
{kind=link}
A commonly misunderstood aspect of autism and autism spectrum disorders (particularly by antivaccinationists and believers in the quackery known as “autism biomed”) is that autism is not a condition of developmental stasis. It is a condition of developmental delay. Autistic children can and do exhibit improvement in their symptoms simply through growth and development. However, parents who subject their children to “autism biomed” quackery of the sort championed by Jenny McCarthy and others seem to view autism as a condition of developmental stasis. That’s why they so easily and predictably attribute any improvement in their children to whatever quackery du jour they are using on them. It’s also why, in order to determine whether a given intervention in autism has any real effect, randomized controlled trials are required. Indeed, it’s not so difficult to see why, if you take into account the widespread belief that autistic children do not improve, along with parents’ imperfect human memories riddled with confirmation bias, confusing correlation with causation, and other confounders like regression to the mean, so many parents believe that “autism biomed” treatments have actually helped their children. Moreover, improvements observed in autistic children tend to be uneven, with periods of little change interspersed with periods of rapid development. Should such a period of rapid development appear after a “biomed” intervention, guess what gets the credit for the improvement?
But how much improvement is possible? Do autistic children “recover,” and, if they do, how much can they recover? The autism biomed movement is rife with stories of “recovered” children, but often, if you investigate these stories, they turn out to be less than convincing, not unlike the way that alternative medicine cancer “cure” testimonials tend not to be so impressive when examined closely. However, in the case of autism, this isn’t always the case. There are clearly children who lose their diagnosis of autism or ASD, with observations published as far back as 1970, when Rutter reported that 1.5% of adults who had been diagnosed with autism were functioning normally, while 30 years later Sigman et al reported that 17% of autistic children in their group lost their diagnosis and 10 years after that Kleinman et al reported that up to 19% of autistic children “lose their diagnosis.” The reason for this observation is hotly debated, and until fairly recently it was often assumed that these children’s recoveries were in fact not true recoveries but children who were either misdiagnosed or overdiagnosed. Such an assumption made intuitive sense because such an outcome is more likely with children diagnosed with Asperger’s disorder or pervasive developmental disorder, not otherwise specified (PDD-NOS), both of which are categories that resulted from the expansion of the diagnostic criteria for autism. Be that as it may, when you boil it all down, it is estimated that between 3% and 25% of autistic children “lose their diagnosis.” However, few of these studies explicitly address whether the social and communication abilities of these children are fully typical.
Outgrowing symptoms of autism
A recent study might help clarify what degree of recovery is and is not possible. Most of the previous studies before this have been small and did not look specifically at the outcomes people are curious about. Published in The Journal of Child Psychology and Psychiatry by Fein et al and entitled “Optimal outcome in individuals with a history of autism“, this study got some news coverage last week under titles such as “Some With Autism Diagnosis Can Overcome Symptoms, Study Finds“; “Scientists seek clues in kids who outgrow autism symptoms“; “Some children outgrow autism: study“; “Health Buzz: Can Autism Fade Over Time?“; and “Children ‘may grow out of autism’“. The authors set the stage in their introduction after surveying the literature, some of which I’ve touched on above:
Several tentative conclusions thus seem warranted based on prior research: (a) losing the ASD diagnosis is a possibility for a minority of children and, at least for some children, is not due to misdiagnosis; (b) ‘optimal outcome’ is associated with higher cognitive functioning and somewhat milder initial symptoms; (c) residual difficulties with language, attention, executive or emotional functioning may persist and need to be characterized. Definitively documenting the existence and characteristics of individuals who lose the diagnosis of autism has important implications for understanding the neurobiology of autism, the impact of intervention on functioning, and the mechanisms underlying improvement. Structural and functional imaging of this group may shed light on whether brain anatomy and function have normalized, or whether normal behavior has been achieved through compensatory mechanisms. The current project aims to document a group of such OO individuals, explore possible persistent weaknesses in areas central to ASD, characterize the range of treatments they received, and look for biological characteristics through structural and functional MRI.
Basically, what the authors did was to characterize these children who would be referred to by antivaccinationists as “recovered.” To do this, they identified a group of 34 children who had had a diagnosis of autism/ASD but no longer meet the criteria for the diagnosis, referred to as “optimal outcome” (OO) above. These children were compared with a group of 44 age- and nonverbal IQ-matched children with high functioning autism (HFA) and 34 children undergoing typical development (TD). What makes this study stand out is that the investigators did something very critical. They were very careful to accept only children whose diagnosis had been made by a physician or psychologist specializing in autism before the age of five verified with a written diagnostic report provided by the parents. Then, as a second step to confirm the diagnosis, the investigators took each report, removed language about the diagnosis, summary, and recommendations but leaving descriptions of the child’s behavior. This redacted reporta were then reviewed in a blinded fashion by one of the co-investigators, along with a bunch of “foil” (a.k.a. control) reports from children with non-ASD diagnoses, such as global delay or language disorder. All foils were correctly rejected, and four OO children’s reports were rejected for inadequate documentation of diagnosis. The second screen was to have the child’s current status evaluated, with clinicians with at least 15 years of experience, who reviewed that the child’s Autism Diagnostic Observation Schedule (ADOS) scores were below ASD thresholds and that in their clinical judgment an ASD was not present.
The overall schema is summarized below:
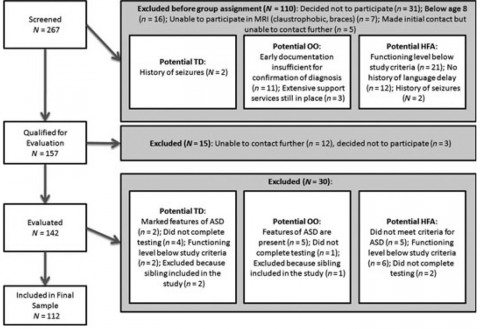
Other criteria included that the children in the OO group had to be fully included in regular education classes with no one-on-one assistance and no education services to address autism deficits (e.g., no social skills training) and that scores on another communication-related test had to be at or above a certain level.
So what next? Well, the authors interviewed the parents and tested the children using several measures, with, where knowledge of group could affect scoring, the tests scored by a researcher blinded to what experimental group the children. These measures included ADOS, Autism Diagnostic Interview-Revised (ADI-R); Social Communication Questionnaire (SCQ); Wechsler Abbreviated Scale of Intelligence (WASI); Vineland Adaptive Behavior Scales (VABS); Benton Facial Recognition Test; Clinical Evaluation of Language Fundamentals-IV (CELF-IV); and the Edinburgh Handedness Inventory. Sex, age, and handedness didn’t differ between the three groups, but verbal IQ was 7 points lower in the HFA group, compared to the OO and TD groups, where it was in the high-average range.
Losing the diagnosis
The investigators reported a number of observations of their groups. First, communication and socialization ADOS scores didn’t differ between the OO and TD groups, although the authors do note that “seven OO participants were judge to have social functioning mildly affected by nonautism conditions, such as anxiety, depression, or impulsivity” and that they will report a full exploration of the psychiatric functioning of all three groups in a separate study. They also noted that by early history the OO group demonstrated somewhat milder social symptoms than the HFA group but that they did not differ in communication or repetitive behavior symptoms. A small number of OO children demonstrated some weakness in the facial recognition test, but it was not statistically distinguishable from what would be expected in the population at large. Overall, by the measures used, the OO children were for the most part indistinguishable from TD children. It was also reported that the children who fell into the OO group also tended to have slightly milder autism upon diagnosis than the HFA group by the ADI-R and SCQ-Lifetime results. Basically, their social deficits seemed to be less marked. However, their language delay and repetitive behaviors were similar to those of the HFA group, at least within the limitations of recollections an documentation from a decade or more before (the mean ages of the groups ranged from 12.8 to 13.9 years).
Of coure, the biggest limitation of this study is that it says nothing about what percentage of autistic children can achieve the “optimal outcome” of losing their ASD diagnosis about what interventions are most likely to facilitate such improvements. The review article from Helt et al that I mentioned before estimated that between 3% and 25% of children diagnosed with an ASD “lose the diagnosis.” However, the percentage who would have achieved this without intervention is unknown. Clearly, a lot more study is needed.
This most recent study (Fein et al) is in line with a study from last year by Fountain et al, which showed up in some media reports last spring. This study reported that approximately 10% of children diagnosed with autism/ASD by age 3 “bloomed”; i.e., they improved rapidly, to the point that by age eight they were high functioning. Similar to Fein et al, Fountain et al observed that repetitive behaviors don’t seem to change as much and that it’s mainly the social and communication dimensions where huge variability in outcomes is seen. Fountain et al also found these correlates with “blooming”:
Bloomers differ from other children with respect to intellectual disability and socioeconomic characteristics. Among young children with severe autism, those most likely to “bloom” are those without intellectual disability and those with more educated, nonminority mothers. Although we are unable to identify the specific mechanisms through which socioeconomic status affects trajectory outcomes, the intervening variables likely include home and neighborhood environments, quality and intensity of treatment, quality of education, the efficacy with which parents are able to advocate for their children with institutions providing services, and many other factors in various permutations. If this heterogeneity in outcomes is associated with parental and community resources, then equal access to early intervention and treatment resources for less-advantaged children is vital. Although some trajectories may be associated with different etiologic drivers, if etiology alone were driving outcomes, we would be less likely to observe the strong socioeconomic effects unless socioeconomic status was associated with exposure to some biological risk factor for a particular autism subtype.
Not surprisingly (at least not to those of us who have followed the antivaccine movement), it is the autistic children born to the types of parents most likely to be antivaccine (more educated, non-minority, higher socioeconomic status) who are most likely to “bloom,” no “biomed” intervention necessary. That’s why, when evaluating whether an intervention of any kind, be it behavioral, medication, or even “biomed,” “works” in autism, it is essential to have a prospective randomized controlled trial. To see what I mean, I’ll refer you to a blog post that is six years old but still very relevant. It’s by Prometheus and entitled, appropriately enough, Listening to Autism. He begins by pointing out that parents, because they observe their children every day, believe that they understand their autism better than anyone else, even experts. Of course, it’s equally, if not more, likely that they are so close to their children that they can’t be objective and that their lack of objectivity can profoundly color their observations and thus lead them astray (confusing correlation with causation, for instance, or mistaking regression to the mean for real improvement), but few of them ever seem to acknowledge, much less accept, this possibility. Prometheus then goes on to discuss the prototypical example of an autism “biomed” treatment: Secretin.
Secretin: A magic bullet that shot blanks
Secretin first hit the scene in 1998, when it was first reported that a single injection of secretin, used as a routine part of endoscopy, appeared to dramatically improve the language and functions of an autistic child. This reporte led to a lot of excitement, a lot of use of secretin, and a bunch of studies of many varieties, short-term, long-term, case series, and, eventually randomized trials. Many of these studies did not support the initial results. Finally, there was a randomized clinical trial done by Repligen, the company that sells Secretin, that was negative. Today, the scientific consensus, as described in a Cochrane Review and multiple other reviews of the scientific literature, is that secretin does nothing for ASD symptoms and that its use in ASD warrants no further study.
None of this stops the autism biomed crowd from advocating and using secretin. If you go to, for instance, the antivaccine crank blog Age of Autism, you will from time to time find commenters extolling the virtues of secretin long after the science has been settled. Other websites still tout it, as well. Indeed, the Florida branch of the Scientology front group Citizens Commission on Human Rights (CCHR) recently argued that the reason the scientific trials of secretin were negative was because the investigators used a “synthetic” version of secretin, while the “dramatic improvements” came from a “natural version” of the hormone from pigs. In other words, some parents and quacks still swear by secretin, even though the evidence is even clearer that secretin does nothing for autism than it is that vaccines do not cause autism.
Luck, greed, and hope
To explain this, combined the results that I just discussed above with a tale that Prometheus tells, which he calls the Tale of the Lucky Stockbroker:
Long, long ago, a smart fellow decided that he would try to make a lot of money in the stock market. Having watched the market for some time, he realized that the best way to make money on stocks wasn’t to buy and sell them, but to sell expert advice.
Knowing that most people who invested in stocks were wary of advice, he set out to prove to people that he had a special power for knowing when stocks were about to go up or down. He got a list of a ten thousand people who were avid stock traders and sent each of them an e-mail describing his services (and fees) and giving them a “sample” stock pick.
Half of the prospective customers got an e-mail saying that the stock would go up in the next week, and half of them got an e-mail saying that the stock would go down. At the end of the week, the stock he picked had gone down, so he sent another e-mail to the five thousand people who had received the “correct” stock advice.
Half of the five thousand got an e-mail saying that another stock would go up in the next week; half got an e-mail saying it would go down. At the end of the week, he sent out another e-mail to the remaining 2500 would-be customers.
At the end of six weeks, he was down to a little over 150 potential customers, but those 150 has seen him make six correct stock predictions in a row! The last e-mail he sent them was to tell them that they could continue to get these predictions only if they bought a five-year subscription to his service.
There is no claim that autism “biomed” quacks are deliberately doing something like this, although perhaps a few are. However, in effect they are doing something like this. Parents who seem to see results, nearly always due to random chance alone and the human tendency to confuse correlation with causation, will convince themselves that whatever treatment they have chosen is “working.” Given that the very parents who tend to gravitate towards autism biomed treatments tend to be the same parents who blame their children’s autism on vaccines, this should not be surprising. They are already likely to easily confuse correlation with causation. Because children, autistic and non-autistic, develop in “spurts,” it’s very easy to think that a treatment that by chance alone happened to be started right before a period of rapid development, was the reason for the improvement in the autistic child’s symptoms, even if it were homeopathy (i.e., water) that was used. Meanwhile, the parents who don’t see any improvement will drift away from the “treatment,” frustrated that it “didn’t work.” Others lash out at any suggestion that autistic children can “recover” spontaneously or with something other than quackery, for instance, Kim Stagliano of the antivaccine crank blog Age of Autism:
Oh! And did you hear some kids “outgrow” their autism. Yuppers. In the Catholic Church we call that a miracle. When Jenny McCarthy told the media her son had lost his diagnosis she was called a liar. Turns out that the only way to lose the diagnosis is by doing nothing. Jeez, I’m always the last to know… I could be driving that Camaro I’m constantly talking about on Facebook with the money we’d have saved.
I’m not sure why there is such hostility here. My guess is that it’s the implicit conclusion that a significant but unknown percentage of children with autism/ASD can develop rapidly and ultimately fall into the neurotypical group. It doesn’t even much matter, for purposes of the observation that “outgrowing” autism is possible what the mechanism is. The authors propose other possible explanations besides development resulting in brain function that is more neurotypical, for example:
A pressing theoretical question is to what extent brain structure and function have normalized in the OO children. It is possible that effective early intervention plus maturation have resulted in the normalization of pathways and functions or even anatomical structure. Dawson et al. (2012) were able to show EEG evidence of normalization of cortical activation in response to faces versus objects in children receiving Early Start Denver Model intervention for 2 years in early childhood, supporting this possibility. Alternatively, successful intervention may have resulted in compensatory functions, such that overt behavior is normal, but atypical pathways or levels of activation are needed to achieve these behavioral results, as has been shown, for example, in dyslexia by Eden et al. (2004). Structural and functional MRI data were obtained from a subset of each group in the present study and are being analyzed.
More likely, it is a combination of factors. Whatever the case, if anything, Fein et al should provide hope to parents of autistic children by emphasizing that autism is not static and that it should be possible, depending upon the mechanism at work in these children who “grew out of” their autism, to identify science-based personalized strategies to maximize the potential of each autistic children, not to mention the chances that they can eventually function as fully independent members of society living productive lives.