
{kind=link}
“We should remain like a neutral judge. Always. The people can decide the best policy.”
On Friday, I discussed an article by a so-called “medical conservative”, Dr. John Mandrola, titled Politics and Medicine is a Bad Idea. In it, Dr, Mandrola warned doctors of venturing into policy debates. He said:
Scientists and clinicians have important meaningful jobs. We harm our ability to succeed when we delve into matters of policy. It distracts and sows distrust. We should remain like a neutral judge. Always. The people can decide the best policy.
He cautioned medical professionals not to “overstep our expertise” and to not delve into certain matters of policy.
In my response, I noted that Dr. Mandrola exempted himself from the standards he set for other doctors and was perfectly willing delve into matters of policy. In an article titled from December 2022 titled How Myocarditis Influences Vaccine Mandate Decisions he said:
Now we can combine these statements to consider the decision to coerce young people to take additional vaccine shots—as is being done on many US college campuses and in the military…In 2022, SARS-CoV-2 vaccine mandates are wrong, and I oppose them.
This article is worth examining further, not just because predictably mislead its readers about COVID and the COVID vaccine, but rather because it ironically proved the wisdom of Dr. Mandrola’s warning that doctors should not let favored policy goals affect how they communicate science.
“Before 2019, everyone lived with a low baseline risk of viral myocarditis. We did so because it was not a modifiable risk. The risk of myocarditis from a mRNA vaccine is modifiable.”
Dr. Mandrola began his article with a review of myocarditis in general. He said:
In most cases, this resolves with supportive care and rest. In some cases, it does not resolve. And the heart can fail.
Dr. Mandrola linked to a report of two patients in their 40s with severe myocarditis after the vaccine. One patient died, tragically, though he didn’t even develop symptoms until two weeks after his second vaccine dose.
In contrast, Dr. Mandrola said the virus presented a negligible threat. He said:
In late 2022, a young person (without severe health issues) has a near-zero risk from SARS-CoV-2. They were very low risk in 2020-2021, but it’s even lower now…The pneumonias and severe COVID-19 illness are nearly gone.
The crux of Dr. Mandrola’s argument was this:
You can’t avoid myocarditis from viral infection. There are many viruses that can lead to myocarditis. It’s not only SARS-CoV-2. Before 2019, everyone lived with a low baseline risk of viral myocarditis. We did so because it was not a modifiable risk.
The risk of myocarditis from a mRNA vaccine is modifiable.
Dr. Mandrola also reported “one final fact”:
SARS-CoV-2 vaccination does not prevent infection nor stop transmission.
“People infected with COVID-19 before receiving a vaccine were 11 times more at risk for developing myocarditis within 28 days of testing positive for the virus. But that risk was cut in half if a person was infected after receiving at least one dose of a COVID-19 vaccine.”
Dr. Mandrola’s analysis was flawed on multiple levels.
First, Dr. Mandrola treated myocarditis as a single entity, whether the cause was a virus or the vaccine. In reality, doctors who’ve treated patients with vaccine-myocarditis and published on the topic universally report that it is nearly always mild and short lived, especially compared to viral-myocarditis. One study, which was published before Dr. Mandrola wrote his essay, compared COVID vaccine-myocarditis to viral-myocarditis recorded before the pandemic. It found:
A total of 866 patients were included for analysis. Over the follow-up period, 1 death (1.0%) of 104 patients with postvaccination myocarditis and 84 deaths (11.0%) of 762 patients with viral infection–related myocarditis were identified. One case (1.0%) of dilated cardiomyopathy and 2 cases (1.9%) of heart failure were identified in the postvaccination group, compared with 28 (3.7%) and 93 (12.2%) in the viral infection–related myocarditis group.
That study concluded:
A significantly lower rate of mortality among individuals with myocarditis after mRNA vaccination compared with those with viral infection–related myocarditis. Prognosis of this iatrogenic condition may be less severe than naturally acquired viral infection–related myocarditis.
Dr. Mandrola didn’t tell this to his readers, and subsequent studies have since shown:
Compared with myocarditis associated with covid-19 disease and conventional myocarditis, myocarditis after vaccination with SARS-CoV-2 mRNA vaccines was associated with better clinical outcomes.
Another study, which was published before Dr. Mandrola wrote his essay, specifically examined COVID myocarditis. It found:
Hospital mortality was more than sixfold higher in patients with myocarditis and COVID-19 compared to those with myocarditis but without COVID-19.
Dr. Mandrola didn’t tell this to his readers either.
Instead he told them about a study that found “post COVID-19 infection was not associated with either myocarditis or pericarditis.” That’s right, Dr. Mandrola thought his readers should know about myocarditis in patients who were “post COVID-19 infection”, not in patients with active COVID. Additionally, Dr. Mandrola, who previously warned about “overdiagnosis” with regards to COVID, tried to scare his readers by letting them know that some people have abnormal blood tests after vaccination, even though they feel totally fine.
Second, while the vaccine has risks, it also has many benefits, none of which Dr. Mandrola mentioned. Dr. Mandrola was right when he said “The risk of myocarditis from a mRNA vaccine is modifiable”- if one forgoes the vaccine. But this comes with an obvious trade-off, forgoing its benefits. Telling patients the “risks of no treatment” is a core of the process of informed consent. The stakes can be high for some people.

Read this article here.
It turns out, thanks to the vaccine, that the risk of myocarditis from SARS-CoV-2 is also modifiable. One study, which was published before Dr. Mandrola wrote his essay, examined 43 million people 13 or older who received at least one dose of a COVID vaccine. It found:
People infected with COVID-19 before receiving a vaccine were 11 times more at risk for developing myocarditis within 28 days of testing positive for the virus. But that risk was cut in half if a person was infected after receiving at least one dose of a COVID-19 vaccine…The risk of myocarditis associated with the vaccine was lower than the risk associated with COVID-19 infection before or after vaccination – with one exception. Men under 40 who received a second dose of the Moderna vaccine had a higher risk of myocarditis following vaccination.
Dr. Mandrola said, “You can’t avoid myocarditis from viral infection”, and if one accepts that COVID infections are inevitable, this obviously greatly strengthens the case to get vaccinated. Dr. Mandrola didn’t share any of this information with this readers, and instead falsely told them viral-myocarditis was “not a modifiable risk”.
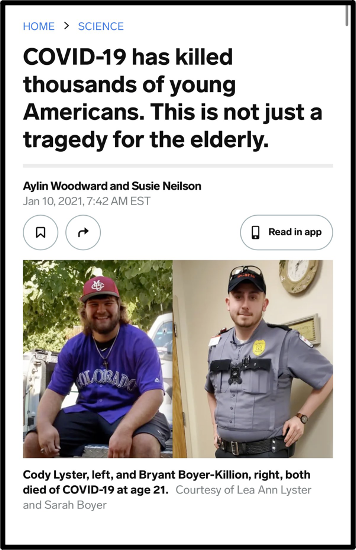
Third, COVID’s harms are not limited to myocarditis. Though Dr. Mandrola said young people had a “near-zero risk” from COVID, there’s a world of difference between zero and near-zero given that many millions of young people have contracted COVID. Consequently, COVID has killed thousands of young men, those most at risk for myocarditis, and it has seriously injured countless more. Young people have suffered strokes, amputations, and long COVID. The vaccine isn’t perfect, but it saved many young people much needless suffering.
Dr. Mandrola didn’t didn’t share any of this information with this readers, but instead used his personal experience as evidence, saying:
Another thing I saw first-hand: there were almost no college-aged persons with COVID-19 who needed oxygen or ventilators. SARS-CoV-2 has a steep age gradient for severe disease.
Read this article here.
Finally, while COVID vaccination “does not prevent infection nor stop transmission”, its effect on these metrics isn’t zero. One study, which was published before Dr. Mandrola wrote his essay, found:
After a third dose, estimated vaccine effectiveness against Omicron was 61% for symptomatic infection.
Dr. Mandrola didn’t didn’t share this information with this readers.
Another study, which was published before Dr. Mandrola wrote his essay:
Analysed data on more than 22,000 confirmed cases of SARS-CoV-2 infection across California’s 35 adult prisons over a 5-month period starting at the end of 2021, when the first wave of Omicron began ripping through the United States.
It found that:
Among individuals with COVID-19, those who received at least one vaccine shot were 24% less likely to infect close contacts— in this case cellmates — compared with unvaccinated prisoners
That’s not great, but it’s not nothing. Dr. Mandrola didn’t didn’t share this information with this readers either.
“In 2022, SARS-CoV-2 vaccine mandates are wrong, and I oppose them.”
Dr. Mandrola said “In 2022, SARS-CoV-2 vaccine mandates are wrong, and I oppose them”. He claimed that a core reason was, “The pneumonias and severe COVID-19 illness are nearly gone.” Though Dr. Mandrola framed his opposition to vaccine mandates largely as a reflection of the improved COVID landscape of December 2022, his opposition did not begin on that date.
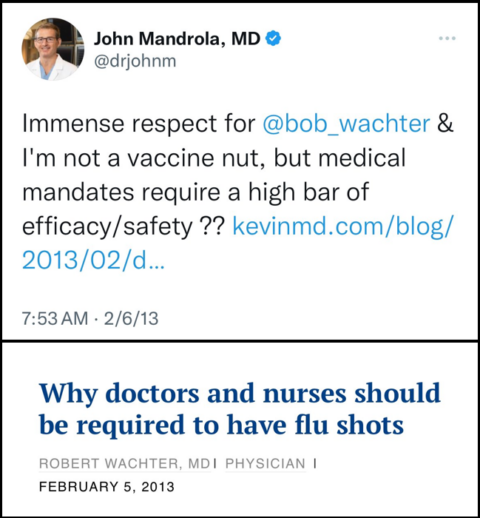
Prior to the pandemic, he “just asked questions” about vaccines mandates. He continued to denigrate vaccines mandates in 2021 (here, here, and here), only months after COVID vaccination began. “Colleges should be rethinking vaccine mandates”, he said in July 2021, based on the “results” of a poll on social media. The Delta variant arrived immediately thereafter, causing “pneumonias and severe COVID-19 illness” in young people, especially unvaccinated ones.
And thus it becomes clear: In 2022, when Dr. Mandrola wrote his essay opposing vaccine mandates, he started with his long-standing political opinion- vaccine mandates are wrong- and worked backward to selectively present only the “evidence” that supported his preferred policy.
Just asking questions!
To be clear, I am not arguing in favor of vaccine mandates, especially given their middling impact on viral transmission. In fact, beyond noting that frontline healthcare workers generally supported mandates for frontline healthcare workers, I’ve can’t recall publicly giving my opinion on the subject. I generally try to avoid blending politics and medicine.
But, I can’t stop thinking about this paragraph:
Scientists and clinicians have important meaningful jobs. We harm our ability to succeed when we delve into matters of policy. It distracts and sows distrust. We should remain like a neutral judge. Always. The people can decide the best policy.
The people can decide the best policy, but only if they have the best information. Doctors who prioritized politics over being a “neutral judge” failed to provide the best information. As Dr. Mandrola said, “Another downside of these forays into policy is the possibility of reducing trust—which is already at a low level”.
Indeed.