
{kind=link}
Earlier this month, a large multinational research group published a study in the journal Vaccine using the Global Vaccine Data Network (GVDN) to examine thirteen medical conditions that the group considered “adverse events of special interest” potentially associated with COVID-19 vaccination. In the study, they examined the records of more than 99 million vaccinated individuals in eight countries, with the intention of identifying higher-than-expected cases of one or more of these conditions after a COVID-19 vaccination. The vaccines investigated included the most commonly used vaccines, the mRNA-based vaccines distributed by Pfizer and Moderna, as well as nonreplicating adenovirus vector-based vaccines. and protein-based vaccines. The GVDN network includes Argentina, Australia – New South Wales, Australia – Victoria, Canada – British Columbia, Canada – Ontario, Denmark, Finland, France, New Zealand, and Scotland, and the healthcare data studied was comprised of either individual- or population-level data, depending on the availability in the study sites. Overall, it was a massive undertaking that also belies the frequent antivax lie that vaccines aren’t studied for safety and efficacy.
It’s also a good case study to show how antivaxxers spin even a study that shows—as this study did—specific vaccines to be quite safe, with only rare serious adverse events associated with them, into antivax propaganda used to fear monger about vaccines. The way they do this is through two tactics. One is to falsely portray the risk-benefit ratio of vaccines as unacceptable by falsely decreasing the denominator (the benefit) by claiming that the vaccines have little or no benefit. The other is through the Nirvana fallacy, in which any deviation from a perfectly safe vaccine with zero adverse events is used to portray the vaccine as hopelessly dangerous. In the two weeks since this study was published, I’ve seen antivaxxers doing both and therefore thought that a discussion of this study and the antivax reaction to it would be useful to our readers. The reality-based interpretation of the study is that it is yet more evidence that the benefits of COVID-19 vaccination far outweigh the tiny risks of serious adverse events. The antivax interpretation is, of course, that COVID-19 vaccines are dangerous, toxic sludge.
Let’s dig in.
99 million patient records, and this is all GVDN found
Given the size and the scope of the study, first let’s reproduce the chart showing which vaccines were studied:
Table 2. Total number of vaccinations by brand.
| Vaccine platform | Vaccine brand | Total doses |
|---|---|---|
| Inactivated | Covilo or SARS-CoV-2 Vaccine (Vero Cell) [Sinopharm (Beijing)] | 134,550 |
| Covaxin [Bharat Biotech] | 1,660 | |
| CoronaVac or Sinovac [Sinovac Biotech] | 31,598 | |
| Inactivated (Vero cell) [Sinopharm (Wuhan)] | 623 | |
| Nucleic acid-based | Comirnaty or Riltozinameran or Pfizer/BioNTech COVID-19 Vaccine Bivalent [Pfizer/BioNTech] | 3,516,963 |
| Comirnaty or Tozinameran [Pfizer/BioNTech or Fosun-BioNTech] | 183,677,660 | |
| Comirnaty or Tozinameran Paediatric [Pfizer/BioNTech or Fosun-BioNTech] | 2,439,086 | |
| Spikevax bivalent Original/Omicron [Moderna] | 2,750,476 | |
| Elasomeran or Spikevax or TAK-919 Half Dose [Moderna or Takeda] | 400,395 | |
| Elasomeran or Spikevax or TAK-919 [Moderna or Takeda] | 36,222,514 | |
| Protein-based | MVC-COV1901 [Medigen] | 16 |
| Covovax or Nuvaxoid [Novavax or Serum Institute of India] | 66,856 | |
| Non-replicating viral vector | Convidecia or Convidence [CanSino] | 3,938 |
| Covishield or Vaxzevria [AstraZeneca or Serum Institute of India] | 23,094,620 | |
| Sputnik Light or Gam-COVID-Vac [Gamaleya Research Institute] | 26 | |
| Sputnik V [Gamaleya Research Institute] | 84,460 | |
| Janssen [Janssen/Johnson & Johnson] | 1,137,505 |
In brief, a total of 183,559,462 doses of BNT162b2, 36,178,442 doses of mRNA-1273, and 23,093,399 doses of ChAdOx1 were administered across participating sites during the study period to a grand total of 99,068,901 vaccinated individuals. As for the study period, I’ll just quote the methods:
The study periods varied across countries, commencing on the date of the site-specific COVID-19 vaccination program rollout, and concluding at the end of data availability (Table 1). In general, the study periods spanned from December 2020 until August 2023. The shortest study period observed occurred in Australia – New South Wales, including 11 months from February 2021 to December 2021. Argentina had the longest study period, from December 2020 to August 2023, encompassing a total of 32 months.
The risk intervals used after each dose were 0–7 days, 8–21 days, 22–42 days, and 0–42 days. For each vaccination dose, day 0 was denoted the day of vaccine receipt. For this manuscript, we present results for the risk interval of 0–42 days only.
I can tell what antivaxxers will say right here, namely that the followup period was way too short. To that, I like to point out yet again that adverse events attributable to vaccination almost always occur shortly after vaccination, as in days to a couple of weeks. But what were these “adverse events of special interest” (AESI)? I’ve discussed the concept before in the context of a “reanalysis” of the original Pfizer randomized controlled clinical trial (RCT) data used to approve its vaccine and how this “reanalysis” was basically an exercise in extended data mining and p-hacking, or, as I like to call it, statistically torturing the data until they confess. In any event SAESIs were defined by the Brighton Collaborative, a group dedicated to vaccine safety and improving the scientific rigor of vaccine science. For purposes of the current study, the SAESIs chosen to be studied included these 13 conditions:
- Myocarditis. This is inflammation of the heart muscle, regardless of cause.
- Pericarditis. This is inflammation of the pericardial sac that surrounds the heart
- Guillain-Barré syndrome. GBS is a rare rapid-onset autoimmune disorder in which the immune system attacks peripheral nerves, resulting in demyelination that causes muscle weakness and paralysis.
- Transverse myelitis. This is inflammation of the spinal cord that can result in paralysis. Before the pandemic, antivaxxers tried to blame Gardasil for a case of transverse myelitis.
- Bell’s palsy. This is idiopathic and almost always temporary paralysis of one side of the face due to loss of function of the facial nerve. This was one condition that was suspected very early on during the vaccination program.
- Acute disseminated encephalomyelitis. This condition that involves inflammation of the brain and spinal cord, usually due to autoimmune disease.
- Convulsions or seizures.
- Cerebral venous sinus thrombosis. These are blood clots that form in the brain’s venous sinuses (that we’ve written about before).
- Splanchnic vein thrombosis, blood clots that form in the splanchnic veins; i.e. the veins that supply the internal organs in the abdomen, such as intestines and liver.
- Pulmonary embolism. These are blood clots that usually originate in the legs and travel to the lungs. Depending on how large they are, they can be life-threatening.
- Thrombosis with thrombocytopenia syndrome. This is a condition in which blood clots form in large blood vessels and use up platelets, resulting in a low platelet count.
- Thrombocytopenia, or low blood platelets.
- Immune thrombocytopenia. This is an autoimmune disorder that leads to low blood platelets because the immune system attacks them.
Again, this subset of conditions was selected on the basis of safety signals in the safety data for COVID-19 from the much larger list published by the Brighton Collaborative. The followup came to 23,168,335 person-years of followup, with comparison made to the expected (background) rates for these conditions, which were obtained by participating sites using pre-COVID-19 vaccination healthcare data stratified by age and sex using data from 2015 to 2019 (2019–2020 for Denmark). A ratio of observed/expected (OE) was then calculated for each AESI.
So, what did the investigators find? I’ll summarize. An elevated observed/expected ratio was observed for the following key AESIs:
- Gillain-Barré syndrome (2.49x elevated OE) following the first dose of the ChAdOx1 vaccine (replication-deficient adenovirus-based vaccine, AstraZeneca). This signal was not observed for the other vaccines.
- Cerebral venous sinus thrombosis (3.23x elevated OE) following the first dose of the ChAdOx1 vaccine (replication-deficient adenovirus-based vaccine, AstraZeneca).
- Acute disseminated encephalomyelitis (3.78x elevated OE) following the first dose of mRNA-1273 vaccine (Moderna).
- Pericarditis (6.9x elevated OE after a third dose of ChAdOx1-based vaccine); 1.7x and 2.6x elevated OE after the first and fourth doses of mRNA-1273 (Moderna). I note that the patter with the Moderna vaccine is rather odd (first and fourth dose, but no elevated risk otherwise), which suggests to me a possible spurious result. See table following this list.
- Myocarditis was associated with the mRNA vaccines at all doses, confirming a lot of earlier findings, but less so with the adenovirus-based vaccines. See table below.
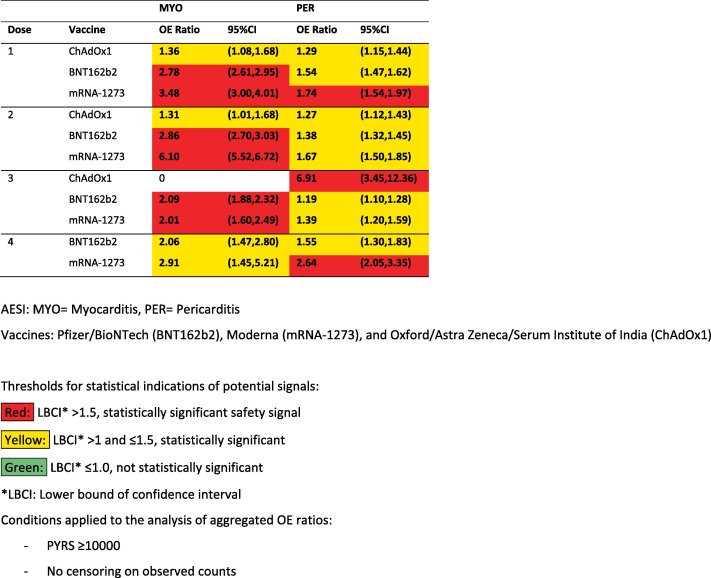
This might sound very scary, and indeed antivaxxers have even made a chart to make it look that way:
Remember, though, that these are relative ratios and say nothing about the actual number of AESIs being examined. If you look at the absolute numbers, the results become a lot less scary. For example, After the first dose of the AstraZeneca vaccine, there was a 3.2x greater-than-expected risk of cerebral venous sinus thrombosis observed in 69 events, compared to an expected 21.That’s out of over 23 million doses of this vaccine. Similarly for Guillain-Barré syndrome, 76 events were expected, but 190 events were observed. That’s out of over 23 million doses of this vaccine. As for acute disseminated encephalomyelitis, seven cases were observed after vaccination with the Pfizer vaccine compared to the two cases that would be expected. That’s out of 183 million doses.
For example, the authors also found a possible safety signal for transverse myelitis and acute disseminated encephalomyelitis, but, again, look at the raw numbers. There were seven cases of acute disseminated encephalomyelitis after vaccination with the Pfizer vaccine (out of nearly 184 million doses), versus the expected number of two. In other words, these adverse events are quite rare. They might be elevated after vaccination but remain rare. I also like to point out that being able to detect single digit numbers of adverse events after 180+ million doses of vaccines rather puts the lie to claims by antivaxxers that we can’t detect rare adverse events.
There is another issue, as well. Remember the comparator: The populations in these countries from 2015 to 2019; i.e., the years immediately prepandemic. The question is whether the denominator (expected/background rate) was affected by the pandemic, and likely it was given this:
Meanwhile, the chances of having a neurological event after a Covid infection were up to 617-fold higher than following COVID vaccination, which suggests “the benefits of vaccination substantially outweigh the risks,” according to the Vaccine study researchers. The risk of developing myocarditis is higher post-Covid infection than after getting a Covid vaccine, according to Akiko Iwasaki, PhD, professor of Immunobiology at Yale University. Myocarditis risk after the second dose of a Covid vaccine is 35.9 per 100,000 people, compared to a 64.9 per 100,000 risk after Covid infection. The risk of developing Guillain-Barre syndrome after Covid infection was six times greater, and the risk of developing it after vaccination was 0.41 times greater than the control group, according to a 2023 study published in Neurology.
Consequently, although the elevated risk of various SAESIs associated with these vaccines appears to be significantly elevated (although still rare) after vaccination with certain COVID-19 vaccines, the elevated risk might be less than the investigators estimated if COVID-19 itself led to elevations in the rates of these conditions above baseline.
Of course, none of these considerations trouble antivaxxers, who immediately seized on the study to portray vaccines as deadly.
Steve Kirsch’s gonna Steve Kirsch: Or, how I learned to stop worrying and love any study that I can spin
You already saw how one antivaxxer on X, the platform formerly known as Twitter, spun the results by leaving out absolute numbers and context. Leave it to everyone’s favorite tech bro turned rabid (and particularly stupid) antivaxxer, Steve Kirsch, to crank the fear mongering up to 11:
A new study of over 99 million vaccinated people has been highly promoted in the press with headlines like “Covid Vaccines Linked To Small Increase In Heart And Brain Disorders, Study Finds—But Risk From Infection Is Far Higher.”
I’m going to convince you that this is bullshit.
Oh, goody. Whenever Mr. Kirsch says something like this, I know that I’m about to be buried in a veritable pile of stinking, drippy diarrheal bullshit. He starts by referring to the chart made by the antivaxxer above and asking:
A safe vaccine would be indistinguishable from a placebo. Does this look safe to you?
See what I said about the Nirvana fallacy? No, Mr. Kirsch. No one in the public health community of scientists and physicians has ever said that a safe vaccine must have an adverse events profile indistinguishable from that due to placebo. That’s your invention, a massive straw man based on the Nirvana fallacy, in which anything less than perfect safety (zero adverse events) and perfect efficacy (100% effective in preventing not just disease but transmission) is viewed as a reason to reject the vaccine. Rather, a safe vaccine is one that is effective and has an acceptable adverse reaction profile in the context of the risk of harm to the population from the disease being vaccinated against.
As predicted, Mr. Kirsch also pulled out the ever-popular antivax appeal to “long term” safety:
They only looked for 42 days after the shots since everyone knows you can’t get adverse events after 42 days (I’m being sarcastic).
Actually, it’s pretty accurate to say that adverse events six or more weeks after vaccination are very, very rare indeed. I’ll just cite this article summarizing the question, as I like to do whenever antivaxxers drop this trope on me. If one wants to quibble, the article does acknowledge some adverse events up to eight weeks after vaccination, but Mr. Kirsch isn’t being that pedantic. For him, any time frame after vaccination chosen for examining adverse events would be too short because he is an antivaxxer and for antivaxxers no time frame is “long term enough” for any vaccine safety study.
Next up:
They didn’t evaluate mortality due to the shot since everyone knows the vaccines are safe and didn’t kill anyone (I’m being sarcastic).
Because, of course, Mr. Kirsch falsely believes that the vaccines have killed millions of people. Here’s the thing, though. First, this study was designed to look at AESIs based on the literature thus far about COVID-19 vaccine safety. If the vaccine were as deadly as Mr. Kirsch deludedly believes it to be, it would have shown up long ago, picked up by the vaccine safety monitoring systems in the US, Europe, Australia, Canada, etc. (Seriously, the level of utter fantasy-based thinking that it takes to believe that tens of millions of deaths would either not be noticed by these systems or would be covered up is truly difficult for science-based people to comprehend.) Here, he’s covering up the flimsiness of his critique with sarcasm.
Next up:
They found clearly increased risk of the various AESI, but the end conclusion is that the risks after COVID infection are far higher, so people should take the shots. This is unbelievable. I don’t know a single cardiologist whose business dropped after the COVID vaccines rolled out. Do you?
Actually, the study itself says almost nothing about the risks of the shots relative to the risks from COVID-19. Seriously. Go read it. I’ll wait. Mr. Kirsch is conflating an interview with Akiko Iwasaki, PhD, professor of Immunobiology at Yale University (which I quoted above) with the actual conclusions of the paper.
Here’s basically all the paper says about the risk-benefit ratio:
The safety signals identified in this study should be evaluated in the context of their rarity, severity, and clinical relevance. Moreover, overall risk–benefit evaluations of vaccination should take the risk associated with infection into account, as multiple studies demonstrated higher risk of developing the events under study, such as GBS, myocarditis, or ADEM, following SARS-CoV-2 infection than vaccination.
In other words, it’s saying that these safety signals should be contextualized in terms of their clinical relevance and the risk of these AESIs relative to the risk from the disease, not the definitive statement straw-manned by Mr. Kirsch. He also throws in an appeal to personal incredulity for good measure. Here’s a hint: Just because you can’t believe something doesn’t mean it’s not true. As for the bit about the cardiologist. That’s an appeal to personal anecdote and utterly meaningless. After all, no one is saying that myocarditis isn’t a risk after certain COVID-19 vaccines, and certainly no one is claiming that cardiologists have lost business since the vaccines rolled out. Yet that doesn’t stop Mr. Kirsch from repeating that same brain-dead line again later in his post.
And, of course, there’s the conspiracy theory in which “They” are “hiding” the “truth” from you:
As usual, they aren’t allowed to share the data so you have to take their word for it.
The reason they aren’t allowed to share the data is that the databases used contain individual-level health records with protected health information (PHI). Given how Mr. Kirsch has received a stolen database from New Zealand with PHI that he’s misused to claim that COVID-19 vaccines have killed 13 million people. He even threatened to release PHI from the stolen database that he has as a means of pressuring the New Zealand government. So, yes. I wouldn’t let Mr. Kirsch anywhere near PHI of any kind either. He’s proven himself to be utterly untrustworthy.
The rest of Mr. Kirsch’s diatribe consists mainly of him cherry picking a single study to claim that COVID-19 vaccines don’t work. (Remember, if there is no benefit to the vaccine, then any risk at all from it is unacceptable, which is why antivaxxers try their damnedest to deny any benefit at all from the vaccines or to argue that the benefit is so minimal as not to be worth even the rare adverse event.) He cites a dubious year-old analysis of the VAERS database from Josh Guetzkow, who has long been trying to portray antivax crankery as “suppressed.”
He then argues that, even if it is true that the risk of various adverse events is higher with COVID-19 than with the vaccine:
But even if that was true (which it isn’t), it doesn’t matter because, as I mentioned earlier, the vaccine doesn’t prevent you from getting COVID, so the vaccine is simply adding to the risk.
Again, Mr. Kirsch bases this assertion on one cherry picked study and then cites his own ridiculous Internet/Substack survey as though it were evidence of anything other than that his audience believes that COVID-19 vaccines cause horrific complications and an antivax propaganda film disguised as a documentary (and promoted by The Epoch Times), The Unseen Crisis. As is typical of such “documentaries,” it largely consists of anecdotes by people who blame COVID-19 vaccines for their various and sundry health problems and complaining that doctors wont’ believe them, interspersed with interviews with antivax quacks like Robert Malone, Peter McCullough, and others attributing all sorts of harms to the vaccines, whether there’s good evidence that those harms were caused by the vaccines or not. Mr. Kirsch notes that he’s in it, too, because of course he is.
He concludes by lying about the New Zealand data:
All my attempts at data transparency have been rejected. The health authorities have determined that you get better public health outcomes if you keep the public in the dark. So all my calls for data transparency fall on deaf ears. The best “ground truth” data we have is from the New Zealand data leak…and it clearly shows that the vaccine increases mortality. The critics acknowledge I’m right, but say that “it must be due to a confounder.” More on that coming up tomorrow.
No, as I’ve discussed, people keep telling Mr. Kirsch he’s wrong because his analysis was risibly incompetent and he could well have a biased sample from the overall database, among other problems. Kirsch is gonna Kirsch though; that is, he’ll never admit error but will instead repeatedly double down when his errors are pointed out.
Heads I win, tails you lose
In the end, this study and how antivaxxers have spun it is an excellent example of “Heads I win, tails you lose.” While the study puts the lie to the ideas that vaccines aren’t studied for safety, that we don’t carefully study potential adverse events from vaccination, and that we can’t detect rare events in vaccine safety studies, like all vaccine safety studies that acknowledge rare adverse events due to vaccination, it provides grist for the antivax propaganda mill. Again, if you assume, as antivaxxers do, that vaccines don’t work, then of course you’re going to conclude that the adverse event profile of any vaccine should be indistinguishable from placebo because if an intervention has no benefit then even one adverse event makes the risk-benefit ratio one divided by zero, or infinity. Similarly, if you don’t believe that the disease is dangerous (as antivaxxers try to portray COVID-19, then no adverse events are acceptable because you don’t need the vaccine. In any event, it is a fantasyland antivaxxers are living in, because no pharmaceutical product that is effective is 100% safe. In the real world we have to weigh risks versus benefits. In antivaccine world, only the risks matter, and no risk, no matter how small, is acceptable.
As I said before, it’s the Nirvana fallacy combined with trying to convince you that vaccines don’t work. No matter how safe a study demonstrates a given vaccine to be, as this study demonstrates the COVID-19 vaccine to be very safe but not perfectly safe, antivaxxers will spin it by emphasizing only the risk side of the equation. They used to do it long before the pandemic, and they do it with a vengeance now.