{kind=link}
There are some weeks when I know what my topic will be—what it must be. These are weeks in which the universe gives the very appearance of handing to me my topic for the week on the proverbial silver platter with a giant hand descending from the clouds, pointing at it, and saying, “Blog about this, you idiot!” Usually, it’s because a study is released or something happens or a quack writes something that cries out for rebuttal. Whatever it is, it’s big and it’s unavoidable (for me, at least).
This is one of those weeks.
The reason it’s one of those weeks is because just last Friday, as I was driving to work, I heard a news story on NPR about a study that had just been released in the Journal of Pediatrics. The story, as it was reported, noted that the study being discussed looked specifically at a certain antivaccine trope and found for yet the umpteenth time that vaccines are not correlated with an increased risk of autism. Normally the news that a study had once again failed to find a link between vaccines and autism would be as surprising as a study finding that the sun rises in the east and sets in the west, or finding that water boils at 100° C at sea level. At this point, the evidence is so utterly overwhelming that there is not a whiff of a hint of a whisper of a correlation between vaccines and autism that it has become irritating that antivaccine activists keep pressuring scientists to do the same study over and over again, coming up with the same results over and over again, and then seeing antivaccinationists fail to believe those same results over and over again. Apparently, antivaccine activists think that if the same sorts of studies are done enough times, there will be a positive result implicating vaccines as a risk factor for or contributing cause to autism. By sheer random chance alone, this might happen someday, given the definition of statistical significance, but so far there has not been a single large, well-designed epidemiological study by reputable researchers that has found a link.
The final nail in the coffin of “too many too soon”?
Its utterly expected result notwithstanding, what makes the study reported on by NPR interesting is that it looked specifically at a common antivaccine trope that started popping up a lot five or six years ago. To my knowledge, although it had been percolating for a couple of years before that, this trope had its big debut when Jenny McCarthy led an antivaccine “protest” march on Washington, DC in June 2008, coupled with the delightfully Orwellian slogan, “Green our vaccines!” Quite honestly, I had to hand it to the antivaccinationists. “Too many too soon” and “Green our vaccines” were great slogans. They were pithy, simple, and communicated the message that vaccines were toxic and that they shouldn’t be given to young children. From a scientific standpoint they were horribly wrong, but from a propaganda standpoint they were brilliant, not the least of which because “too many too soon” was much more difficult to falsify than other antivaccine tropes, such as the roundly falsified claims that the mercury-containing preservative thimerosal causes or contributes to autism, that vaccines are loaded with “toxins,” and the idea popularized by the now disgraced Andrew Wakefield that the MMR triple vaccine could result in “autistic enterocolitis” and autism itself. This study looks right at the “too many too soon” hypothesis and finds zero evidence to suggest that there is anything to it. As I said, this could be completely predicted beforehand, but antivaccinationists keep forcing scientists to do the same study over and over and over again in different ways. They’re still not convinced, but we can always hope to convince the fence sitters.
The study itself was carried out by Frank DeStefano, Cristofer S. Price, and Eric S. Weintraub, from the CDC and Abt Associates, and the complete study, Increasing Exposure to Antibody-Stimulating Proteins and Polysaccharides in Vaccines Is Not Associated with Risk of Autism is available to all online, which is a lovely thing. It also used publicly available data from a previous study published in 2010 that looked for associations between mercury exposure in thimerosal-containing vaccines and autism. I discussed this study in detail when it originally came out and therefore won’t discuss it further (at least not much) here.
The previous study (Price et al) and this study (DeStefano et al) were both based on the same case control study. A case control study is a type of retrospective study in which subjects with a certain condition (cases) are matched as closely as possible with subjects without the condition under study (controls), and the two groups compared to look for factors that correlate with the condition in the cases. That’s how an earlier study from 2007 that failed to find a link between thimerosal-containing vaccines (Thompson et al) and adverse neurodevelopmental outcomes was performed, and that’s how Price et al and DeStefano et al were also performed. Being retrospective, such a study can never be quite as rigorous as a randomized controlled trial or a prospective cohort study. However, given that thimerosal has already been removed from all infant vaccines other than the flu vaccine (and there is a thimerosal-free alternative) and, more importantly, that it would be unethical to conduct a randomized double blind, placebo-controlled clinical trial, this sort of trial is the best evidence that we will be able to come up with.
I think it’s worth briefly recapping the design of this study, so that you don’t have to spend too much time clicking on previous links:

Basically, the two groups that ended up being studied consisted of 256 children with ASD and 752 matched controls. The authors justify the study thusly:
The initial concerns that vaccines may cause autism were related to the measles, mumps, and rubella vaccine and thimerosal-containing vaccines. In 2004, a comprehensive review by the Institute of Medicine concluded that the evidence favors rejection of possible causal associations between each of these vaccine types and autism. Nonetheless, concerns about a possible link between vaccines and autism persist, with the latest concern centering on the number of vaccines administered to infants and young children. A recent survey found that parents’ top vaccine-related concerns included administration of too many vaccines during the first 2 years of life, administration of too many vaccines in a single doctor visit, and a possible link between vaccines and learning disabilities, such as autism. All of the foregoing concerns were reported by 30%-36% of all survey respondents, and were reported by 55%-90% of parents who indicated that their children would receive some, but not all, of the vaccines on the recommended schedule. Another recent survey found that more than 10% of parents of young children refuse or delay vaccinations, with most believing that delaying vaccine doses is safer than providing them in accordance with the Centers for Disease Control and Prevention’s recommended vaccination schedule.
So basically this research was driven not so much by a scientific question as by a social imperative. Scientists have long known that there is no compelling rigorous evidence suggesting that vaccines cause autism or that “too many too soon” can result in or predispose to autism. Sadly, it can’t be repeated too many times (as I’m repeating here) that antivaccinationists force scientists to keep reinventing the wheel in order to try to reassure the parents whose doubts are stoked by the misinformation and pseudoscience promoted by antivaccinationists.
Before I get to the results in detail (you already know the results in general), I’ll also reiterate a point I made when discussing Price et al that this study had the strength that derives from the fact that the case and control populations were collected from three managed care organizations (MCOs) that participate in the Vaccine Safety Datalink, a collaborative effort between the CDC’s Immunization Safety Office and nine MCOs that was established in 1990 to monitor immunization safety and address gaps in scientific knowledge about rare and serious events that can occur after immunization. The VSD uses a large linked database using administrative data sources at each MCO from which data are gathered on vaccination(vaccine type, date of vaccination, concurrent vaccinations), medical outcomes (outpatient visits, inpatient visits, urgent care visits), birth data, and census data. Consequently, because of the detailed records maintained by these MCOs, investigators using VSD data are able to develop a detailed and accurate estimate of vaccine exposure from the computerized databases maintained by the MCOs as well as the medical records of the cases, controls, all supplemented by standardized interviews with the parents. In addition, outcomes have been measured in clinical settings using standardized assessment tools. In Price et al, the most up-to-date standardized assessment tools used to diagnose ASDs were used to identify cases, and the same is true in DeStefano et al. In addition, in order to make sure that the controls did not include children with undiagnosed ASD, which would tend to decrease any apparent differences between the groups, the lifetime form of the Social Communication Questionnaire was administered to controls as part of the interview with each mother for children who had indications of any neurodevelopmental difficulties. Several children were excluded from the control group in this manner. Finally, the detailed medical records and databases maintained by the MCOs allowed for the detailed determination of and control for many potential confounders.
Another major strength of DeStefano et al is how the investigators chose to compare vaccine exposures; basically, they estimated total antigen exposure rather than just counting the number of vaccines. They also looked at total antigen exposures from vaccines administered at single visits as well as the cumulative antigen exposure:
We evaluated antigen exposure for 3 age ranges according to 2 measures: cumulative exposure to antigens within the specified age range and the maximum number of antigens received in a single day within the specified age range. Data were collected on a large number of covariates, including child and family characteristics, maternal exposures during pregnancy, childbirth conditions, early childhood health conditions, and maternal healthcare-seeking behavior (ie, Kotelchuck prenatal care index, cholesterol, and Pap smear screenings).
For those who aren’t familiar with immunology, an antigen is a substance that evokes the production of one or more antibodies. In the case of vaccines, an antigen could be a protein or polysaccharide. In the case of killed vaccines (in which extracts isolated from killed viruses or bacteria are used to provoke the antibody response), there can be dozens, or hundreds, of antigens. An example is the whole cell pertussis vaccine, which is not used anymore. More modern vaccines tend not to be killed organism vaccines anymore, but rather vaccines made of recombinant proteins, protein fragments, or polysaccharides. Such vaccines contain many fewer antigens, but they are the specific antigens that produce an effective immune response against the organism. The vaccines examined in the study ranged from a single antigen per dose (hepatitis B) to 3,004 antigens per dose (DTP-Hib).
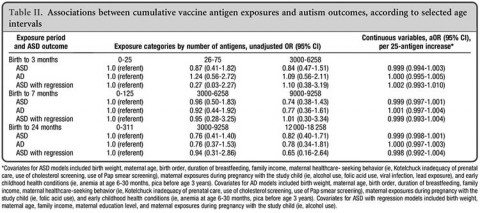
Using a strategy similar to the earlier Price et al study, DeStefano et al examined antigen exposure and compared the number of vaccine antigens to which the controls and the cases were exposed. What do you think they found? Yes, I know. I already told you what they found from the beginning: Nada, zip, nothing. No correlation between antigen exposure from vaccines and the risk of developing autism or autism spectrum disorder (ASD)—or even ASD with regression. The results are summarized in Table II from the paper, which shows that there is no correlation between cumulative vaccine antigen exposures and autism outcomes:
Nor was there a correlation between maximal antigen exposure at one session of being vaccinated and autism outcomes:
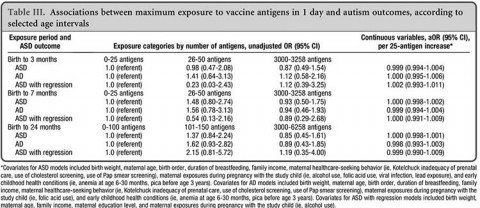
This is as negative a study as I have ever seen. There is not even a whiff of a hint of a whisper of an association between the number of antigens to which the cases and the controls were exposed and the subsequent risk of autism. Not only do the confidence intervals for the adjusted odds ratios all overlap 1.0, but they’re very tight. It doesn’t get more negative than this in an epidemiological study, leading the authors to conclude:
We found no evidence indicating an association between exposure to antibody-stimulating proteins and polysaccharides contained in vaccines during the first 2 years of life and the risk of acquiring ASD, AD, or ASD with regression. We also detected no associations when exposures were evaluated as cumulative exposure from birth to 3 months, from birth to 7 months, or from birth to 2 years, or as maximum exposure on a single day during those 3 time periods. These results indicate that parental concerns that their children are receiving too many vaccines in the first 2 years of life or too many vaccines at a single doctor visit are not supported in terms of an increased risk of autism.
They also note:
Considerations of biological mechanisms should be taken into account when evaluating a possible association between autism and immunologic stimulation from vaccines early in life. The infant’s immune system is capable of responding to a large number of immunologic stimuli. Beginning at birth, an infant is exposed to hundreds of viruses and other antigens, and it has been estimated that an infant theoretically could respond to thousands of vaccines at once.15 The possibility that immunologic stimulation from vaccines during the first 1-2 years of life could be related to the development of ASD is not well supported by the known neurobiology of ASD, which tends to be genetically determined with origins in prenatal development,19-22 although possible effects in early infancy cannot be ruled out completely. It can be argued that ASD with regression, in which children usually lose developmental skills during the second year of life, could be related to exposures in infancy, including vaccines; however, we found no association between exposure to antigens from vaccines during infancy and the development of ASD with regression.
In other words, from the standpoint of prior plausibility, there is no compelling reason to suspect that vaccines could cause autism because such a mechanism is not consistent with what we know about the neurobiology of autism. Consistent with this lack of plausibility, the authors failed to find any correlations between exposure to antigens from vaccines and the risk of autism. They sliced and diced the data in a variety of ways looking for correlations and didn’t find any, and their data are in agreement with a study by Smith et al (discussed by my “good bud” Orac here) that failed to find a difference in non-autism neurodevelopmental outcomes between children who received all their recommended vaccines on time and those who were late, or, as I like to view it, “too many too soon” versus “too few too late.”
Yes, there were limitations to DeStefano et al in that it was retrospective. In addition, as the authors discussed, not all antigens are equal in evoking an immune response. Some have more epitopes (areas on the antigen molecule that can trigger an immune response) than others, and the study didn’t weight the antigens for the intensity of the immune response that they evoke. Even so, the antigenic load has fallen dramatically, and this study is based on the vaccine schedule of the 1990s. Indeed, the authors note that the antigen load due to the vaccine schedule has fallen from several thousand in the late 1990s to an estimated 315 in 2012. This is a drop in the bucket compared to the number of antigens infants and children encounter every day, as Emily Willingham notes. Matt Carey and Christine Vara also agree.
The antivaccinationists attack
Not surprisingly, even though this study was released on Good Friday, with a holiday weekend fast approaching, antivaccinationists were sufficiently displeased that they managed to launch a series of broadsides against the study. It’s instructive to look at the bad science and logical fallacies that populate such “criticisms.” For instance, Dr. “Bob” Sears, who is, despite his efforts to appear otherwise, as antivaccine as they come, went to Facebook to rant against the study. His complaints reveal such ignorance about statistical methods and basic epidemiology that it’s worth a quick look:
I pretty much only have one major criticism of this study. You would probably find the exact same results no matter what group of kids you studied. Pretty much all children in any given span of years receive the exact same number of shot antigens. (By the way, an antigen is simply a protein or sugar germ-related ingredient in a vaccine – some vaccines only have a few, some have many.) Virtually all kids WITH autism have had the same shots as kids WITHOUT autism. So, why would it even be useful to study this? You’ll get the same results every time, whether you study 1000 kids or 100,000 kids. They all get the same shots on the same schedule. They would have gotten the same results if they’d studies asthma, cancer, or any other chronic problem. All this study proved is that all the kids in that HMO got about the same vaccines over that 5 year time period. This doesn’t give us any useful data on how vaccines would have or would not have influenced the rate of autism.
Clearly, Dr. Bob doesn’t understand the very concept of a case-control study. Rather amusingly, he says that “virtually all the kids with autism have had the same shots as kids without autism” without realizing that that very conclusion in a case control study would be pretty powerful evidence that vaccine exposure is not a risk factor for autism! In actuality, though, he’s misstating the conclusion of DeStefano et al, anyway. The real conclusion was that the number of antigens from vaccines a child sees (which is a surrogate for vaccine load) has no correlation with that child’s risk of autism, ASD, or ASD with regression.
But if you really want hilarity, take a look at what he proposes as an alternative:
Now, if I were to do a study (and have several million bucks to fund it), here’s how I would look at the question of whether or not an increased number of vaccines relates to an increased risk of autism: I would take a bunch of kids who had all the vaccines on the regular schedule and look at the rate of autism in that group. We know that it’s about 1 in 50 kids. Then I’d take a whole bunch of kids who were only partially vaccinated and look at the rate of autism. I would subdivide the partially vaccinated group into subgroups based on the total number of vaccines given during infancy. I would perhaps have a group that delayed vaccines. And hey, while we’re at it, let’s really go crazy and find a few totally unvaccinated kids just for fun. On the other hand, no. Let’s not. It would be totally unethical to subject a group of totally unvaccinated children to any type of medical research. Ok, back to my study. These data would then give us a true look at autism rates compared to number of vaccines given and the age at which they were given.
Now THAT would be an interesting study. Unfortunately, it’s just too logical. It’s much better to study things in a confusing and illogical manner so you can get some results that the press can really sink their teeth into.
As I said, Dr. Bob’s ignorance is quite striking, because that’s rather what was done in Price et al for autism and Thompson et al for other neurodevelopmental outcomes. One notes that Dr. Bob also doesn’t tell us how he would compare these populations. What sort of study would he do? A case control? Oh, wait, he doesn’t like case control studies, finding them “confusing and illogical.” (No kidding. It’s very clear that he’s confused.) Maybe he would like a cohort study? Actually, that’s what he seems to be suggesting. After all, case control studies starts with the outcome (presence or absence of disease or condition) and then work back to exposure, while cohort studies start with exposure and work towards outcomes. Each study type has its advantages and disadvantages, but I get no sense that Dr. Bob has any clue about when it is best to use one versus the other. One notes, for instance, that Sir Richard Doll used the case control study method to be among the earliest investigators to confirm a link between cigarette smoking and lung cancer, while A. B. Hill used a cohort design. Both produced the same results, just from a different approach. Basically, it’s sour grapes. Dr. Bob just didn’t like the outcome of of DeStefano et al. His criticism of the study demonstrates that he has no understanding of the issues behind case control studies, and his suggestion of an apparent cohort study doesn’t address his rejection of DeStefano et al, specifically the question of why he thinks the results of DeStefano et al are so flawed that a huge new multimillion dollar cohort study is necessary to address the question of whether vaccines increase the risk of autism.
Instead, he retreats to conspiracy mongering and antivaccine fear mongering:
So, is anyone really surprised to see the Journal of Pediatrics study? What were you expecting? CDC researchers to publish as study that actually showed an increased risk of autism related to vaccines? The CDC would NEVER simply publish such a study. I doubt anyone would. Anyone at the CDC who published such a study would be fired faster than they could sell their Pharma stock.
Yawn. The pharma shill gambit. How original.
Of course, the antivaccine crank blog Age of Autism is very unhappy as well, but seems unable to muster any complaints much more coherent than those of Dan Olmsted, who basically mindlessly parrots Dr. Bob Sears’ objections, and Anne Dachel, who could muster nothing more than a call for the usual “vaxed versus unvaxed” study and reinforcing my conclusion that antivaccinationists don’t understand even the basics of clinical trial design, epidemiology, or ethics.
Perhaps the most amusing misunderstanding of basic epidemiology and the nature of a case control study comes from homeopath Heidi Stevenson of Gaia Health, who tries to argue…well, I’ll let you see for yourself:
As initially pointed out, this study was done on the assumption that there is no connection between autism and vaccinations. Therefore, there was no reason to do such a study. Why would you do a study on whether there’s an association between autism and vaccinations before you believe that there’s been a study demonstrating such a connection? If this were legitimate science, then there’d be no reason to do it.
Uh, no. This study was done to see if there was a connection between vaccine and autism detectable as a difference in vaccine antigen exposure between cases and controls. Stevenson digs herself in even deeper in terms of showing how little she understands what a case control study is when she writes:
This study, even if well done, would be meaningless simply because it jumps the gun. It makes no sense to do a study on the relative degree of a potential toxin’s effect on autism when no study has yet been done to determine that there is one. Since no such study has been done that officially implicates vaccines as the cause of autism, as explained earlier, what’s the point in doing a study focused on the relative degree of harm? This is pure duplicity on the part of the CDC.
One notes that Sir Richard Doll’s case control study was done before his and A.B. Hill’s cohort study. Does Stevenson doubt that smoking is an enormous risk factor for lung cancer? No, case control and cohort studies are different methodologies that each have advantages and disadvantages compared to the other. However, if a case control study as well done as DeStefano et al is so completely negative, there is no scientific justification for proceeding to do a cohort study. Yet that’s exactly what Dr. Sears and a homeopath are demanding because they think that a different study methodology will show them what this methodology didn’t. No doubt if someone did a cohort study of the type they want and it was negative, they’d proceed to demand a case control study.
Stevenson also tries to nitpick aspects of the study. For instance, she complains that more controls were eliminated than cases. The reasons for this were explained in both Price et al (in more detail) and in DeStefano et al, namely that they were deemed ineligible because they didn’t meet the protocol requirements. Indeed, in my previous post on Price et al, I reproduced the flowsheet that showed exactly how cases were ascertained and how subjects who fell under various exclusion criteria were eliminated. This study uses the same subjects, so the same flowsheet applies. One wonders whether Stevenson bothered to look up Price et al. Whether she did or not, Stevenson appears not to understand the concept of a case control study and how the cases and controls have to be matched as closely as possible for everything other than the condition that differentiates them.
Then, Stevenson lays down this doozy:
They looked at the number of antigens given to each child, both overall for their first two years and the number given on single days. This presumes that the number of antigens, rather than the number of vaccinations is the issue. It completely ignores adjuvants and other vaccine ingredients, including known toxins such as formaldehyde, mercury, and sorbitol 80, among others.
So which is it? “Too many too soon” or “the toxins“? I can’t tell. I guess it’s whatever argument happens to be convenient that day for the antivaccinationist making it.
The “evolution” of the antivaccinationist
Over the last decade or so, the reasons antivaccinationists advance for their fear and loathing of vaccines as an alleged cause of autism have “evolved” in response to what can be considered the “selective pressure” of scientific studies. It’s not surprising that that evolution has involved a tendency to migrate to hypotheses (I’m being really generous using that word here, I admit) whose main trait is to become more difficult to falsify. For instance, back in the late 1990s and early 2000s, the two predominant ideas were that MMR causes autism (this idea was most common in the U.K., thanks to Andrew Wakefield) or that the mercury in the thimerosal preservative in childhood vaccines caused autism (the favored notion in the U.S.). These were straightforward “hypotheses” that could be falsified using epidemiological studies of relatively simple design. And they were falsified roundly.
Then came the “toxins” gambit, which postulated that vaccines were full of vile substances ranging from antifreeze to formaldehyde to aborted fetal tissue. This one was more difficult conceptually in that there are a number of chemicals in vaccines, but they are all present at doses that are harmless. However, saying that was a harder sell, and the idea behind the “toxins” gambit was to force scientists to have to test each chemical, each adjuvant, each ingredient individually, a difficult enough task given the number of chemicals, and then in various combinations, an impossible task. That the task was impossible was the very point, of course. No matter how many trials scientists did, antivaccinationists could always say, “What about this adjuvant or this combination of adjuvants?”
Which brings us to “too many too soon.” It appeared to be a “hypothesis” that was impossible to falsify, but DeStefano et al came about as close as it’s ethically possible to falsifying the hypothesis. No wonder that all that antivaccinationists are left with are calls for “vaxed versus unvaxed” studies and pharma shill ranting.