{kind=link}
In a previous article, I described how silly it was for doctors to demand a million-child randomized-controlled trial of children under the age of 5 years in the middle of a raging pandemic. I also mocked the idea that the best way to maintain trust in routine pediatric vaccinations was to misinform people about the COVID vaccine for children. I’d like to explore two more silly reasons doctors have given for leaving unvaccinated babies vulnerable to COVID.
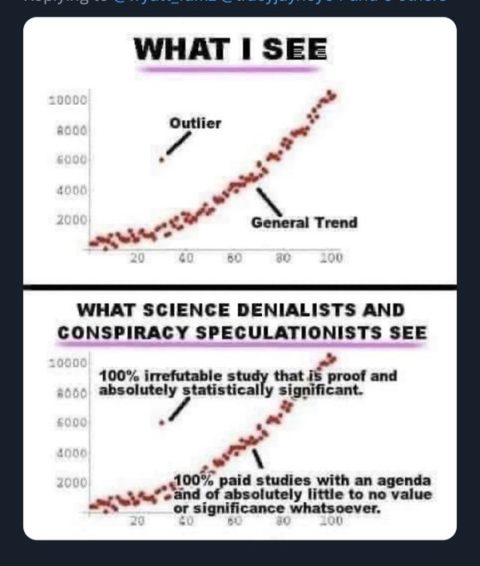
For part 1, I will remind you of a previous article where I described how contrarian doctors selectively report and omit information to minimize pediatric COVID and frighten parents about vaccines. There has been a deluge of research throughout the pandemic, and it’s not hard to find one or two studies that support any preconceived viewpoint, even if these studies are outliers from the general trend. It’s also really easy just to not mention unwanted facts, namely that COVID can be really bad for a very small percentage of children, that rare tragedies add up to non-trivial numbers when tens of millions of children get COVID, and that the vaccine isn’t perfect, but it has consistently been shown to limit COVID’s harms for children.
Honest brokers do their best to report the totality of the evidence. However, by cherry-picking only the studies that advance their agenda and refusing to share unwanted facts, doctors who don’t care for sick children can misinform parents to increase the numbers of unvaccinated children who contract COVID. Two recent articles by familiar names demonstrate this misleading technique.
Vaccine myocarditis: Rate
With this in mind, let’s review the latest information on vaccine-myocarditis. Vaccine-myocarditis most commonly occurs in adolescent and young-adults males several days after their second vaccine dose. Most, but not all, studies found a higher rate with Moderna compared to the Pfizer. Until last month, only the Pfizer vaccine was authorized for children in the US. Below are the rates of vaccine-myocarditis for young males after their second dose of the Pfizer vaccine, except where noted otherwise. (If I learn of other studies, I will add them).
- USA: 1 in 2,650, 12-17 years
- Hong Kong: 1 in 2,700, 12-17 years
- USA (Vaccine Safety Datalink): 1 in 6,800 12-17 years, no statistical signals for children 5-11 years
- Meta-analysis: 1 in 7,200-20,000, 12-17 years with “low certainty” after an mRNA vaccine
- Israel: 1 in 9,350, 16-29 years
- Denmark: 1 in 10,000 12-17 years, either vaccine dose
- Israel: 1 in 12,000 12-15 years
- Ontario: 1 in 12,300, 12-17 years
- USA (VAERS): 1 in 13,000 16-17 years, 1 in 21,500 12-15 years, 1 in 400,000 5-11 years
- USA: 1 in 16,600, 12-17 years
- Nordic registry data: 1 in 17,500, 16-24 years
- Nordic Countries: 1 in 18,200, 16-24 years
- Singapore: 1 in 20,700, 12-19 years (includes myocarditis/pericarditis and Pfizer/Moderna)
- French national health system (Epi-phare): 1 in 38,500, 12-29 years
- France: 1 in 52,300, 12–17 years
- UK: 1 in 71,000 under 18 years (males and females, first or unknown dose), 1 in 100,000 (males and females, second dose)
- Denmark: No increased risk for males
In case you missed it, I’ll highlight that one American vaccine-safety monitoring found a rate of 1 in 400,000 for males 5-11 years, while the other found no “statistical signals” for this age. According to one CDC report, after 8.7 million Pfizer doses given to children ages 5-11, there were only 11 cases of myocarditis. Seven of the children had recovered and 4 were “recovering”. Additionally, it’s now well-known that the rate can be greatly reduced by spacing out the vaccine doses. A study from Ontario found a rate of 1 in 100,000 for adolescent boys with an extended interval between doses.
As virtually no children older than 5 (slide 20) are receiving their second vaccine now, many more cases have already happened than will happen in the future. I’m confident the number of times I’ve discussed this topic exceeds the number of children currently hospitalized with it, which plausibly is zero. Several other doctors can say this as well.
Vaccine myocarditis: Clinical course
While there is clearly great variability regarding the rate of vaccine-myocarditis, the clinical course entirely consistent across all studies. Affected children feel chest pain, shortness of breath, palpitations, and fatigue. Nearly all are hospitalized, and there are markers of cardiac inflammation on routine tests. While it’s never a trivial matter when a child is hospitalized, most leave feeling fine after a couple days. All studies report the condition is nearly always mild, with a good outcome:
- “All patients in this series had a benign course; none required intensive care unit admission” (Dionne)
- “All 7 patients resolved their symptoms rapidly” (Marshall)
- “All were discharged after a median of 2 days. There were no readmissions or deaths” (Diaz)
- “Hospital course is mild with quick clinical recovery and excellent short-term outcomes” (Jain)
- “All patients received brief supportive care and were recovered or recovering at the time of this report” (Montgomery)
- The clinical course of vaccine-associated myocarditis-like illness appears favorable, with resolution of symptoms in all patients” (Rosner)
- ” All the cases were clinically mild” (Mevorich)
- “Acute clinical courses were generally mild” (Gargano)
- “The mild phenotype of myopericarditis cases in our study were comparable with cases described in other studies, except 1 patient with myocarditis and MIS-C, who needed treatment at intensive care unit” (Nygaard)
- “Most cases of myocarditis were mild or moderate in severity” (Witberg)
- “The clinical course was mild in all six patients” (Mouch)
- “All patients had resolution of their chest pain, were discharged from the hospital in stable condition, and were alive with preserved left ventricular ejection fraction at last contact” (Larson)
- “Most cases of suspected COVID-19 vaccine myocarditis occurring in persons <21 years have a mild clinical course with rapid resolution of symptoms” (Truong)
- “95% are considered to be mild cases” (Israel Ministry of Health)
- “Most vaccine-associated myocarditis events have been mild and self-limiting” (Patone)

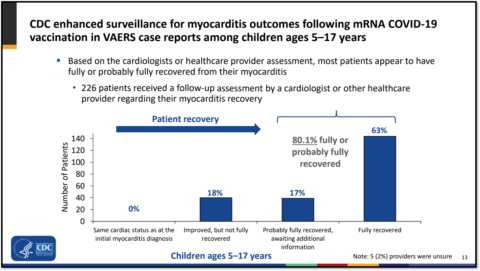
While this is good news, a very small number of children have needed treatment in the ICU or have not fully recovered. Though they seem headed in that direction, they will likely face restrictions with vigorous activity until they do. While the condition should not be minimized for these reasons, the long-term clinical picture looks mostly encouraging as well. According a recent CDC report/a>,
At least 90 days after myocarditis diagnosis, most patients who were reached reported no impact on their quality of life, and most did not report missing school or work.
Radiographic abnormalities (late gadolinium enhancement) have been found on follow-up cardiac MRI several months later in several studies. While these parameters were improved from baseline, their clinical significance is unknown. As such, affected individuals will have to have their cardiac status monitored over time. Though there have been some fatalities associated with mRNA vaccines, most occurred in adults older than 50. 23.3 million American children have received two vaccine doses, and there are no clear fatalities as far as I know.
Risk versus benefits
Obviously, the risk of the vaccine has to be viewed in the context of its benefits. Because they consider both the risks and benefits, nearly all pediatricians, including cardiologists, continue to strongly advocate for pediatric vaccination. As they work with sick children, they know that their hospitals have been deluged with COVID patients at times, but none have opened a vaccine-injury ward. That’s why they are “alarmed” at low pediatric vaccination rates. This is in contrast to the doctors I criticize who believe “natural immunity” will protect children, though enough children remain vulnerable that over 300 are being hospitalized with COVID daily.
Fortunately, the vaccine continues to limit these severe outcomes, even with Omicron. This includes the vaccine’s ability to prevent MIS-C, which can cause much a more severe myocarditis in 75% of affected children. (Happily MIS-C seems to have vanished for now). Several studies (here and here) have found the vaccine’s benefits outweigh the risks for all age and sex subgroups, though this could change if new variants escape our current vaccines.
Cherry-picking
What relevance does any of this have to vaccinating children younger than 5 years? Most pediatricians would answer “none at all”, given the extremely reassuring data from children ages 5-11 years and that younger children will receive a lower vaccine dose. If the vaccine is routinely given to young children, they might need fewer shots when they are older and most vulnerable to vaccine-myocarditis.
Unfortunately, not all doctors felt the need to communicate this information in an informative, nuanced way when discussing the vaccine for young children.
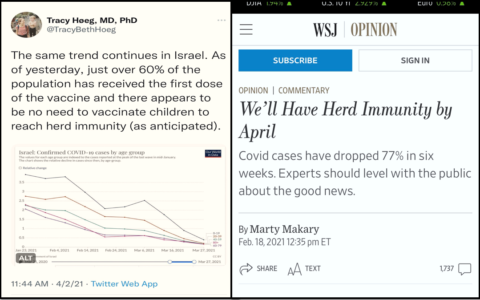
Dr. Marty Makary, who said we had reached herd immunity over a year ago, warned:
The small size of the studies in children under 5 makes it nearly impossible to observe rates of rare complications such as myocarditis, which occurs in 1 in 2,650 12-17 year-old boys after the 2nd dose. This complication has been associated with EKG changes in children and even concerning MRI findings months after recovering from myocarditis. The New England Journal of Medicine reported one case of vaccine-associated myocarditis death in a 22-year-old in an Israeli population study. Keep in mind that babies can’t tell you when they have myocarditis.
Dr. Tracy Hoeg, who suggested last year that pediatricians were confusing COVID and RSV, similarly wrote:
The trials, in other words, enrolled only a fraction of the number of participants that would have been required to determine efficacy against end points like severe disease, hospitalization, and rare adverse events such as myocarditis, which has been linked to COVID vaccination in males in the 12- to 17-year-old age group at a rate of up to 1 in 2,700.
The cherry has been picked.
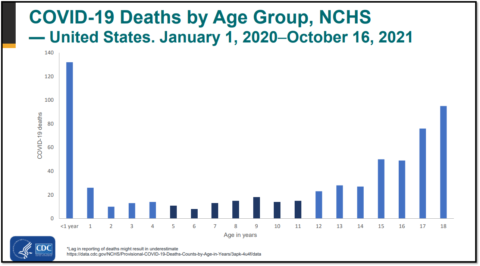
Did Drs. Makary and Hoeg reference these particular studies because they had the strongest methodology? Of course not. They shared them as established fact for one reason only – they had the highest rate of vaccine-myocarditis. The many larger studies showing lower rates, especially for children ages 5-11, were unmentionable. Similarly, because the vaccine-myocarditis almost always has a favorable prognosis, neither doctor reported this, though the death of a 22-year-old in Israel was used to scare parents. The fact that babies have the highest risk of dying from COVID and that over 500 children younger than age 5-years have died so far was also unmentionable. All harms of the virus are unmentionable, as is all evidence that the vaccine can limit these harms.
While at least Drs. Makary and Hoeg shared an accurate number, which was by no means certain given their previous work, here’s why this cherry-picking matters. Very few people who read their essays will know they were only told a very small fraction of the relevant information. The governors they advise (Florida, Virginia) are likely similarly ignorant. And so, many people are now wildly misinformed, and some politicians are recommending against vaccinating children.
In early 2021, Drs. Makary and Hoeg both felt herd immunity was just around the corner and so there was no need to vaccinate children. Rather than say “I was wrong”, their goal now is to frighten parents by casting the vaccine in the worst possible light and to pacify them by casting the virus in the best possible light. Judging by the abysmal vaccination rate for young children, they’ve succeeded. As pediatric hospitalizations creep upwards once again, nearly matching the Delta peak of last summer, they should visit a children’s hospital and take a well-deserved victory lap.