the Vaccine/Autism Controversy Live On? (Chris Mooney, June 2009)
Summary of Key Research about Vaccines & Autism
MMR and Autism
Wakefield AJ, et al. Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. The Lancet, Volume 351, Issue 9103, Pages 637 – 641, 28 February 1998 doi:10.1016/S0140-6736(97)11096-0
Summary: This is the original Lancet article by Andrew Wakefield that spawned the MMR-autism scare. The study is a small analysis of 12 subjects that Wakefield claims had evidence of the measles virus in their GI tract and that this correlated with the MMR vaccine and the onset of autism. This study has subsequently been discredited on a number of levels. It turns out that Wakefield had undisclosed conflicts of interest – namely a patent application for a replacement MMR vaccine. He was also a consultant for an attorney looking to sue the manufacturers of the MMR vaccine, and in fact many of the subjects of this study were childen of clients of this attorney. The techniques used to identify measles virus in the GI tracts were later disputed and failed to replicate. Review of records also disputes the timing of the onset of symptoms and the MMR vaccine. The scandals surrounding this study eventually led to 10 of the original 12 co-authors to retract their support for the paper. (For a more detailed history and analysis see Brian Deer’s investigation.)
Afzal M A, et al. Absence of measles-virus genome in inflammatory bowel disease. The Lancet 1998; 351: 646-7.
Summary: The Lancet published a research letter by Afzal et al., in response to Wakefield et al.’s earlier papers published in the Journal of Medical Virology (39:345-53, 1993 and 51:90-100, 1997) describing the presence of measles virus in Crohn’s and ulcerative colitis tissues. They concluded that using the best available polymerase chain reaction ( PCR ) technology, they were unable to find measles virus genome in gut mucosal biopsies from patients with Crohn’s disease or ulcerative colitis.
Chen R, Destefano F. Vaccine adverse events: causal or coincidental? The Lancet 1998; Vol 351: 611-12.
Summary: Commentary that highlights vaccines are given to millions of healthy people, usually infants, and that extremely high standards for vaccine safety are demanded. It’s important that the report by Wakefield of several children whose chronic bowel and behavioral abnormalities were linked by their parents and physicians to measles, mumps, and rubella (MMR) vaccination are examined, critically and with an open mind. The commentary also highlights that vaccine-safety concerns such as that reported by Wakefield and colleagues; “may snowball into societal tragedies when the media and the public confuse association with causality and shun immunization. This painful history was shared by the UK (among others) over pertussis in the 1970s after another similar case- series was widely publicized,and it is likely to be repeated all too easily over MMR. This would be tragic because passion would then conquer reason and the facts again in the UK.”
Fombonne E. Inflammatory bowel disease and autism, The Lancet: Research Letters 1998; Vol 351: 955.
Summary: Research letter published in The Lancet on 28th March 1998, written by Eric Fombonne that suggests no particular association between Crohn’s disease and autism among children immunised with MMR.
Kiln M. Autism, inflammatory bowel disease, and MMR Vaccine, The Lancet- Research Correspondence 1998; Vol 351: 1358.
Summary: Correspondence published in The Lancet, written by MR Kiln. Highlights that Wakefield and colleagues’ report did not show an established link between MMR vaccine and autism, and that health professionals and parents should have even more, not less, confidence in the safety of present MMR vaccine and the benefits of vaccination.
Mrozek-Budzyn D; Kieltyka A; Majewska R Lack of Association Between Measles-Mumps-Rubella Vaccination and Autism in Children: A Case-Control Study. The Pediatric Infectious Disease Journal: 1 December 2009. doi: 10.1097/INF.0b013e3181c40a8a
Summary: This is a retrospective case-control study conducted in Poland that found no correlation between autism and either the single measles vaccine or the trivalent MMR vaccine. In fact, there appeared to be a protective effect in that there was less autism in those who were vaccinated. This is likely either a random result or the result of an unknown confounder. However, this study does not reflect any increased risk of autism in those receiving either type of vaccine.
Peltola H, Patja A, Leinikki P, et al. No evidence for measles, mumps, and rubella vaccine-associated inflammatory bowel disease or autism in a 14-year prospective study. Lancet, May 2 1998, 351(9112) p1327-8.
Summary: This study showed that, with over a decade’s effort to detect all severe adverse events associated with MMR vaccine, no data could be found supporting the hypothesis that it would cause pervasive developmental disorder or inflammatory bowel disease.
- 3 million doses of MMR between 1982-1996 in Finland
- Follow-up interval = 1y4m – 15y5m (mean 10y8m)
- 31 children developed GI symptoms (30 after the first dose).
- Time interval between MMR and symptoms = 20h – 15d
- 1 episode of Guillain-Barré syndrome
- 5 children had febrile seizures
- 2 children had headaches
- No cases of autism were reported
Taylor B, Miller E, Farrington CP, Petropoulos MC, Favot-Mayaud I, Li J, Waight PA. Autism and measles, mumps, and rubella vaccine: no epidemiological evidence for a causal association. Lancet. 1999;353:2026-9.
Summary: This population-based study investigated whether there was an association between the incidence of autism and MMR immunization in the North-East Thames region. This study confirmed that there was an increase in the prevalence of autism but this increase was not related to the introduction of MMR or to vaccine coverage. This study did not identify any association between MMR vaccine and the age of diagnosis of autism. The results of this paper do not support a causal association between MMR and autism, either in its initiation or the onset of regression.
Fombonne E. Are measles infections or measles immunizations linked to autism? Ask the Editor Journal of Autism and Developmental Disorders (August 1999) Vol 29:No 4:1999
Summary: Letter in the Journal of Autism and Developmental Disorders that examines whether measles infections or measles immunisations are linked to autism. The letter concludes that no evidence exists to causally link exposures to measles virus or vaccination and autism.
Afzal A, et al. Further evidence of the absence of measles virus genome sequence in full thickness intestinal specimens from patients with Crohn’s disease. Journal of Medical Virology 2000; 62: 377-82.
Patja A, et al. Serious adverse events after measles-mumps-rubella vaccination during a fourteen-year prospective follow-up. Pediatric Infectious Diseases Journal. 2000; 19(12):1127–34.
Summary: This study concluded that causality between immunisation and a subsequent untoward event cannot be estimated solely on the basis of a temporal relation. Comprehensive analysis of the reported adverse reactions established that serious events causally related to MMR vaccine are rare and greatly outweighed by the risks of natural MMR diseases.
Medicines Control Agency/Department of Health (2001) Combined measles, mumps and rubella vaccines: Response of the Medicines Control Agency and the Department of Health to issues raised in papers published in Adverse Drug Reactions and Toxicological Reviews 2000 19(4).
Summary: The Medicines Control Agency and Department of Health carried out a systematic review of the Wakefield & Montgomery paper and found serious errors in it, such as incorrect analysis of trial results, incorrect reporting of the length and detail of studies and a failure to identify and analyse all the evidence.
Committee on Safety of Medicines (2001). Summary of the Committee on Safety of Medicines meeting held 10 January 2001.
Summary: The Committee on Safety of Medicines reviewed the Wakefield & Montgomery paper and concluded: ‘In those studies where MMR has been compared with the component vaccines there is no suggestion that MMR causes more adverse effects than measles vaccines alone.’
World Health Organization (2001). Statement on the use of MMR vaccine 24 January 2001
Summary: The World Health Organization (WHO) released its view of the evidence regarding the safety of the MMR vaccine. It stated: ‘WHO strongly endorses the use of MMR vaccine on the grounds of its convincing record of safety and efficacy. The combination vaccine is recommended rather than the monovalent presentation when available and the disease burden justifies its use. There has been no new scientific evidence that would suggest impaired safety of MMR. On the contrary, all results from vaccine trials published reaffirm the high safety of MMR vaccine.’
Kaye J, del Mare Melero-Montes M, Jick H. Mumps, measles and rubella vaccine and the incidence of autism recorded by general practitioners: A time trend analysis. British Medical Journal 2001 322:460-3.
Summary: Used the GP Research Database to compare MMR vaccine coverage over time with reported rates of autism. Risk of autism increased fourfold in the UK between 1988 and 1999.
Uptake of MMR more or less constant at ~ 95%The authors concluded that ‘the data provided evidence that no correlation exists between the prevalence of MMR vaccination and the rapid increase in the rise of autism over time.’
De Wilde S, Carey IM, Richards N, et al. Do children who become autistic consult more often after MMR vaccination? Br J Gen Pract (England), Mar 2001, 51(464) p226-7.
Summary: The Doctor’s Independent Network database was used to examine whether children subsequently diagnosed as autistic consulted more frequently than controls after MMR vaccination. No difference in consulting behaviour was seen in the six months post MMR. Any dramatic effect of MMR on behaviour seems unlikely.
Dales L, Hammer SJ, Smith NJ Time trends in autism and in MMR immunization coverage in California. JAMA, Mar 7 2001, 285(9) p1183-5.
Summary: Percentage of children immunized with MMR between 1980 and 1994 was compared with incidence of autism during same period. Although a dramatic increase in autism incidence was found, the percentage of children that received MMR was unchanged. Conclusion: No causal association exists between MMR vaccination and the risk of autism.
Davis R L, et al. Measles-mumps-rubella and other measles-containing vaccines do not increase the risk for inflammatory bowel disease. Archives of Pediatrics and Adolescent Medicine 2001 155:354-9.
Summary: Findings from the University of Washington in Seattle which showed that MMR, or other vaccines containing the measles virus, do not increase the risk of inflammatory bowel diseases, such as Crohn’s disease.
Institute of Medicine Immunisation Safety Review Committee (2001). Report of measles-mumps-rubella vaccine and autism.
Summary: The US Institute of Medicine Immunisation Safety Review Committee published a report which concluded: ‘The evidence favours rejection of a causal relationship at the population level between MMR vaccine and autistic spectrum disorders (ASD).’ The chair of the committee warned of possible ‘devastating disease outbreaks’ if parents refrained from having their children vaccinated due to autism fears.
Halsey N A., et al. Measles-Mumps-Rubella Vaccine and Autistic Spectrum Disorder: Report From the New Challenges in Childhood Immunizations Conference Convened in Oak Brook, Illinois, June 12-13, 2000. Pediatrics 2001; 107: 84.
Summary: The American Academy of Pediatrics hosted a multidisciplinary international workshop to review the evidence regarding a possible association between MMR vaccine, inflammatory bowel disease and autism spectrum disorders, specifically autism with regression. It decided a considerable body of evidence did not support a causal relationship between MMR vaccine and autism or inflammatory bowel disease. In addition, it found no data to suggest the separate administration of measles, mumps and rubella vaccines would offer any potential benefit over the MMR vaccine. In fact, it voiced its concern that such an approach would result in many under-immunised children.
Farrington P., et al. MMR and autism: Further evidence against a causal association. Vaccine 2001; 19:3632-5.
Summary: Re-examined previous research, published in The Lancet, which examined signs of autism in children shortly after they received the combined vaccine. Following criticism that the onset of autism may not necessarily be short, the new research looked at the data from the same 357 autistic children who had taken part in the first study but used an extended timescale. The results provided further evidence against a causal association between the MMR vaccine and autism.
Elliman D, Bedford H, Miller E. MMR vaccine: Worries are not justified. Archives of Disease in Childhood 2001; 85:271-4.
Summary: A review of evidence on MMR to date by Elliman and Bedford. It concluded that there is neither experience nor research evidence for giving the triple vaccine separately anywhere in the world. There is no case for introducing single vaccines and worries over MMR are unjustified.
Frombonne E; Chakrabarti S No Evidence for A New Variant of Measles-Mumps-Rubella-Induced Autism. Pediatrics 2001; Oct 108;4(e58):991.
Summary: Compares autistic children who have had MMR to those who have not. It failed to support an association between MMR and regressive autism and concluded that, when combined, current findings did not argue for changes in current immunisation programmes and recommendations.
Spitzer W, Aitken K, et al. The natural history of autistic syndrome in British children exposed to MMR. Adverse Drug Reaction Toxicological Review 2001; 20 (3): 160-3.
Summary: Paper reviews children whose parents are taking legal action against drug manufacturers. It stated that the first symptoms of autism appear over a year after the MMR vaccine and claimed prior research is invalid. However, it provided no evidence to link MMR to autism and the authors failed to produce any scientific references.
Dales L, Hammer SJ, Smith NJ. Time trends in autism and in MMR immunization coverage in California. JAMA 2001; 285: 1183–1185.
Farrington CP, Miller E, Taylor B. MMR and autism: further evidence against a causal association. Vaccine 2001; 19: 3632–3635.
Smeeth L, Hall AJ, Fombonne E, Rodrigues LC, Huang X, et al. A case-control study of autism and mumps-measles-rubella vaccination using the general practice research database: design and methodology. BMC Public Health 2001; 1:2.
Takahashi H, Arai S, Tanaka-Taya K, Okabe N. Autism and infection/immunization episodes in Japan. Jpn J Infect Dis 2001; 54: 78–79.
Medical Research Council Review of autism research (December 2001)
Summary: The Medical Research Council (U.K.) published a review on autism, which stated that understanding and diagnosis of autism spectrum disorders (ASDs) has improved and called for more research in this area. It also stated that in relation to MMR, current evidence does not support the alleged link of MMR and ASDs.
Taylor B, et al. Measles, mumps and rubella vaccination and bowel problems or developmental regression in children with autism: a population study. BMJ 2002. 324:393-6.
Scottish Executive – MMR Report
Summary: Report of the expert group established by the Scottish Executive in response to recommendations set out in the health and community care committee’s report of the inquiry into issues surrounding the alleged relationship between the combined measles, mumps and rubella vaccine and autism.
A PDF of this report is available at: www.scotland.gov.uk/library5/health/rmmr.pdf
Black C, Kaye JA, Jick H. Relation of childhood gastrointestinal disorders to autism: nested case-control study using data from the UK General Practice Research Database. British Medical Journal 2002;325:419-21.
Summary: This study, using the General Practice Research Database, looked at whether children with autism are more likely to have a history of gastrointestinal disorders than children without autism. All children born between 1 January 1988 and 31 December 1999 were reviewed. The study concluded there was ‘no evidence that children with autism were more likely than children without autism to have had defined gastrointestinal disorders at any time before their diagnosis of autism.’
Madsen KM, et al. A population-based study of measles, mumps and rubella vaccination and autism. New England Journal of Medicine 2002; 347: 1477-82.
Summary: A retrospective cohort study published in the New England Journal of Medicine reviewed over 500,000 children born in Denmark. The main objective of this study was to evaluate whether there was an association between MMR vaccine and autism. This paper concluded ‘This study provides strong evidence against the hypothesis that MMR vaccination causes autism.’
Mäkëla, et al. Neurologic disorders after measles-mumps-rubella vaccination. Pediatrics 2002; 110:957-63.
Summary: A further study was published in the journal Pediatrics. The aim of this study was to assess whether there was an association between MMR vaccination and encephalitis, aseptic meningitis, and autism. This retrospective record linkage study in Finland looked at over 500,000 children aged between 1 and 7 years of age vaccinated during November 1982 and June 1986. This study did not identify any association between MMR vaccination and encephalitis, aseptic meningitis or autism.
Thjodleifsson B., et al. Inflammation and inflammatory bowel disease. Effect of Pentavac and measles-mumps-rubella (MMR) vaccination on the intestine. Gut 2002; 51:816-17.
Summary: A paper investigating whether MMR vaccination was associated with the development of ‘autistic enterocolitis’ in Iceland was published. Infants were reviewed before, and 2 and 4 weeks after immunisation with Pentavac for the presence of intestinal inflammation. This paper did not find any evidence of intestinal inflammation during the 4 weeks following MMR or Pentavac immunisation.
Andrews N. et al. Short Report. Recall bias, MMR and autism. Archives of Diseases in Children 2002; 87:493-4.
Summary: Examines the effect of prior knowledge of a suggested causal link between MMR and autism on the parents’ perception of a temporal association between immunisation and onset of symptoms (particularly regression). This paper highlights that there is a significant degree of recall bias in parents of autistic children with regressive features who were diagnosed after the publicity alleging a link between MMR and autism.
Szatmari P. et al. The cause of autism spectrum disorders. British Medical Journal 2003;326: 173-4.
Summary: The possible causes of autism spectrum disorders are reviewed in a recent paper by Prof P. Szatmari. This review highlights the importance of genetic factors but points out that environmental factors cannot be excluded. In this review he states that ‘Despite recent publicity, there is good evidence that the measles, mumps and rubella vaccine is not an environmental risk fact for autism.’
Yeargin-Allsopp M. et al. Original contribution. Prevalence of autism in a US metropolitan area. Journal of American Medical Association 2003;289 (1): 49-55.
Summary: Reported on the prevalence of autism in children aged between 3 to 10 years in 1996 in Atlanta. This paper concluded that the rate of autism in this age group was higher than the rate of autism in studies conducted in the US during the early 80s and 90s. The findings of this study were stated to be similar to more recent studies.
Fombonne E. Editorial. The prevalence of autism. Journal of American Medical Association 2003;289 (1): 87-9.
Summary: The above paper by Yeargin-Allsopp M. et al. was accompanied by an editorial by Dr E Fombonne.
Ki M. et al. Risk analysis of aseptic meningitis after measles-mumps-rubella vaccination in Korean children by using a case-crossover design. American Journal of Epidemiology 2003;157(2): 158-65.
Summary: A study examining the risk of developing aseptic meningitis following MMR vaccination in Korea was carried out. This case-crossover study was shown to be useful in confirming the risk of developing acute adverse events following vaccination. This study confirmed that there was no significant risk of developing aseptic meningitis following the Jeryl Lynn or Rubini strain of MMR. It also confirmed that the Urabe or Hoshino strain of MMR was associated with a risk increased in the third to sixth week following vaccination.
Miller E, Andrews N , Waight P , Taylor B. Bacterial infections, immune overload, and MMR vaccine. Arch Dis Child. 2003; 88:222–223
Summary: This record-linkage study looked at whether MMR vaccine increased the risk of hospitalisation with invasive bacterial infections (such as bacterial meningitis and septicaemia, and pneumonia) in the three months following vaccination. Children aged between 12-23 months admitted to hospital in selected districts in the Thames region of southern England with a bacterial invasive disease between April 1995 and March 1995 were reviewed. This study excluded any children predisposed to developing bacterial infection such as those immunosuppressed. The results of this study showed that MMR did not increase the risk of developing bacterial infections within 90 days following vaccination. This study does not support the theory that MMR causes immunological overload in children.
MMR vaccine – how effective and how safe? The independent review from Consumers’ Association. Drug and Therapeutics Bulletin April 2003, 41 (4):25-30.
Summary: This paper reviews the safety, efficacy and side effects of MMR vaccine. This paper concludes that:
- MMR is a highly effective vaccine
- There is no convincing evidence that MMR vaccine causes, or facilitates development of, either inflammatory bowel disease or autism.
- There is no good reason or scientific basis to adopt an alternative policy that allows substitution of single-antigen vaccines for the combined vaccine.
- The weight of published evidence argues overwhelmingly in favour of MMR vaccine as the most effective and safest way of protecting children from measles, mumps and rubella.
Wilson K., et al. July . Association of Autistic Spectrum Disorder and the Measles, Mumps and Rubella Vaccine. Arch Pediatr Adolesc Med 2003;157: 628-34.
Summary: This article reviewed the available literature on measles, mumps and rubella vaccine and autistic spectrum disorders (ASD). A total of 12 studies (from 5 countries) examining the hypotheses put forward by Dr Wakefield and colleagues were reviewed in detail. None of the studies examined provided evidence of an association between autistic spectrum disorders and MMR. The review did not find any evidence of an epidemic of ASD related to MMR, nor evidence of an association between a variant form of autism and the MMR vaccine. The authors state that ‘Given the real risks of not vaccinating and that the risks and existence of variant ASD remain theoretical, current policies should continue to advocate the use of MMR vaccine’.
Taylor et al. Prevalence of autism and parentally reported triggers in a north east London population. Archives of Disease in Childhood 2003; 88:666-670.
Summary: The aim of this study was to estimate the prevalence of autism and to look at whether parental perception regarding the onset or causes of autism had changed over that time. The results of this study showed a levelling in the prevalence of autism from 1992 to 1996, with a rate of 2.6 per 1000 live births. They also showed that the age at diagnosis had decreased over time.
These two findings suggest that the rise previously found was not a real rise and was likely to be due to factors such as an increased recognition, greater acceptance of the diagnostic label by educationalists and families, and also better recording systems. This paper also showed that there was an increase in the number of parents attributing their child’s autism to MMR since August 1997.
DeStefano F, Thompson W. MMR Vaccine and Autism: An Update of the Scientific Evidence Expert Review of Vaccines 2004; 3(1):19-22.
Summary: Update of scientific evidence in published studies have continued not to find an increased risk of autistic spectrum disorder associated with MMR. MMR vaccine also has not been found to be associated with a unique syndrome of developmental regression and gastrointestinal disorders. There is convincing evidence that MMR does not cause autism or any particular subtypes of autistic spectrum disorder.
Chen W, Landau S, Sham P, Fombonne E. Psychological Medicine. Cambridge University Press, 2004; B:543-553
Summary: Paper examines whether, in the UK, there is an increased risk of autism (AD) following exposures, in early life, to wild measles, live attenuated measles, alone or in combination as MMR, and the alteration of the mumps strain within MMR.
The paper concludes no increased risk of autism (AD) following exposures to wild measles and vaccinations with monovalent measles, and Urabe or Jeryl–Lynn variants of MMR, were detected.
Smeeth, et al. MMR vaccination and pervasive developmental disorders: a case-control study. The Lancet,. 2004; 364:963-969.
Summary: Case-control study of 1294 cases and 4469 age and sex matched controls to determine if there is an association between MMR vaccination and development of PDD. Conclusion: MMR not associated with increased risk of PDD.
Barbaresi, et al. The Incidence of Autism in Olmsted County, Minnesota, 1976-1997. Archives of Pediatric and Adolescents Medicine. 2005; 159:37-44.
Summary: Recent studies suggest that the number of children diagnosed with autism has increased. The cause of this increase, as yet is unknown, but better recognition and changes in classification of autistic spectrum disorders and related conditions are thought to contribute to this increase. One suggestion has been that MMR immunisation has caused this increase. There is no scientific evidence to support this hypothesis.
Miller E, Andrews N, Grant A, Stowe J, Taylor B. No evidence of an association between MMR vaccine and gait disturbance Archives of Disease in Childhood 2005;90:292-296
Summary: This study provides no evidence for a causal association between MMR and gait disturbance.
Honda H, Shimizu Y, Rutter M. 2005. No effect of MMR withdrawal on the incidence of autism: a total population study. Journal of Child Psychology and Psychiatry 46(6):572–79.
Summary: Population-based study of 300,000 in Yokohama, Japan looking at ASD diagnoses from 1988-1996. From 1988 to 1993 MMR vaccination rates declined, and there were no MMR vaccinations after 1993. Meanwhile, during the same period of time ASD diagnoses steadily increased. Therefore there was a significant lack of correlation between exposure to the MMR vaccine and the subsequent diagnosis of ASD.
Fombonne E, Zakarian R, Bennett A, Meng L, McLean-Heywood D. Pervasive developmental disorders in Montreal, Quebec, Canada: prevalence and links with immunizations. Pediatrics 2006; 118: e139–150.
Richler J, Luyster R, Risi S, Hsu WL, Dawson G, et al. Is there a ‘regressive phenotype’ of Autism Spectrum Disorder associated with the measles-mumps-rubella vaccine? A CPEA Study. J Autism Dev Disord 2006; 36: 299–316.
Afzal MA, Ozoemena LC, O’Hare A, Kidger KA, Bentley ML, et al. Absence of detectable measles virus genome sequence in blood of autistic children who have had their MMR vaccination during the routine childhood immunization schedule of UK. J Med Virol 2006;78: 623–630.
D’Souza Y, Fombonne E, Ward BJ. No evidence of persisting measles virus in peripheral blood mononuclear cells from children with autism spectrum disorder. Pediatrics 2006;118: 1664–1675.
Uchiyama T, Kurosawa M, Inaba Y. MMR-vaccine and regression in autism spectrum disorders: negative results presented from Japan. J Autism Dev Disord 2007;37: 210–217.
Baird G, Pickles A, Simonoff E, Charman T, Sullivan P, et al. Measles vaccination and antibody response in autism spectrum disorders. Arch. Dis. Child. 2008; 93:832-837.
Summary: A Case-control study community based study to test the hypothesis that measles vaccination wasinvolved in the pathogenesis of ASD as evidenced by signs ofa persistent measles infection or abnormally persistent immuneresponse shown by circulating measles virus or raised antibodytitres in MMR vaccinated children with ASD compared with controls .
No difference was found betweencases and controls for measles antibody response. There wasno dose response relationship between autism symptoms and antibodylevels. Measles virus nucleic acid was amplified by RT-PCR inPMBC from one case with autism and two typically developingchildren. There was no evidence of a differential response tomeasles virus or the measles component of the MMR in childrenwith ASD, with or without regression, and controls who had eitherone or two doses of MMR. Only one child from the control grouphad clinical symptoms of a possible enterocolitis.
Hornig M, Briese T, Buie T, Bauman ML, Lauwers G, et al. (2008) Lack of Association between Measles Virus Vaccine and Autism with Enteropathy: A Case-Control Study. PLoS ONE 3(9): e3140. doi:10.1371/journal.pone.0003140
Summary: This study replicated the original Lancet article by Andrew Wakefield that started the scare that the MMR vaccine might be associated with autism. The researchers found that there was no correlation between measles virus being found in the gut and autism, and also found no correlation between the timing of the MMR vaccine and the onset of autism or GI symptoms. (Further discussion here and here.)
Thimerosal and Autism
Andrews N, et al., Thimerosal exposure in infants and developmental disorders: a retrospective cohort study in the United Kingdom does not support a causal association. Pediatrics, 2004;114:584-591.
Summary: From the methods of this study: “A retrospective cohort study was performed using 109,863 children who were born from 1988 to 1997 and were registered in general practices in the United Kingdom that contributed to a research database.” And the results: “Only in 1 analysis for tics was there some evidence of a higher risk with increasing doses. Statistically significant negative associations with increasing doses at 4 months were found for general developmental disorders, unspecified developmental delay, and attention-deficit disorder. For the other disorders, there was no evidence of an association with thimerosal exposure.”
In other words – the researchers found a random scattering of mild positive and negative correlations between thimerosal exposure and a few neurodevelopment outcomes, with most outcomes showing no correlation. This is consistent with other studies and is essentially what we expect if thimerosal does not cause neurodevelopmental disorders. Some in the anti-vaccine camp have cherry-picked the weak association with tics, but there is no more reason to think that correlation is anything other than random noise than there is to believe that thimerosal protects against ADHD based upon this data.
Fombonne E., et al., Pervasive Developmental Disorders in Montreal, Quebec, Canada: Prevalence and Links with Immunizations. Pediatrics. 2006;118:139-150.
Summary: This is a population based study involving 27,749 children born from 1987 to 1998. The researchers calculated the total exposure to thimerosal, which dropped to zero after 1996 as thimerosal was removed from childhood vaccines in Canada at that time. They found:
The prevalence of pervasive developmental disorder in Montreal was high, increasing in recent birth cohorts as found in most countries. Factors accounting for the increase include a broadening of diagnostic concepts and criteria, increased awareness and, therefore, better identification of children with pervasive developmental disorders in communities and epidemiologic surveys, and improved access to services. The findings ruled out an association between pervasive developmental disorder and either high levels of ethylmercury exposure comparable with those experienced in the United States in the 1990s or 1- or 2-dose measles-mumps-rubella vaccinations.
Heron J, Golding J, and ALSPAC Study Team. Thimerosal exposure in infants and developmental disorders: a prospective cohort study in the United Kingdom does not support a causal association. Pediatrics. 2004;114:577-583.
Summary: This study is similar to the Andrews study, except this was prospective rather than retrospective. They followed > 14,000 children with neurological assessments from 6 to 91 months of age. As with the Andrews study they found a random scattering of mild correlations, mostly negative (meaning that thimerosal exposure was associated with a decreased risk of neurological signs or disorders) and only one positive correlation with poor pro-social behavior. These results are consistent with chance, i.e. no cause and effect between thimerosal and neurodevelopmental disorders.
The researchers conclude: “We could find no convincing evidence that early exposure to thimerosal had any deleterious effect on neurologic or psychological outcome.”
Hviid A, Stellfeld M, Wohlfahrt J, Melbye M. Association between thimerosal-containing vaccine and autism. Journal of the American Medical Association 2003;290:1763-1766.
Summary: This is yet another population-based study looking at a large number of children – this one is a Danish study comparing children vaccinated with a thimerosal-containing vaccine and the same vaccines but without thimerosal. The methods indicate:
Population-based cohort study of all children born in Denmark from January 1, 1990, until December 31, 1996 (N = 467,450) comparing children vaccinated with a thimerosal-containing vaccine with children vaccinated with a thimerosal-free formulation of the same vaccine.
The results are pretty straight-forward and entirely negative:
The risk of autism and other autistic-spectrum disorders did not differ significantly between children vaccinated with thimerosal-containing vaccine and children vaccinated with thimerosal-free vaccine.
Madsen KM, Lauritsen MB, Pedersen CB, Thorsen P, Plesner AM, Andersen PH, Mortensen PB. Thimerosal and the Occurrence of Autism: Negative Ecological Evidence From Danish Population-Based Data. PEDIATRICS Vol. 112 No. 3 September 2003, pp. 604-606
Summary: Madsen et al evaluated autism rates in Denmark from 1971 – 2000. From 1961 – 1970 children received 400 micrograms of thimerosal. From 1971-1992 they received 250 micrograms of thimerosal. After 1992 all thimerosal was removed from childhood vaccines in Denmark. The study identified 962 children with autism over this period. They found that from 1970 to 1990 there was no change in the incidence of autism. After 1990 autism rates began to increase, which was attributed to expanding diagnosis and surveillance. These numbers generally match the experience in other Western nations. (See here and here for further discussion.)
Miles JH, and Takahashi TN. 2007. Lack of association between Rh status, Rh immune globulin in pregnancy and autism. American Journal of Medical Genetics, Part A1. 143(13):1397–407.
Summary: Given the lack of association between vaccine exposure, thimerosal exposure, and autism spectrum disorder (ASD), proponents of the mercury- autism hypothesis have blamed possible exposure by the mother to thimerosal exposure during pregnancy. Rh- mothers may be treated with Rhig which may be preserved with thimerosal. This study looked at 305 mothers with children on the autism spectrum and compared them to general population. They found so significant difference in the risk of being Rh- or having been exposed to thimerosal in mothers with ASD children compared to the general population. Therefore exposure to thimerosal during pregnancy does not appear to be associated with ASD.
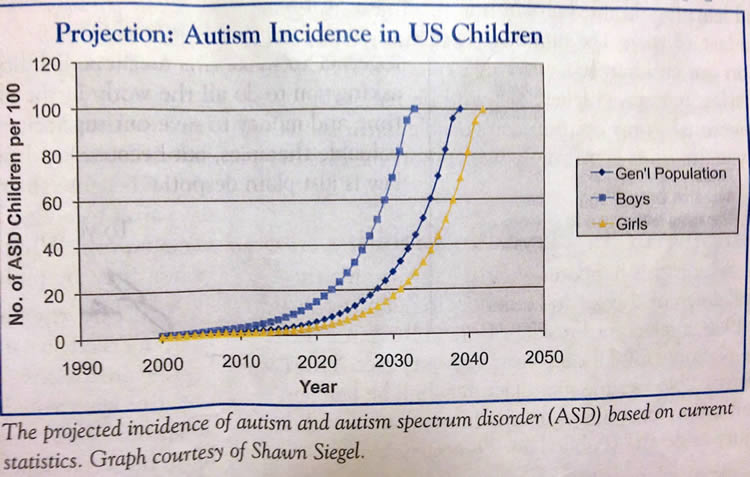
Schechter R, Grether JK. Continuing Increases in Autism Reported to California’s Developmental Services System: Mercury in Retrograde. Arch Gen Psychiatry. 2008;65(1):19-24.
Summary: The data presented in this study is the most definitive evidence against an association between thimerosal in vaccines and autism. It shows that after all but trace amounts of thimerosal were removed from the routine childhood vaccine schedule (although remaining in some optional flu vaccines), the rate of autism diagnoses did not decrease, as predicted by vaccine-autism proponents. This is especially significant because this is the same database used by proponents to argue that the increase in the rate of autism in the 1990s correlated with an increase in the vaccine schedule and the total thimerosal exposure.
The graph below (click to enlarge) shows the steady increase in the rate of autism diagnoses (by birth year) long after the removal of thimerosal from the vaccine schedule was completed – by the end of 2002.
Thompson WW, et al. Early Thimerosal Exposure and Neuropsychological Outcomes at 7 to 10 Years. N Engl J Med. 2007 Sep 27;357(13):1281-92.
Summary: This study enrolled 1047 children and compared their thimerosal exposure based upon immunization records to outcomes on standardized neurological testing. They found: “Among the 42 neuropsychological outcomes, we detected only a few significant associations with exposure to mercury from thimerosal. The detected associations were small and almost equally divided between positive and negative effects.” This is the expected statistical noise, occurring by chance alone. This study therefore lends strong support to a lack of association between thimerosal exposure from vaccines and neurodevelopmental disorders. (Further discussion here, here, and here.)
Tozzi AE, Bisiacchi P, Tarantino V, De Mei B, D’Elia L, Chiarotti F, Salmaso S. Neuropsychological Performance 10 Years After Immunization in Infancy With Thimerosal-Containing Vaccines. PEDIATRICS Vol. 123 No. 2 February 2009, pp. 475-482 (doi:10.1542/peds.2008-0795)
Summary: This study analyzed data from a vaccine safety study performed in 1993. They were able to compare two groups randomized to different pertussis vaccines with either low dose (62.5 µg) or a higher dose (137.5 µg) of thimerosal ten years later. They found no difference in autism rates between the two groups. When they did multiple comparisons for other neurological conditions they found only two minor correlations, less than predicted by chance – so essentially the study found no significant correlation between two doses of thimerosal and neurological outcome. This evidence contradicts the belief that a similar increase in the dose of thimerosal in the US in the 1990s caused an increase in the incident of autism. (See here for further discussion of this study.)
Verstraeten T, et al., Safety of thimerosal-containing vaccines: a two-phased study of computerized health maintenance organization databases. Pediatrics 2003;112:1039-1048.
Summary: This is a 2-phase retrospective cohort study looking at a large database of children from three HMOs. The first phase looked at 124,170 children from 1992-1999 from two HMOs and found an association between thimerosal exposure and tics in the first HMO and an association between thimerosal and language delay (but not tics) at the second HMO. The second phase was of 16,717 children from 1991-1997 at a third HMO and found no significant associations. The strength of this study is that it used three independent data sets to confirm any chance associations. It found no consistent associations between thimerosal and any neurodevelopmental disorder, and it found no association at all with autism or ADHD. This is most consistent with a lack of association between thimerosal exposure and neurodevelopmental disorders, but the authors call for follow up of the inconsistent association with tics and language delay.
Autism Diagnosis, Incidence and Prevalence
Bishop DV, Whitehouse AJ, Watt HJ, Line EA. Autism and diagnostic substitution: evidence from a study of adults with a history of developmental language disorder. Dev Med Child Neurol. 2008 Mar 31
Summary: This study set out to test the hypothesis that the increase in the rate of autism diagnoses is caused in part by diagnostic substitution – meaning that in the past what is now diagnosed as autism would have been given a different label. They looked at 38 adults aged 15-31 who had been diagnosed with developmental language disorder and found:
“Eight individuals met criteria for autism on both instruments, and a further four met criteria for milder forms of autistic spectrum disorder. Most individuals with autism had been identified with pragmatic impairments in childhood. Some children who would nowadays be diagnosed unambiguously with autistic disorder had been diagnosed with developmental language disorder in the past. This finding has implications for our understanding of the epidemiology of autism.”
This and other evidence supports the conclusion that there is no true autism epidemic, just a change in diagnostic practices.
Chakrabarti S, Fombonne E. Pervasive developmental disorders in preschool children: confirmation of high prevalence. Am J Psychiatry. 2005 Jun;162(6):1133-41.
Fombonne E. Epidemiology of autistic disorder and other pervasive developmental disorders. J Clin Psychiatry. 2005;66 Suppl 10:3-8.Click here to read
Jick H, Kaye JA. Epidemiology and possible causes of autism. Pharmacotherapy. 2003 Dec;23(12):1524-30.
Mitchell, S., J. Brian, L. Zwaigenbaum, W. Roberts, P. Szatmari, I. Smith, and S. Bryson. 2006. Early language and communication development of infants later diagnosed with autism spectrum disorder. Journal of Developmental and Behavioral Pediatrics 27(2 Suppl):S69–78.
Summary: Many parents believe their child contracted autism from vaccines because autism is typically recognized and diagnosed around the time that many vaccines are given. However, studies are beginning to show early signs of autism, pushing the diagnosis to younger and younger ages – before many vaccines are given, and consistent with the hypothesis that autism is dominantly genetic. This study, for example, is a prospective analysis of high risk children and low risk controls and found that those later diagnosed with autism showed delayed language development as early as 12 months of age.
Rutter, M. 2005. Incidence of autism spectrum disorders: changes over time and their meaning. Acta Paediatrica 94(1):2–15.
Summary: The results speak for themselves:
“The true incidence of autism spectrum disorders is likely to be within the range of 30–60 cases per 10 000, a huge increase over the original estimate 40 years ago of 4 per 10 000. The increase is largely a consequence of improved ascertainment and a considerable broadening of the diagnostic concept. However, a true risk due to some, as yet to be identified, environmental risk factor cannot be ruled out. There is no support for the hypothesis for a role of either MMR or thimerosal in causation, but the evidence on the latter is more limited.”
Shattuck P (2006). The Contribution of Diagnostic Substitution to the Growing Administrative Prevalence of Autism in US Special Education. Pediatrics 117:1028-1037.
Summary: If true autism rates are not increasing but rather the diagnosis is being made more because of an expansion of surveillance and a broadening of the definition, then there are certain predictions that flow from that hypothesis. One prediction is that the estimated true rate is higher than the rate of diagnosis (more cases are being captured, but those cases have to be there in the first place). The second is that as autism diagnoses increase the rate of other diagnoses that autism is now being substituted for must simultaneously decrease. This study finds that these two predictions are in fact true, supporting the notion of surveillance and definition as the causes of the increase in the autism diagnosis rate.
The study concludes:
“Prevalence findings from special education data do not support the claim of an autism epidemic because the administrative prevalence figures for most states are well below epidemiological estimates. The growing administrative prevalence of autism from 1994 to 2003 was associated with corresponding declines in the usage of other diagnostic categories.”
Teitelbaum P, Teitelbaum O, Nye J, Fryman J, Maurer RG. Movement analysis in infancy may be useful for early diagnosis of autism. PNAS November 10, 1998 vol. 95 no. 23 13982-13987
Summary: This is an analysis of 17 autistic children demonstrating the presence of movement disorders as early as several month of age. The authors argue that these movement disorders are a reliable indicator of autism before the diagnosis is typically recognized by parents and formally diagnosed. They further argue that these indicators are likely present from birth. This study, combined with other video studies and head circumference data, contradicts the often made claim that vaccination correlate with the onset of autism.
Reviews
Parker SK, Schwartz B, Todd J, and Pickering LK (2004). Thimerosal-containing vaccines and autistic spectrum disorder: a critical review of published original data. Pediatrics 114:793-804.
Summary: From the abstract:
“Studies do not demonstrate a link between thimerosal-containing vaccines and ASD, and the pharmacokinetics of ethylmercury make such an association less likely. Epidemiologic studies that support a link demonstrated significant design flaws that invalidate their conclusions. Evidence does not support a change in the standard of practice with regard to administration of thimerosal-containing vaccines in areas of the world where they are used.”
Taylor, B. 2006. Vaccines and the changing epidemiology of autism. Child Care, Health, and Development 32(5):511–19.
Summary: From the abstract:
“Results: The recorded prevalence of autism has increased considerably in recent years. This reflects greater recognition, with changes in diagnostic practice associated with more trained diagnosticians; broadening of diagnostic criteria to include a spectrum of disorder; a greater willingness by parents and educationalists to accept the label (in part because of entitlement to services); and better recording systems, among other factors. The cause(s) of autism remains unclear. There is a strong genetic component which, along with prenatally determined neuro-anatomical/biochemical changes, makes any post-natal ’cause’ unlikely.
“Conclusions: There has (probably) been no real increase in the incidence of autism. There is no scientific evidence that the measles, mumps and rubella (MMR) vaccine or the mercury preservative used in some vaccines plays any part in the aetiology or triggering of autism, even in a subgroup of children with the condition.”