{kind=link}
[Editor’s note: Because of a family health emergency over the weekend, Dr. Gorski did not have a post ready for his usual Monday morning slot. This is also the reason that the virtual Q&A for the movie Virulent: The Vaccine War, originally scheduled for yesterday evening, was postponed and is in the process of being rescheduled. Fortunately, Dr. Jonathan Howard filled in. Dr. Gorski anticipates being back next week. In addition, since our recent loss of Dr. Harriet Hall, we now have a gap in our schedule on Tuesday. Until we are able to find someone to take that spot regularly—no one can ever truly replace Dr. Hall—Tuesdays will be empty.]
A question
Should the gravity of a medical condition be judged based on its underlying cause or the frequency/severity of the injury that results? Though I believe the gravity of a medical condition should judged based on the frequency/severity of the injury that results, my opinion is surprisingly controversial amongst doctors. I also do not believe that vaccine side effects can be equated to COVID deaths in young people simply because both are rare. One is much worse than the other. This too is surprisingly controversial amongst doctors.
COVID myocarditis
In an article titled “Setting the Record Straight: There is no ‘Covid Heart’” three medical “conservatives“, Drs. John Mandrola, Andrew Foy and Vinay Prasad, argued that “The issue of Covid-19 induced cardiac problems was massively overblown.”
They thought the frequency of COVID-related heart disease was not too concerning, referencing a study of athletes where “just 21 of the 3,000 had definite, probable, or possible cardiac involvement based on lab testing and cardiac imaging.” They said this rate, 1 out of 143 people, was “reassuring”. It was “less than 1%”, they correctly noted. They similarly discussed another study where “researchers studied 145 student athletes who had Covid-19 and found myocarditis in only 1.4% of them.”
“Just 21 of the 3,000″ and “only 1.4%” is how they described the rate of COVID-myocarditis.
Drs. Mandrola, Foy and Prasad were similarly reassured about the severity of COVID-related heart disease. “People who have recovered from Covid-19 have no special reason to worry about their hearts”, they wrote. “Even in the sickest of the sick, Covid-19’s effect on the heart appears to be modest,” they said about one study. “Cardiac magnetic resonance scans done during convalescence showed that nearly half of the individuals had no major heart abnormalities,” they wrote, though this means that just over half of the individuals had major heart abnormalities. Though Drs. Mandrola, Foy and Prasad did not report it, this study also found:
Myocardial infarction was found in 19% (28/148) and inducible ischaemia in 26% (20/76) of those undergoing stress perfusion (including 7 with both infarction and ischaemia). Of patients with ischaemic injury pattern, 66% (27/41) had no past history of coronary disease.
Drs. Mandrola, Foy and Prasad told their readers this damage was “modest” and not a “special reason to worry”.
The felt the real lesson was about science communication. They expressed their “concern about overdiagnosis” in a letter and warned about “hyperbolic messaging.” They wrote:
The broader lesson is that science communication in times of crisis must keep a level head. The public, and decision-makers, need properly controlled studies instead of early sensational reports. In a world where success is measured by clicks, the idea that even mild cases of Covid-19 could pose a new and unprecedented threat to the heart took off. That fear has largely been unsubstantiated, though news of it won’t spread nearly as quickly.
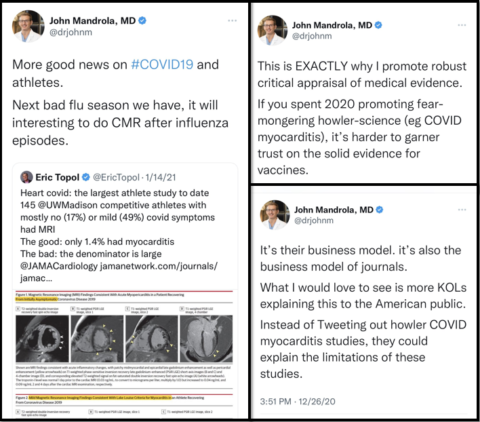
Dr. Mandrola spread this message on social media, warning about “fear-mongering howler-science” studies on COVID-myocarditis. He reacted to the study that showed 1.4% of athletes with COVID had myocarditis by saying this was “good news”.
To summarize, according to medical “conservatives”, myocarditis is “modest” even in “the sickest of the sick”, so long as COVID is the cause. Those who have recovered have “no special reason to worry about their hearts” and anyone who claims otherwise is “fear mongering”. A study showing cardiac involvement in “just” 21 of 3,000 athletes was “reassuring”, and another showing myocarditis in “only” 1.4% of athletes was “good news”. “The evidence for the assertion that a Covid-19 infection is a big heart risk for young people is unconvincing”, Drs. Mandrola and Prasad wrote recently, linking to their article Setting the Record Straight: There is no ‘Covid Heart’ as proof.
Medical “conservatives” implored us to engage in sober, rational analysis regarding COVID. In times of crisis, we must keep a level head.
1.4% of athletes with myocarditis is “good news” and studies on COVID-myocarditis are “fear-mongering howler-science.”
Vaccine-myocarditis
But then something happened that changed everything for so-called medical “conservatives”.
The COVID vaccine was found to cause myocarditis in about 1 in 10,000 adolescent males after their second Pfizer dose. (I discuss vaccine-myocarditis rates here.) It is vanishingly rare in younger children, if it happens at all. If we generously estimate that 10 million adolescent males have been vaccinated, this means that 1,000 boys younger than 18-years have been affected by vaccine-myocarditis, which is slightly higher than the number of children (914) who were hospitalized with COVID in one day during the peak of the Omicron wave. In one (pre-Omicron) study, 38% of hospitalized children were sick enough to be intubated in the ICU.
Though medical “conservatives” protest that the “media” minimizes the clinical course of vaccine-myocarditis, doctors who’ve actually treated these patients and published their findings (like Dr. Frank Han) are in complete agreement about its short-term prognosis. The initial report from Israel said “95% are considered to be mild cases,” and 27 studies from around the world have confirmed this pattern.
The largest systematic review of adolescents and young adults summarized 23 studies involving 854 patients. It found a “low incidence rate and largely favorable early outcomes of COVID-19 mRNA vaccine–associated myopericarditis in adolescents and young adults.” Even in those with abnormal cardiac imaging, a systematic review of 468 cases found that “all reported cases with abnormal cardiac MRI findings showed a favorable clinical course at the acute phase.” Another review of 276 cases reported that, “Fortunately, most myocarditis cases associated with mRNA vaccines are mild in nature and do not have serious complications and require only a few days of hospital admission.” Another systematic review of 22 studies stated “the prognosis of this self-limiting condition is generally good.”
Every study I could find on the clinical course of vaccine myocarditis
Gargano et al.(Morbidity and Mortality Weekly Report) |
Acute clinical courses were generally mild. |
Israel Ministry of Health |
95% are considered to be mild cases. |
Yasuhara et al.(JAMA Pediatrics) |
This systematic review and meta-analysis found low incidence rate and largely favorable early outcomes of COVID-19 mRNA vaccine–associated myopericarditis in adolescents and young adults from a wide range of populations. These findings are reassuring but continued follow-up is warranted. |
Samimisedeh et al.(Journal of Magnetic Resonance Imaging) |
All reported cases with abnormal cardiac MRI findings showed a favorable clinical course at the acute phase. |
Khan et al.(Cureus) |
Fortunately, most myocarditis cases associated with mRNA vaccines are mild in nature and do not have serious complications and require only a few days of hospital admission |
Ling et al.(The Lancet Respiratory Medicine) |
The prognosis of this self-limiting condition is generally good, long-term outcomes for affected patients after 3 months and 6 months are currently awaited. |
Dionne et al.(JAMA Cardiology) |
All patients in this series had a benign course; none required intensive care unit admission. |
Marshall et al.(Pediatrics) |
All 7 patients resolved their symptoms rapidly. |
Woo et al.(Journal of Medical Virology) |
In agreement with previous reports on these patients’ relatively favorable clinical courses, symptoms of all 74 patients in this review resolved, and nearly a third (31.0%) of them recovered with conservative treatment. |
Diaz et al.(JAMA) |
All were discharged after a median of 2 days. There were no readmissions or deaths. |
Jain et al.(Pediatrics) |
Hospital course is mild with quick clinical recovery and excellent short-term outcomes. Myocardial injury and edema are noted on CMR. Close follow-up and further studies are needed to understand the long-term implications and mechanism of these myocardial tissue changes. |
Montgomery et al.(JAMA Cardiology) |
All patients received brief supportive care and were recovered or recovering at the time of this report. |
Rosner et al.(Circulation) |
The clinical course of vaccine-associated myocarditis-like illness appears favorable, with resolution of symptoms in all patients. |
Mevorach et al.(The New England Journal of Medicine) |
All the cases were clinically mild, involving a mean duration of hospitalization of 3.1 days |
Nygaard et al.(The Pediatric Infectious Disease Journal) |
The mild phenotype of myopericarditis cases in our study were comparable with cases described in other studies, except 1 patient with myocarditis and MIS-C, who needed treatment at intensive care unit. |
Witberg et al.(The New England Journal of Medicine) |
Most cases of myocarditis were mild or moderate in severity. |
Mouch et al.(Vaccine) |
The clinical course was mild in all six patients. |
Larson et al.(Circulation) |
All patients had resolution of their chest pain, were discharged from the hospital in stable condition, and were alive with preserved left ventricular ejection fraction at last contact. |
Truong et al.(Circulation) |
Most cases of suspected COVID-19 vaccine myocarditis occurring in persons <21 years have a mild clinical course with rapid resolution of symptoms. Abnormal findings on cardiac MRI were frequent. Future studies should evaluate risk factors, mechanisms, and long-term outcomes. |
Patone et al.(Nature Medicine) |
Most vaccine-associated myocarditis events have been mild and self-limiting. |
Lai et al.(Journal of the American College of Cardiology) |
This study found a significantly lower rate of mortality among individuals with myocarditis after mRNA vaccination compared with those with viral infection–related myocarditis. Prognosis of this iatrogenic condition may be less severe than naturally acquired viral infection–related myocarditis. |
Varma et al.(The Medical Journal of Australia) |
COVID-19 mRNA vaccine-associated myocarditis has a mild, self-resolving clinical course, in contrast to reported complications and long term sequelae associated with COVID-19, such as multisystem inflammatory syndrome in children, and other forms of myocarditis. The long term consequences of myocardial injury with vaccine-associated myocarditis nevertheless warrant further investigation. |
Witberg et al.(The New England Journal of Medicine) |
Our study indicates that BNT162b2 vaccine–induced myocarditis in adolescents appears to be a rare adverse event that occurs predominantly in males after the second vaccine dose. The clinical course appears to be mild and benign over a follow-up period of 6 months, and cardiac imaging findings suggest a favorable long-term prognosis. |
Mansanguan et al.(Tropical Medicine and Infectious Disease) |
The clinical presentation of myopericarditis after vaccination was usually mild and temporary, with all cases fully recovering within 14 days. |
Naveed et al.(Canadian Medical Association Journal) |
Although observed rates of myocarditis were higher than expected, the benefits of vaccination against SARS-CoV-2 in reducing the severity of COVID-19, hospital admission and deaths far outweigh the risk of developing myocarditis |
Mevorach et al.(Circulation) |
The clinical presentation was mild, with resolution of postbooster myocarditis in all cases, as judged by clinical symptoms, inflammatory markers, and troponin levels, ECG, echocardiogram normalization if abnormal (<55% ejection fraction), and a relatively short hospital stay. |
Goyal et al.(QJM: An International Journal of Medicine) |
Myocarditis following COVID-19 vaccination is often mild, seen more commonly in young healthy males and is followed by rapid recovery with conservative treatment. |
Gao et al.(American Journal of Preventative Medicine) |
Although an increased risk of myocarditis and pericarditis was found among individuals who received COVID-19 vaccine, it is worth noticing that myocarditis or pericarditis was predominantly mild in the vaccinated individuals. |
COVID myocarditis versus vaccine myocarditis: Severity
Several studies have compared clinical outcomes between vaccine-myocarditis, classic viral myocarditis, and myocarditis caused by multisystem inflammatory syndrome in children (MIS-C), a potentially devastating COVID complication that has affected over 9,300 American children, 9 times more than the number of children who’ve developed vaccine-myocarditis.
Though Drs. Mandrola, Foy and Prasad, neglected to mention MIS-C in their article on “COVID heart”, myocarditis and coronary artery aneurysms frequently occur in children with MIS-C. Other studies have reported acute heart failure in children with MIS-C. Other cardiac complications of myocarditis due to MIS-C include “shock, cardiac arrhythmias, pericardial effusion, and coronary artery dilatation”. Cardiac arrhythmias have led “to hemodynamic collapse and need for ECMO support” in some children. Though most children recover well, 76 children have died of MIS-C.
One review that compared vaccine-myocarditis, classic viral myocarditis, and myocarditis caused by MIS-C, found that vaccine-myocarditis was the mildest of the three. It said:
Compared with classic myocarditis, those with MIS-C myocarditis had better clinical outcomes, including rapid recovery of cardiac function. Patients with vaccine-related myocarditis had prompt resolution of symptoms and improvement of cardiac function.
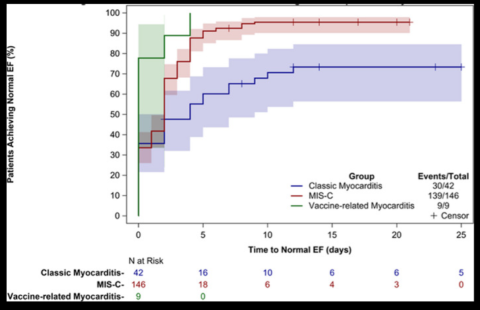
Patients with vaccine-myocarditis recover faster than children with MIS-C-myocarditis
Another study “reviewed the data of 42 COVID‐19‐related myocarditis patients from two systematic reviews and compared the outcomes with 74 patients” with vaccine-myocarditis. It found:
The number of patients who experienced complications or required intensive care was significantly lower among the mRNA vaccine‐related myocarditis patients. Furthermore, there was no mortality reported among the mRNA vaccine‐related myocarditis patients, and more patients recovered without myocarditis‐specific medical treatments.
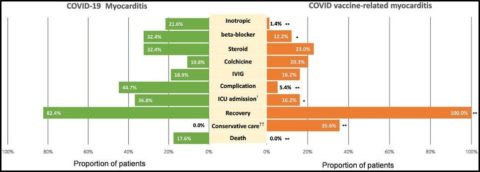
Patients with vaccine-myocarditis far better than those with COVID-myocarditis
Additionally, there is emerging evidence that COVID can damage the heart beyond acute myocarditis. Though medical conservatives reflexively deride studies whose results they don’t like as “fear mongering howler science”, one study found “that heart attack death rates took a sharp turn and increased for all age groups during the pandemic.” According to one article:
The spikes in heart attack deaths have tracked with surges of COVID-19 infection—even during the presumed less-severe Omicron phase of the pandemic. Furthermore, the data showed the increase was most significant among individuals ages 25-44, who are not usually considered at high risk for heart attack.
“The dramatic rise in heart attacks during the pandemic has reversed what was a prior decade long steady improvement in cardiac deaths,” said Yee Hui Yeo, MD, first author of the study and a Cedars-Sinai physician-scientist. “We are still learning the many ways by which COVID-19 affects the body, regardless of age, gender, ethnicity or race.”
Dr. Yeo is right to take a medically conservative approach towards a brand new virus. We’ll be learning about the effects of repeat COVID infections on our brain, lungs, and heart for the rest of our lives. Only a medical radical would suggest repeatedly exposing unvaccinated children to a novel virus and hoping for the best.
COVID myocarditis versus vaccine myocarditis: Frequency
COVID myocarditis is more frequent than vaccine-myocarditis, even for young males. One study found that:
Among males aged 12 to 17 years, the incidence of myocarditis or pericarditis after infection with SARS-CoV-2 was about twice as high as after vaccination with 2 doses of an mRNA-based COVID-19 vaccine. When MIS, a post–COVID-19 syndrome that often includes cardiac complications, was included in the comparison, the risk of cardiac problems was about 2 to 6 times higher after infection than after 2 doses of vaccine. Men aged 18 to 29 years had a 7 to 9 times greater risk of cardiac complications after infection than after 2 doses of vaccine.
Though he claims otherwise on social media and his writing for the general public, in his review on the topic, even Dr. Prasad was forced to concede that:
The incidence of myocarditis found for young men after SARS-CoV-2 infection is larger than what we found for myocarditis following COVID-19 vaccination.
I’ve not seen him acknowledge his own finding elsewhere.
A blatant double standard
Looking at all of this, it’s hard to conclude that the vaccine poses a bigger risk to the heart than the virus, though of course, COVID’s harms are not limited to myocarditis. This is why pediatric hospitals were deluged with sick children during the Delta and Omicron waves, while no hospital in the world had to open a vaccine-injury unit. Over 2,000 children have died from COVID in the US, double the number of children who’ve been affected by vaccine-myocarditis. As far as I know, no children have died from the vaccine, which has proven effective in limiting COVID’s gravest harms in children, including MIS-C and death. Many more children would have suffered had no efforts been made to protect them from COVID as some medical “conservatives” advocated.
Nonetheless, because I value consistency in my writing, I’ve said many times that it’s serious whenever a young person is hospitalized with vaccine-myocarditis, even if nearly all of them leave after a couple of days feeling fine. Though it is very rare, some patients can be quite sick and not all recover immediately. A small number of adults around the world have died from this disorder. These are tragedies. Most individuals are advised to abstain from vigorous activity for several months, and they will have to be monitored over the long-term for possible cardiac scarring and arrhythmias. So, while vaccine-myocarditis shouldn’t be minimized, a doctor who says its prognosis is “usually mild and temporary” would only be honestly reporting what literally every study on the topic has reported thus far.
Medical “conservatives” felt otherwise. Dr. Mandrola told his Twitter audience it would be inappropriate for doctors to accurately report these results. He felt that to maintain “trust”, doctors had to both minimize the risk of COVID and exaggerate the harms of the vaccine. This is because medical “conservatives” have an absurd and blatant double-standard for how they evaluate harms of the virus versus harms of the vaccine.
- Though Drs. Prasad and Mandrola felt that “Even in the sickest of the sick, Covid-19’s effect on the heart appears to be modest,” they felt “even the slightest bit of inflammation in the heart should be treated seriously” when the vaccine was to blame.
- They wrote that wrote that people who have recovered from COVID “have no special reason to worry about their hearts”. However, they warned the vaccine could “scar tissue created in response to heart inflammation can be the source of the rhythm disturbance”.
- With COVID-myocarditis, they discouraged unnecessary tests and even signed a “letter of concern about overdiagnosis”. With the vaccine, Dr. Prasad warned that “subclinical myocarditis is often far greater than reported myocarditis”.
- While they felt “The issue of Covid-19 induced cardiac problems was massively overblown,” Dr. Mandrola wrote that “vaccine-induced myocarditis concerns demand respect”.
- Though they wrote with COVID-myocarditis, we “need properly controlled studies instead of early sensational reports,” they were eager to amplify early sensational reports about vaccine-myocarditis. “I don’t think people realize the damage continuing to push 2 doses in young men will do,” Dr. Prasad tweeted, one month after warning us to avoid “hyperbolic messaging” about COVID-myocarditis.
- Dr. Mandrola dismissed the idea that “even mild cases of Covid-19 could pose a new and unprecedented threat to the heart”. However, when discussing the vaccine he said, “Humans have only one heart; inflaming it at a young age is not a small thing”.
- Dr. Prasad said 21 of 3,000 patients with COVID-myocarditis was “reassuring”. When discussing the much lower rate of vaccine-myocarditis, he said “That 1/3-5k ballpark is deeply concerning”. “We ought to make a concerted effort to lower harms in this group”, he said about the vaccine, of course.
- Dr. Mandrola felt concerns about COVID-myocarditis were “fear mongering”, and that it was “good news” that 1.4% of athletes developed COVID-myocarditis on cardiac MRI. Good news! In contrast, with the vaccine and a myocarditis rate of 0.01%, he said we need more “caution” and that accurately quoting studies that describe vaccine-myocarditis as “mild” was a “trust shredder”.
- “The point is that the risk of COVID in this age group is super low, as is the risk of vaccine-induced myocarditis”, Dr. Mandrola said, implying an equivalency between vaccine side-effects and death.
- Though Dr. Mandrola had previously argued for “robust critical appraisal of medical evidence” when discussing COVID-myocarditis, he responded to someone who provided accurate information about COVID’s harm to children by saying:
“I think we can avoid being too quantitative”.
Yes, one can avoid being too quantitative, but this is not a goal to strive for.
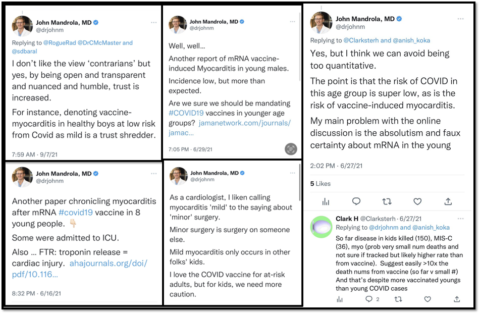
Dr. Mandrola warns us to not to be “too quantitative” when discussing COVID.
And that’s how it always has been with these doctors. Vaccine side-effects were treated as a life-altering catastrophe for masses of adolescents, while anything the virus did to young people was brushed off as “fear mongering” – and yes, this includes children and young adults dying from COVID. I previously discussed Dr. Prasad’s horrifying admonition that we should casually accept unvaccinated children dying of COVID as a “matter of course”.
He was not alone. In December 2020, after thousands of young adults had already died, none were vaccinated, and the majority had yet to be infected, Drs. Mandrola and Foy wrote an article titled “No, Young Adults Should Not Live in Fear from Coronavirus“. The core of their argument was that “the infection fatality rate for young adults is quite low”. In other words, not that many young people will die of COVID. They said a “fear of death” was not a valid reason for young adults to avoid the virus. Sure, “an excess of 12,000 deaths sounds bad” they wrote, but it’s just a “tiny absolute increase in risk”. They felt our focus should be on all the people who didn’t die. They wrote:
Thus, the individual risk for a person this age is found by dividing 4,560 (the number dead from COVID19 in this study) by 88 million. This equates to a 0.0052% risk of dying from COVID19.
Of course, anything that kills young people could be minimized this way. Currently, over 43,000 Americans ages 19-44 years have died of COVID, and the vast majority would be alive had they been vaccinated and boosted. Even though this is 6 times the number of soldiers who’ve died fighting in wars since 9/11, Drs. Mandrola and Foy told them not to fear this outcome. Moreover, death is not the only bad outcome from COVID, though Drs. Mandrola and Foy and didn’t even mention COVID’s non-fatal harms.
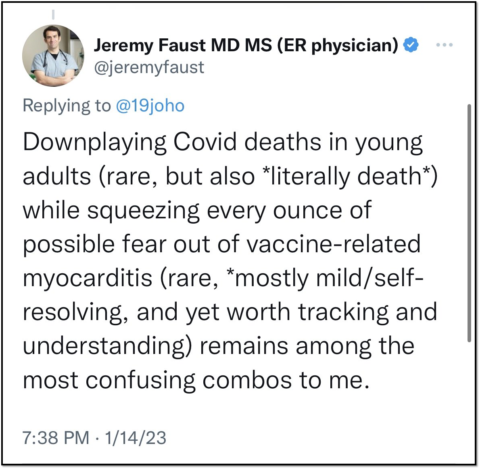
I too am confused
It does not make much sense to me that doctors who feel this way about thousands of dead young people, instead feel the need to warn them about something that has killed a small number of young adults around the world. However having told young people not to fear death or anything else COVID might do to them, medical “conservatives” instead felt they should be very afraid of vaccine-myocarditis. No longer were we told to calculate “the individual risk for a person this age”, and anyone who did so would be accused of minimizing this side effect. Even though virtually no teenagers are getting vaccinated today, and it’s plausible there are no children in the hospital with vaccine-myocarditis, medical “conservatives” retain their laser-like focus on this side effect.

Dr. Prasad has some thoughts on vaccine-myocarditis
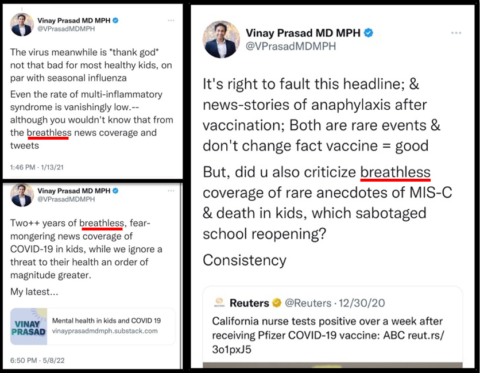
In contrast, even though medical “conservatives” declared the pandemic over multiple times, children are still getting sick with and very rarely dying of COVID. However, could you ever imagine Dr. Prasad or any medical “conservative” making a video about a child who died of COVID or spent 160 days on a ventilator? Of course not. Medical “conservatives” overtly and consciously do not acknowledge such children, even though there are many more of them. Dr. Prasad even suggested there was something fundamentally wrong with anyone who shared basic facts on pediatric COVID. He always said they were breathless. This was an artistic critique. He did not like their tone.
In fact, Dr. Prasad complained that children seriously injured by COVID received too much media attention. He said providing accurate information to parents only “sabotaged school reopenings”. In April 2021 he said that the “media’s breathless coverage of MIS-C and variants has been a disservice”. The Delta and Omicron variants would rip through the pediatric population the next year, causing unprecedented illness, especially for unvaccinated children. Many misinformed parents were under the illusion it was “just the flu” and some of their children really suffered. “I just had a false sense of security that it was just like the flu and it wasn’t that serious. Obviously it is that serious and it was that serious. Now, I can see,” said one mother whose unvaccinated child wound up on a ventilator. Yet, Dr. Prasad felt that parents like her had been overly-informed about COVID’s risk to children. Imagine that.
In contrast, he excoriated The Atlantic for not covering “the human story of a 22 year boy with myocarditis.” “There is little to no coverage of a serious, proven AE (adverse event) in young healthy people,” he said. “It won’t be pretty,” he added, breathlessly.
Reality check: COVID has killed about 1,850 more children than the flu since the start of the pandemic.
Trust in medicine
I believe the gravity of a medical condition be judged primarily based on the frequency/severity of the injury that results, rather than its underlying cause. I also don’t think vaccine-myocarditis is a fate worse than death. Medical “conservatives” disagree. Nonetheless, I always like to find points of agreement with the doctors I discuss, and Dr. Mandrola was right about the importance of trust in medicine.
Doctors who repeatedly and blatantly contradict themselves are motivated by ideology, not evidence. They don’t deserve our trust.