{kind=link}
Dug the Dog strikes again, as he did three weeks ago. I had a couple of ideas for a post this week, but none of them were time-sensitive or timely. Then, over the weekend, I saw a post on the antivaccine crank blog Age of Autism by Dan “Where are the Autistic Amish” Olmsted entitled Weekly Wrap: Another Medical Practice with a Sane Vaccine Schedule – and No Autism. Given the tendency towards a—shall we say?—lack of accuracy of Olmsted’s previous reporting, it’s no surprise that he’d latch on to this study. I’m also seeing it appear around other antivaccine websites. I had gotten wind of it late last week, a few of my readers having sent it to me but hadn’t decided yet whether to blog about it. Then it appeared on AoA. Thanks, Dan.
So let’s see how this study is being spun by the antivaccine movement:
When we at Age of Autism talk about ending the epidemic, the “to do” list seems almost overwhelming – funding a vax-unvaxed study, getting mercury out of flu shots, proving the HepB shot is nuts, wresting control of the agenda from pharma, fixing Vaccine Court (this time in the good sense of “fix”), establishing that biomedical treatments help kids recover, and on and on.
But there’s a shortcut to all this, and it goes straight through pediatricians’ offices. The evidence is growing that where a sane alternative to the CDC’s bloated vaccine schedule is offered, and other reasonable changes adopted, autism is either non-existent or so infrequent that it doesn’t constitute an epidemic at all.
The latest example comes from Lynchburg, Va., and the pediatric practice of Dr. Elizabeth Mumper. She noticed a frightening rise in autism in the 1990s. Concerned that vaccines and other medical interventions might be playing a role – concerned in other words that SHE was playing a role — Mumper changed course.
Fewer vaccines. Fewer antibiotics. No Tylenol. Breast-feeding. Probiotics. Good, pesticide free diets.
Since then, hundreds more children have been seen in her practice, Advocates For Children. But no more autism.
In essence, this study is being spun to imply that doing all of these things will eliminate autism, or at least dramatically decrease its prevalence.
You can see one thing just from this description that makes me doubt this study, and that’s something very simple: Changes in too many variables being tested at once. Even if Dr. Mumper’s study shows what she claims it shows (and what Dan Olmsted advertises it as showing), there’s no way of knowing which, if any, of these things was responsible for the changes observed. I could say this quite easily before I even read the study. Fortunately, all of you can read along, because Mumper’s study is available online for all. Or maybe unfortunately, because, as you might expect, it’s not a very good study. Its hypothesis is diffuse and unclear, and it’s based on dubious science. Its methodology isn’t so hot either. Let’s take each in turn.
First, though, I have to make a general observation about this paper. That general observation is that it’s very sloppily put together. One notices that there are only 52 references listed, even though citations number up to over 100 in the text. It really does look as though the reference list is incomplete or wrong, as just a brief perusal showed me citations that do not appear to relate to the text in which they are being cited. For instance, after a sentence mentioning fecal transplants, Mumper cites references 35 to 37, none of which has anything to do with fecal transplants. One paper is about the consolidation of memory in the amygdala, while the others are about neurocognition in schizophrenia and impaired inhibitory control in children with ASDs. That’s just one example. To me it looks as though the wrong reference list might have been printed, or that Mumper didn’t bother to make sure that the citation numbers match the references.
Mumper starts with standard “autism epidemic” exaggerations and misinformation, in which she states in the very first paragraph that during the time she has been a practicing pediatrician the prevalence of autism has increased from 1 in 5,000 in 1975 to as high as 1 in 50 in 2013. As we’ve pointed out here many times before, the increase in the reported prevalence of autism and autism spectrum disorders (ASDs) is almost certainly accounted for by three things: (1) the broadening of the diagnostic criteria for ASDs in the early 1990s; (2) diagnostic substitution, in which conditions that were formerly classified as something else are reclassified as an ASD; and (3) intensive screening programs. We’ve noted that recent studies examining adult cohorts for ASDs using current-day criteria have produced estimates of autism prevalence similar to what is being reported in children now (for example, this one). Not surprisingly, antivaccinationists don’t like these studies. They also don’t like it when I point out that screening for a medical condition—any medical condition—will result in an apparent increased prevalence of that condition, as previously subclinical and undiagnosed cases are discovered. My favorite example of this is ductal carcinoma in situ, a precancerous condition in the breast whose incidence and prevalence have skyrocketed, largely thanks to mammographic screening programs, which I explicitly compared to autism and ASD prevalence. The bottom line is that, although we can’t rule out a modest increase in the true prevalence of ASDs, there almost certainly is no “autism epidemic.” Worse, from the view of antivaccinationists, if there is no “autism epidemic,” then vaccines almost certainly can’t be a significant cause of or contributor to autism.
Mumper then goes on to cite several papers that are either dubious, don’t support the vaccine/”toxin” hypothesis, or are unrelated, starting with various papers that claim a correlation between ASD prevalence and airborne pollutants. I’ve discussed at least a couple of these papers before, such as this one looking at mercury emissions from coal-burning power plants and this one claiming a correlation between proximities to freeways and ASD prevalence. Virtually every one of these studies that I’ve ever read suffer from one of the same flaws: The ecological fallacy or inadequate controlling for major confounders, in particular urbanicity and access to services. Mumper also tries to link breastfeeding to decreased ASD prevalence, but even she has to admit that there’s no evidence. In any case, I don’t know any scientist or pediatrician who would argue that breastfeeding is in general not good for babies (quite the contrary); so I’m not sure why she has focused on breastfeeding. Actually, upon further thought, I rather suspect that I do know. She tries to relate breastfeeding to the almost certainly nonexistent entity known as autistic enterocolitis, presenting in Table I gut biopsy results from 21 children in her practice with autism and noted that 13 had evidence of lymphoid nodular hyperplasia. Of course, there would be significant selection bias here, as presumably only children with GI symptoms would undergo colonoscopy and ileal biopsies. (At least, I hope that’s the case; it’s not as though certain practitioners who practice “autism biomed” haven’t been known to be a little quick to biopsy autistic children for questionable indications.) Then it was a community pathologist who examined the specimens; we have no idea if he was skilled in pediatric GI pathology. As Wakefield has taught us (thanks to Brian Deer), it’s very easy to mistake normal lymphoid nodule development for inflammation.
Next up, Mumper cites studies suggesting that probiotics during pregnancy and infancy result in less irritable bowel disease, allergic rhinitis, asthma, and various other disorders. All of this might or might not hold up to further scrutiny, but it’s really not related to autism and ASDs. None of this stops Mumper from trying to relate these studies to ASDs through the “immunological actions” of probiotics. To say that this is speculation is to be kind. That’s what it is at best: Speculation. At worst, it’s completely unfounded speculation. And so it goes. Mumper goes on and on about nutritional factors that might or might not be related to ASDs, the use or overuse of antibiotics, the claim that acetaminophen might be related to ASDs when given after vaccination. It’s all terribly thin gruel upon which to build a study.
Then, of course, there’s the vaccine issue. In justifying looking at vaccines, Mumper cites the tired, old familiar litany of bad science and pseudoscience:
The CDC and AAP have issued statements that vaccines are not associated with the risk of autism and that there are epidemiologic studies suggesting no causal role.58-60 Under immunization as a result of parental perceptions of vaccine safety remains a primary concern of the American Academy of Pediatrics.61 As a result, primary care physicians are taught ways to address parents’ vaccine concerns, take opportunities to vaccinate, and use recall methods to catch patients up on vaccines.62 Despite having one of the most aggressive vaccination policies in the developed world, specifying 22 vaccine doses for a total of 12 diseases by 1 year of age,63 the United States had higher infant mortality rates in 2009 than 33 other nations.64
Notice that the numbering of all the references cited starts at 58. The reference list only goes up to 52. I know, I know. I’m repeating myself. But I had to keep looking at it again and again, because I couldn’t believe that such a blatant error was made and had to keep going back to look at the paper and its reference list. In any case, I couldn’t look up the references cited in the passage above. I could, however, guess at what reference 64 might have been. I bet it was this execrably bad study, or another by the same authors. Reading the next paragraph, I realize that it almost certainly was one of those horrible studies by Neil Z. Miller, because Mumper mentions his name:
In 2009, five of the 33 nations with the lowest infant mortality rates required 12 vaccine doses, the least amount, while the United States required the most vaccine doses. Using linear regression analysis of unweighted mean infant mortality rates, Miller calculated a statistically significant high correlation between increasing number of vaccine doses and increasing infant mortality rates (r = 0.992 p value 0.0009).64 Correlation does not equal causation. But since the United States spends more money per capita on medical care than the rest of the industrialized world,65 it seems prudent to examine all possible contributions to the relatively poor health of our most vulnerable citizens – children.
Yup, Miller’s cherry-picked data dredging is definitely one of Mumper’s citations.
But enough of the unconvincing rationale for this study, what, exactly, did Mumper do? Well, she basically describes her strategies for “preventing” autism in her practice, which include:
- Minimizing environmental toxicant exposures. What this means, apparently, is “avoidance of pesticides and herbicides during pregnancy, feeding children and pregnant women a whole food diet that is as organic as possible, and using less toxic ‘green’ cleaning products in the home in hopes of preventing some cases of neurodevelopmental disorders and in the knowledge that it seems to be safe and reasonable anticipatory guidance for all children.” That’s all very nice, but based on little or no evidence.
- Maximizing breastfeeding prevalence. Again, I’m not sure that any pediatrician would argue with trying to encourage breastfeeding.
- Recommending probiotics. This is done, of course, based on the flimsiest of evidence.
- Nutritional counseling. To Mumper this means “1) pre-natal vitamins containing folinic acid, ideally in the active form such as 5 methyl- tetrahydrofolate, 2) eating locally grown organic fruits, vegetables and protein as much as possible 3) avoiding processed foods, preservatives, monosodium glutamate, aspartame, nitrites and 4) avoiding mercury containing fish.” None of this is bad, although there’s no evidence that organic fruits and vegetables are of any higher nutritional value than regularly farmed produce. There’s also no good scientific evidence that any of this correlates with autism.
- Antibiotic stewardship. No one is likely to argue that minimizing antibiotic exposure is a bad thing, but I’d also be concerned that Mumper doesn’t use antibiotics when they are actually indicated. Nor is there any good scientific evidence that antibiotic exposure has a causative or predisposing relationship with autism.
- Minimizing use of acetaminophen. Again, few would argue that we should use lots of acetaminophen, but, again, there is no good evidence that use of acetaminophen correlates with autism/ASDs or its complications or comorbid conditions.
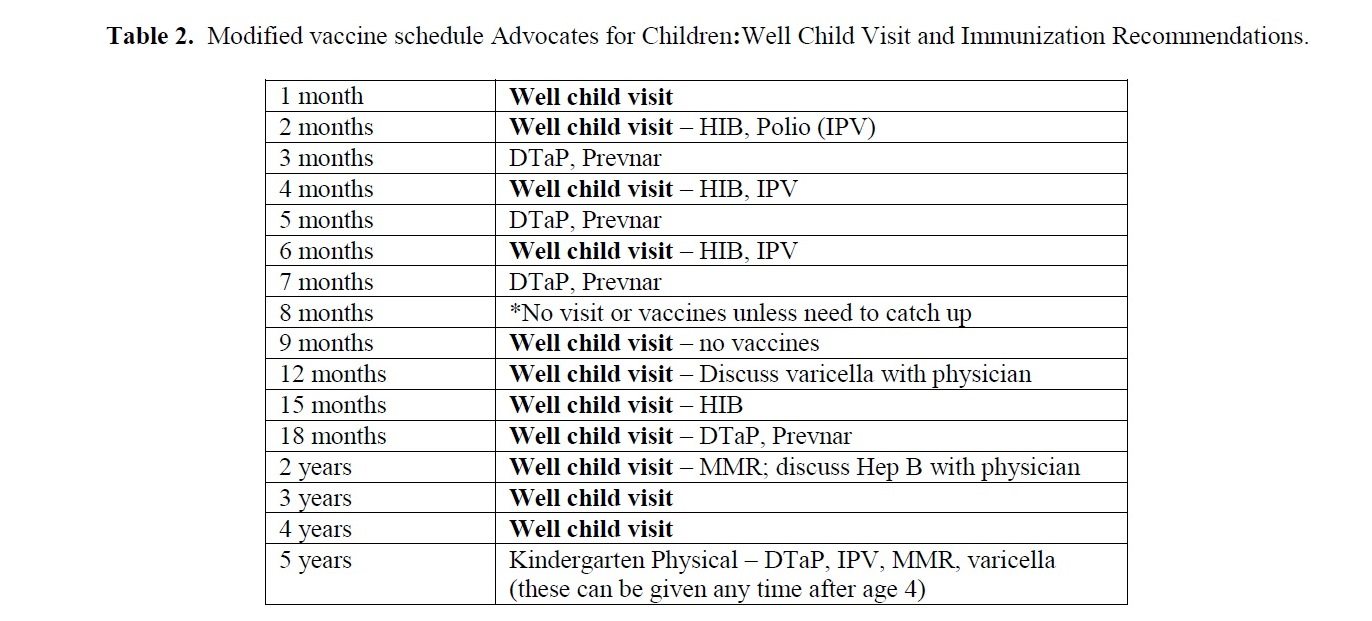
- Allowing/implementing a modified vaccine schedule. Here’s the tropes come in. Dr. Mumper’s schedule is basically a variant of the delayed vaccination schedule based on the “too many too soon” trope. (See below.)
So, here’s the vaccine schedule advocated by Dr. Mumpers (click to embiggen):
Now, let’s compare Dr. Mumper’s schedule to the CDC-recommended vaccination schedule (click to embiggen):
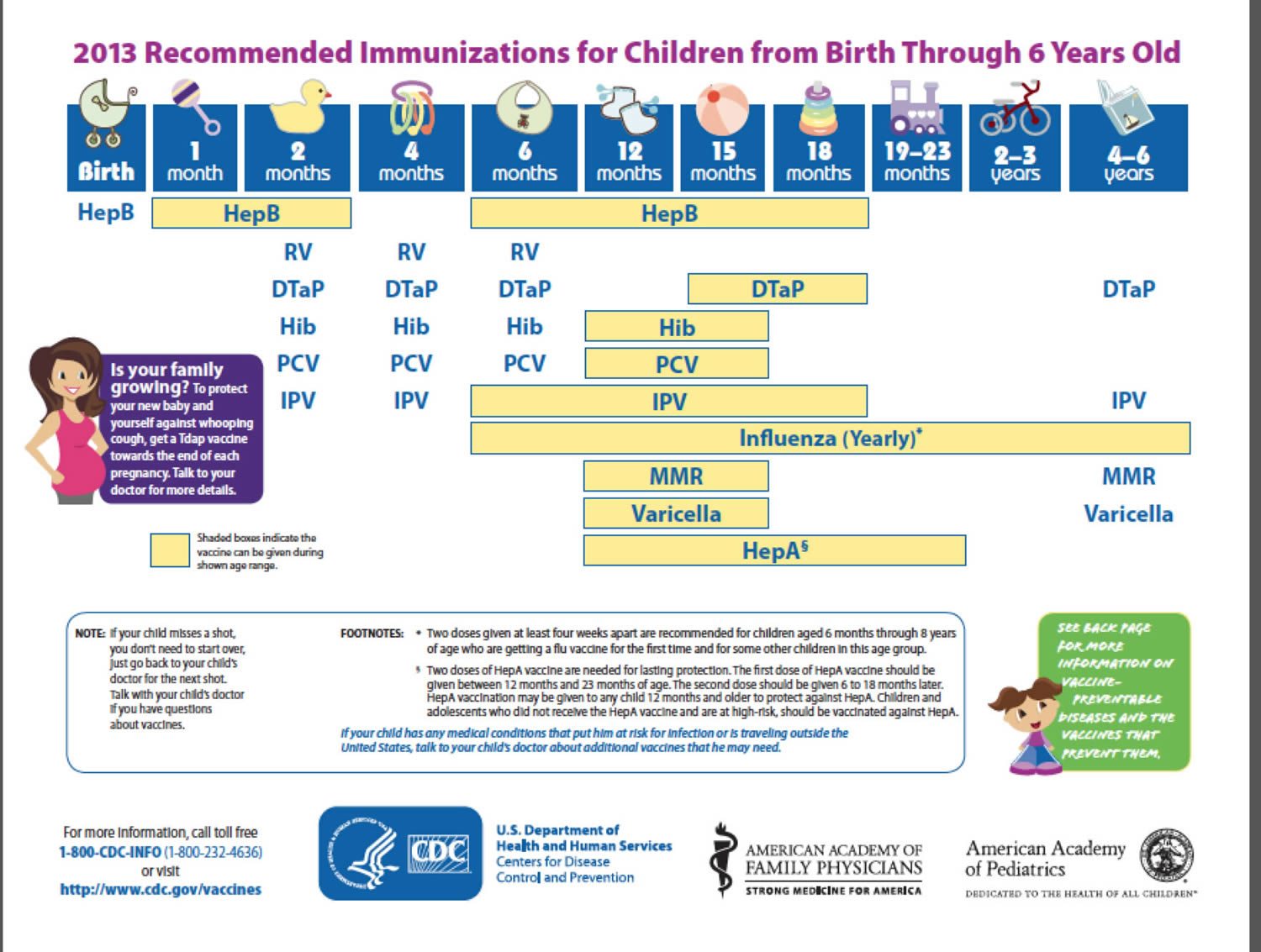
Prominent differences between Dr. Mumper’s proposed schedule and the CDC-recommended schedule are that Dr. Mumper doesn’t give flu vaccines, the hepatitis A or B vaccines, or the rotavirus vaccine. The MMR vaccine is pushed back to age 2, and the varicella vaccine (chickenpox) is pushed back to age 5. My initial guess was that the only reason Dr. Mumper requires the varicella vaccine is because it’s required in Virginia to enter school. In fact, this whole vaccine schedule strikes me as being the bare minimum to meet the Virginia state requirements for vaccines required to enter school or day care.
So what’s the bottom line? Mumper basically selected these patients:
Patient Selection
Inclusion criteria were: 1) all general pediatric patients born in 2005 or later; 2) presented for well child care prior to 2 months of birth and 3) followed until at least the age of 2 years and 2 months. Totally 294 patients qualified for the inclusion criteria and have been selected in the current research.
They were treated according to Dr. Mumper’s procedures listed above, and this is what Dr. Mumper found:
In the current research, there are no new cases of autism out of the 294 cases recognized and recorded, resulting in 0% prevalence of ASD. Based on the CDC background risk of autism of 1 in 50 for the cohort born around 2005 we would expect to have about 6 new cases of autism in our practice. We calculated our statistics using a Chi-squared test with 1 degree of freedom. Using the CDC autism rate of 1 in 50 reported in 2013 (but based on surveys of eight year old children), the expected rate for our 294 patients starting in 2005 would be 5.88 children with autism. Zero new cases of autism would occur by chance 1.4% of the time (p-value 0.014, significant at 0.05).
That’s it. That’s Mumper’s finding. That’s all there is to this paper. It’s a retrospective study with no control group that claims that she found no cases of ASDs in her practice since 2000 (but doesn’t have a patient number for the period between 2000 and 2005) and has found no new cases in the 294 patients followed in her practice from 2005 to 2013 from under two months of age at least to two years.
Just to check further into this, I took my handy dandy statistics program and played around with some numbers. Encouragingly (I suppose), when I ran a chi-squared test on Mumper’s numbers comparing them against a 1 in 50 prevalence reported earlier this year, I got a p-value of 0.0143. Of course, given that Dr. Mumper’s sample size is so small, it doesn’t take much for her “statistically significant” result to drop from statistical significance. For example, if I insert the autism prevalence of 1 in 88 from last year’s CDC study, the p-value jumps up to 0.071, no longer statistically significant. Given that last year’s study and this year’s study used different methodologies, it isn’t clear which figure is closer to the true prevalence of ASDs. Nor is the latest study evidence of an “autism epidemic,” but rather evidence that we are getting better at not missing any cases. In any case, playing around with different numbers, I found that the autism prevalence at large has to be at least 1 in 77 to make Dr. Mumper’s results statistically significant compared to the general prevalence of ASDs. I also found out that if she found just one case of ASD, the p-value would jump to 0.043, which would barely be statistically significant and is close to what Dr. Mumper reported in this case (0.042), which reassured me that I chose numbers for the control group similar or identical to what she chose. Two cases in Dr. Mumper’s practice would cause that p-value to skyrocket to 0.108.
Not surprisingly, Mumper reports that, after her paper was reviewed, one child was referred on suspicion of autism based on expressive language delay, but no diagnosis has been made. This brings up another issue (besides the fragility of her “results”). In a retrospective study like this, the control group has to be chosen to be as close as possible to the observation group, and Dr. Mumper just didn’t do this. The apparent prevalence of ASDs can depend on the availability of services (which is one reason why urban/suburban populations often appear to have more ASDs), screening, and socioeconomic factors. Dr. Mumper didn’t even attempt to compare the prevalence of ASDs in her practice to that of the surrounding area. For instance, in 2011, the prevalence of autism/ASD in Virginia was reported to be 0.8%. I realize that the more recent numbers are much higher and that the prevalence is increasing in Virginia, as it is for the rest of the country, but the latest figures that I could find for Virginia show a lower prevalence rate. The point is that we have no idea whether the number Dr. Mumper chose is a valid one to compare her practice to. That’s the problem with retrospective studies using existing prevalence as a control. They rarely tell us anything, particularly with such small numbers.
That is, of course, the very problem with small numbers. An N of 294 is way too small to make any hard and fast conclusions. Indeed, reading this paper I was amazed at how small the number was. An active pediatrician should have more than 37 new infant patients a year over nearly eight years. That’s less than one a week. Even if we take into account that all of these patients were seen before two months and followed at least until age 2 years, that’s still a small number for a pediatrics practice. One wonders how her practice can survive on those numbers. Be that as it may, what we have here is a dubious set of observations based on no clinical prior plausibility looking at a vaccine schedule that is based in no science and seems tailored to meet the minimum requirements of the Virginia school system’s vaccine requirements. On the other hand, given that Dr. Mumper appears to spend most of her effort treating children with developmental disorders with “autism biomed”, perhaps well baby visits are a small part of her practice. Then there’s the issue of the age range studied. The age range at which autism and ASDs are most commonly diagnosed is over the age of two; so how did Dr. Mumper assure that she captured all the diagnoses after age 2?
And did I mention that the center where these observations were made, the Rimland Center, appears to be, to my observations, a wretched hive of “autism biomed” quackery? Just take a look at its offerings: hyperbaric oxygen, reflexology, DAN! protocol treatments (that’s “Defeat Autism Now!” for those who aren’t familiar with “autism biomed”), gluten-free, casein-free, special carbohydrate diets, and more. All of this is consistent with the DAN! protocol, which includes pretty much every form of autism quackery known to quacks under its rubric, including chelation therapy, hyperbaric oxygen, and a wide variety of other quackery, such as Bioset supplementation, and Diflucan to “get the yeast out.” It’s no wonder that I’ve described “biomed” treatments like the DAN! protocol as uncontrolled and unethical experimentation on autistic children. It’s not for nothing that autism biomed has been referred to as an “autism cult.”
Finally, there’s Dr. Mumper herself. It’s not surprising that such a bad study would come from Dr. Mumper, as she is a vaccine-autism true believer to the point that she is cited in Whale.to and has presented at the yearly antivaccine quackfest Autism One and, most recently, at the 2013 Biomedical Conference. Also of note, Dr. Mumper has had her testimony dismantled in front of the Vaccine Court as one of the expert witnesses for the plaintiffs in the Autism Omnibus hearings.
In the end, Dr. Mumper’s study tells us a whole lot of nothing. Certainly, it is no evidence that doing what Dr. Mumper advocates doing has any effect whatsoever on the risk of developing autism in infants. The study will, however, be trotted out (as it has already been) as “evidence” that if we’d only decrease the number of vaccines, encourage breastfeeding more, decrease antibiotic usage and indulge in various unscientific interventions, we could virtually eliminate autism. It is evidence of nothing of the sort. Amusingly, however, this study is unlikely to be embraced by the hard core antivaccinationists. Why? Because even the decreased number of vaccines in Dr. Mumper’s proposed vaccine schedule are too many vaccines. (Just look at some of the amusing and depressing antivaccine comments after Dan Olmsted’s post.) To such antivaccinationists, one vaccine is one vaccine too many.