
{kind=link}
With emergency use approvals (EUAs) having been granted by the FDA to two mRNA vaccines against COVID-19, one manufactured by Pfizer/BioNTech and the other developed by Moderna, with more likely to follow in the coming months, we are on the cusp of what is likely to be the largest mass vaccination program in history. It’s a program that is likely to take many months to achieve even in wealthy “First World” countries, given the logistics of manufacturing, distributing, and administering vaccines, one of which requires an ultracold storage temperature. As vaccines roll out, first to tens of thousands and then to tens of millions, it is inevitable that there will be adverse reactions attributed to them. The question will then become: Did the vaccine cause the adverse reaction? You can bet that the antivaccine movement and the COVID-19 cranks will blame every adverse health event after administration of any of the COVID-19 vaccines that are just starting to find their way into the arms of frontline healthcare workers and the most vulnerable, and I’m worried that we in the science-based medicine community might not be sufficiently prepared for the tsunami of bad epidemiology that is to come.
What led me to think about this was this story:
A volunteer who signed up for Moderna’s coronavirus vaccine trial was struck by lightning 28 days after receiving the injection. That 72 year-old volunteer, whose name and gender have been withheld, met with the freak accident after getting an actual shot of Moderna’s vaccine, rather than the placedo [sic], during the second phase of the vaccine’s trials.
The bizarre incident was revealed in the US Food and Drug Administration’s written media briefing into the safety of Moderna’s new vaccine. Doctors diagnosed the lightning strike victim with arrhythmia – an irregular heart beat – believed to have been caused by the strike. No further updates have been provided on the volunteer’s condition.
The incident comprised one of three Serious Adverse Effects (SAEs) suffered by study participants who received the real vaccine – with all of those health scares deemed unrelated to the shot itself.
This led to a sarcastic comment that I couldn’t resist Tweeting:
Others couldn’t resist, either:
But but but
The microchip attracted that lightning bolt! pic.twitter.com/eJXmmCENlv
— Steve Carroll DO MEd (@embasic) December 16, 2020
A 72yo that SURVIVED getting hit by lightning with just arrhythmia? I think that's a significant result. They should start touting it as PROTECTION from lightning strikes.
— Derek Zarban (@DerekZarban) December 17, 2020
You get the idea.
Obviously, it’s utterly ridiculous to conclude that a vaccine can somehow make its recipient more likely to be the victim of a lighting strike or, to put it in simpler terms, that a vaccine will attract lightning. There’s no plausible scientific mechanism for a vaccine (or even an implanted microchip, if there were one in COVID-19 vaccines) to accomplish this. That’s why I and my fellow advocates of science-based medicine made jokes about it. It’s also why I chose to use this particular example to illustrate that most adverse events (AEs) in large clinical trials of vaccines involving tens of thousands of people are more likely to be coincidence than due to the vaccine. Other examples include people getting hit by cars, which happens in large clinical trials, events that are included in the AEs listed. The key problem in such clinical trials is to differentiate AEs that are likely to be due to the vaccine versus AEs that are not. Of course, antivaxxers either don’t understand this key distinction or willfully ignore it in the service of spreading disinformation, but I can see these sorts of stories doing harm in persuading people to accept COVID-19 vaccines.
What I’m going to do in this post is to look at a couple of AEs being attributed to COVID-19 vaccines and, hopefully, by discussing them, help you understand how to look at them. You know the press will hype them. You know antivaxxers will go wild over them. What I’m hoping to achieve in this post is to provide some of the tools for you to critically examine these claims. I’ll look at two claims and then circle back to review them in the context of determining causality. One occurred during the clinical trials, and one occurred after vaccination after the EUA.
Tiffany Dover and the case of vasovagal syncope
Tiffany Dover is a nurse who was caught on video fainting after having received the COVID-19 vaccine, leading to stories like this, from the ever-sensationalistic New York Post:
This is the scary a moment a nurse who had just received the coronavirus vaccine at a Tennessee hospital told reporters she was feeling dizzy and then fainted.
Nurse manager Tiffany Dover received the Pfizer-BioNTech jab at CHI Memorial Hospital in Chattanooga on Thursday and was giving a press briefing when she began to trail off, according to WTVC-9.
“All of my staff, you know, we are excited to get the vaccine. We are in the COVID unit, so therefore, you know, my team will be getting first chances to get the vaccine,” Dover said.
“And I know that it’s really … Sorry, I’m feeling really dizzy,” she continued.
One of the doctors behind her caught her as she passed out about 17 minutes after receiving the shot.
“It just hit me all of a sudden, I could feel it coming on. I felt a little disoriented, but I feel fine now, and the pain in my arm is gone,” Dover said after recovering.
Doctors said the episode was not related to the ingredients in the vaccine.
And here’s the video:
That story ran on Friday. By Saturday, antivaxxers were claiming that Tiffany Dover was in bad shape (or even dead) and that CHI Memorial Hospital and the CDC were covering it up:
OMFG! FAINTING NURSE DIED
TIFFANY DOVER IS DEAD
I saw that fainting nurse died, so I checked it out!
This death record…Posted by Kitty Lynn on Saturday, December 19, 2020
And:
And, in case you’re wondering:
So what happened? Anyone in primary care, emergency medicine, or involved in any activity in medicine in which patient blood draws, injections, or vaccinations are involved knows that this was almost certainly nothing more than vasovagal syncope, a very common reaction to needlesticks. This phenomenon is not rare. It’s actually far from rare, so much so that the CDC has a webpage that discusses fainting after vaccination, which usually occurs within 15 minutes and can sometimes even happen before vaccination in response to just the sight of the needle. It’s the reason why people receiving vaccinations are usually observed for 15-30 minutes afterward. As the CDC notes:
Fainting can be triggered by many types of medical procedures. In fact, CDC has received reports of people fainting after nearly all vaccines. Fainting after getting a vaccine is most commonly reported after three vaccines given to adolescents: HPV, MCV4, and Tdap. Because the ingredients of these three vaccines are different, yet fainting is seen with all of them, scientists think that fainting is due to the vaccination process and not to the vaccines themselves. However, there is not yet a definite answer about whether an ingredient of the vaccines is responsible for the fainting or if adolescents are simply more likely than children or adults to experience fainting.
The CDC also has studied the issue before, for example, in this study undertaken because of reports of vasovagal syncope after vaccination with HPV vaccines, in which CDC investigators examined reports from the Vaccine Adverse Event Reporting System (VAERS). The CDC found:
A total of 463 reports of postvaccination syncope during January 1, 2005–July 31, 2007 (Figure), were identified among persons aged >5 years, compared with 203 reports during 2002–2004. The rate of reports for postvaccination syncope among persons aged >5 years were as follows: 0.30 reports per million doses distributed in 2002, 0.35 per million doses distributed in 2003, 0.28 per million doses distributed in 2004, 0.31 per million doses distributed in 2005, and 0.54 per million doses distributed in 2006.
Compared with reports received during 2002–2004, those received during 2005–2007 were more likely to involve females (61.1% versus 77.5%) or persons aged 11–18 years (47.3% versus 62.0%) (Table). In 292 (63.1%) of the 463 reports during 2005–2007, syncope was associated with at least one of the following recently approved and recommended adolescent vaccines: MCV4, Tdap, and HPV.
Thirty-three (7.1%) of the 463 postvaccination syncope reports during 2005–2007 were coded as serious (Table); the percentage was not substantially different from the corresponding 20 (9.9%) serious reports during the earlier comparison period. After clinical review, seven of the reports coded as serious were excluded because they were either not compatible with the diagnosis of syncope (n = 4) or did not meet the criteria of seriousness (n = 3); 26 reports of serious adverse events were analyzed further. The 26 patients ranged in age from 11 to 84 years (median: 18 years), and 20 (76.9%) were female. Similar to the findings for syncope reports overall, females aged 11–18 years accounted for the largest number of serious syncope reports (n = 11 [42.3%]). Among the 23 patients for whom times of vaccination and syncope onset were indicated, 12 (52.2%) occurred within 5 minutes of vaccination, and 16 (69.6%) occurred within 15 minutes. Ten of the 26 serious reports indicated that secondary injuries occurred after syncope, including head injuries (n = 9) after syncope-related falls and a motor-vehicle incident (n = 1) because the patient lost consciousness while driving. Seven (70.0%) of the 10 secondary injuries occurred within 15 minutes of vaccination.
Meanwhile, it turns out that the video was deceptively edited, leaving out how rapidly Dover recovered and how she explained right after recovering:
After getting the shot, Dover began to feel lightheaded and then passed out, which was shown in the news clip.
Shortly afterward, she explained to the TV reporter, “I have a history of having an overactive vagal response and, so, with that, if I have pain from anything — hang nail or I stub my toe — I can just pass out.”
Dover reported that she was “feeling fine” after her fainting episode. “The pain in my arm is very minimal, actually, but it doesn’t take much,” she said, estimating that she has fainted “six times in the last six weeks.”
The hospital issued a statement the following day quoting Dr. Jesse Tucker saying, “The fainting episode is not an adverse reaction to the vaccine, but related to her medical condition.”
An “overactive vagal response” basically means that nerves controlling heartbeat and blood pressure send the wrong signal — slowing the heart while expanding blood vessels — and blood pools in the legs, so the brain doesn’t get enough oxygen. This response is often triggered by pain and causes a person to faint.
It’s “quite common,” according to a description from Cedars-Sinai, which explained that the condition “most often affects children and young adults, but it can happen at any age.”
Pediatrician Dr. Vincent Iannelli has discussed the issue of fainting after vaccination in depth. He points out that the most common reports are of teens receiving adolescent vaccines, especially girls receiving Gardasil, but that the “CDC has received reports of people fainting after nearly all vaccine..” What amazes me, in fact, is that, a few days after mass vaccination of healthcare workers and nursing home residents and workers, we haven’t seen a whole lot of reports of syncope after COVID-19 vaccination and a lot of examples of healthcare workers being caught on camera fainting.
Pointing to a common phenomenon that generally doesn’t have anything to do with specific vaccines but the needle and the pain, and using it to demonize vaccines, is an old antivaccine trope. It became a particularly common and favorite technique after Gardasil was approved and so many adolescents started getting vaccinated, as syncope after vaccination appears to be more common in that age group by claiming that HPV vaccines cause postural orthostatic tachycardia syndrome (POTS). Dr. Iannelli has also discussed POTS, quoting the CDC regarding whether HPV vaccination can cause POTS:
POTS is a condition that causes lightheadedness or fainting and a rapid increase in heartbeat upon standing. The cause is unknown, but doctors think POTS may be associated with a number of risk factors and syndromes, including: a recent viral illness, physical deconditioning, chronic fatigue syndrome and nervous system problems.
After citing a number of studies that fail to find evidence of correlation between vaccination and POTS, Dr. Iannelli further notes that the reason there appears to be a correlation between POTS and HPV vaccination that does not indicate causation is probably this:
But why has the focus been on the HPV vaccines?
It is an easy association to notice, after all POTS begins to occur right around when the HPV vaccines are given (teen years) and the HPV vaccines are given in many different countries. Most other vaccines that we give to teens in the United States, including Tdap and the meningococcal vaccines, aren’t as widely used in other countries.
But remember, POTS isn’t a new diagnosis. That anti-vaccine groups are latching onto it to scare parents away from vaccinating and protecting their kids is.
Again, I’m actually pleasantly surprised that there’s only been one high profile example of fainting after COVID-19 vaccination a few days into the vaccine rollout, but I expect to see a lot more of this as the vaccines find their way to more and more people. I also expect to see antivaxxers attempt to link the COVID-19 vaccine to POTS, the way they have with HPV vaccines.
But what about a less obvious example? I started with a ridiculously obvious example of confusing correlation of an AE after COVID-19 vaccination with causation, moved to a more plausible example, and now I’m going to discuss a still more plausible example that might be related to COVID-19 vaccination but, far more likely, is not.
Bell’s palsy and COVID-19 vaccination
Also last week were reports that there was an increased incidence of Bell’s palsy observed in the clinical trials used to gain the EUAs for the Pfizer/BioNTech and Moderna vaccines. Before I delve into these observations, let’s review what Bell’s palsy is. Bell’s palsy, also known as idiopathic facial paralysis is a type of facial paralysis in which the facial nerve on one side ceases to work correctly, resulting in muscle weakness or paralysis on that side of the face. It’s actually a surprisingly common condition, almost always self-limited, and resolves within a few weeks – but it can be, as you might imagine, quite striking and disturbing. Often, the symptoms of Bell’s palsy arise one or two weeks after an infection, such as a cold, ear infection, or eye infection. Symptoms usually appear fairly abruptly and are characterized by a droopy appearance to one side of the face, as you might see after a stroke. Rarely, Bell’s palsy can affect both sides of the face.

This is what Bell’s palsy looks like.
Other symptoms can include:
- drooling
- difficulty eating and drinking
- an inability to make facial expressions, such as smiling or frowning
- facial weakness
- muscle twitches in the face
- dry eye and mouth
- headache
- sensitivity to sound
- irritation of the eye on the involved side
Even though Bell’s palsy is usually self-limited, it is important to distinguish it from other conditions that can cause unilateral facial paralysis, such as a stroke or brain tumor. In any event, the root cause is inflammation and/or compression of the seventh cranial nerve (facial nerve). The exact cause is not known, but in general it’s believed that it’s probably triggered by a viral infection. Some infections that have been associated with Bell’s palsy include:
- herpes simplex, which causes cold sores and genital herpes
- HIV/AIDS
- sarcoidosis, which causes organ inflammation
- herpes zoster virus, which causes chickenpox and shingles
- Epstein-Barr virus, which causes mononucleosis
- Lyme disease
Other risk factors for the condition include pregnancy, diabetes, family history, and lung infections. The treatment is expectant, waiting for the symptoms to resolve, but certain medications can help, including corticosteroids to decrease the inflammation, antiviral medications or antibiotics (if it’s thought that an infection caused the palsy), pain medications, and eye drops to keep the eye on the affected side from drying out because the eyelid can’t be closed all the way. Most affected individuals (75%) will recover within three to six months without treatment.
So now let’s get to the reports:
A 54-page staff report released Tuesday said there were four reported cases of Bell’s palsy among Moderna’s more than 30,000 clinical trial participants. Three of the participants who got Bell’s palsy also received the vaccine instead of a placebo shot. Pfizer’s trial similarly had four reported cases of Bell’s palsy out of some 43,000 participants. All four Bell’s palsy cases in Pfizer’s trial got the vaccine and not the placebo.
And:
Two of the cases of Bell’s palsy among Moderna’s vaccine group have since “resolved” while one was still ongoing at the time of the report, the FDA staff said. The vaccinated participants experienced the paralysis between 22 days and 32 days following inoculation, they said.
Wow! This sounds scary, doesn’t it? Actually, it’s not. How can I say that? Easy. All I have to do is to compare what is observed in the clinical trial with the background incidence of Bell’s palsy in the general population:
In the general population, having nothing to do with Covid-19 nor the Covid-19 vaccine, approximately 40,000 individuals develop Bell’s palsy annually in the United States, or approximately 1 in 10,000. In both groups of vaccine trial participants, the rate (1 in 10,000) was commensurate with the incidence of sudden facial paralysis in the general population.
It should also be noted that the claim that vaccines can cause Bell’s palsy is not new. A couple of years ago, über-quack Dr. Joe Mercola was peddling the myth that vaccines cause Bell’s palsy by citing a study that examined VAERS reports. Dr. Iannelli noted that none of the cases were verified to determine if the Bell’s palsy was real or actually caused by a vaccine. (That is, of course, a general problem with VAERS.) He also noted that there haven’t been any studies that find a convincing link between vaccination and Bell’s palsy other than an inactivated intranasal influenza vaccine that was only used in Switzerland during the 2000-01 flu season, was associated with an increased risk of Bell’s palsy. Other than that, though, there isn’t much of anything.
It’s very, very important when evaluating AEs after vaccination to be aware of the background rate of that particular condition in the general population not receiving the vaccine. In this case, the number of cases observed in the groups receiving the vaccine is actually lower than what we would expect to observe in the general population. What’s actually weird is how few cases were observed in the groups not receiving the vaccine. This indicates that this observed correlation is likely not causative. Obviously, patients need to be followed longer, to see if the incidence over a whole year ends up being worrisome, but at this point it appears unlikely that either the Pfizer/BioNTech or Moderna vaccines cause Bell’s palsy, at least based on the current clinical trials.
This is why the FDA has stated:
Our working hypothesis is this just was an imbalance in background rates like we’ve seen in other trials, but we’ll make sure that we’re going to actually query for that just to bring that question to close
That’s another important point. This observed correlation is not being swept under the rug, contrary to what antivaxxers claim. It’s not being denied. The FDA plans on monitoring the clinical trial recipients for Bell’s palsy and the people receiving the vaccine since the EUA. If there is a real correlation that might indicate causation, it will be found. To that I’d also add that, even if there is a real correlation, a one in ten thousand chance of what is almost always a self-limited condition is a small risk to take for protection against COVID-19, particularly among those who are more susceptible to severe diseases, such as the elderly and those with chronic health conditions.
Vaccines and autism
Let me bring home my message by briefly revisiting the most famous “AE” of all that is attributed to vaccines, autism. As regular readers know, there are many robust, well-designed studies involving a hundreds of thousands, if not millions, of children all over the world carried out using different methodologies that have utterly failed to find even a whiff of a hint of a signal indicating an association between vaccination and autism risk. None of this has ever stopped antivaxxers from invoking the ever-present anecdotes of parents who say their children showed the first signs of autism after vaccination. This is not good evidence. As has been pointed out to antivaxers many times over the years, a number of vaccines are administered during age range when autism symptoms first manifest themselves; so, given the millions of children vaccinated every year, by random chance alone a number of children will manifest their first symptoms of autism in fairly close temporal proximity to vaccination. There’s a lovely graphic over at The Logic of Science that shows a back-of-the-envelope calculation of how many children we would expect to exhibit symptoms of autism after vaccination by random chance alone, noting:

Also noted:
Additionally, we would actually expect the odds of a parent noticing the symptoms of autism to skyrocket shortly after a vaccine is administered. Many parents are very concerned about a vaccine harming their child, and, as a result, they will tend to watch their children very closely after vaccinating them (even if they don’t consciously realize that they are doing so). Thus, they are far more likely to notice an early sign of autism that they might have missed if they hadn’t been watching their children so closely. To give an analogy, after people buy a new car, they often start seeing that model and paint job everywhere, but that model isn’t actually any more abundant than it was before, it’s just that their brains notice it because they are thinking about it (consciously or subconsciously). Even so, you are far more likely to notice an early sign of autism if you are worried about it. So in actuality, my numbers are likely underestimates rather than overestimates.
Indeed. There is a lot of confirmation bias in these anecdotes as well, in which parents remember information that supports their current belief that vaccines caused their child’s autism and forget disconfirming information, particularly subtler symptoms that they might have noticed (or missed) before vaccination that are apparent on videos taken of the child before vaccination. This is human nature. We all do it unconsciously; the only difference between skeptics and everyone else is that we try to compensate for it. Truth be told, we don’t always succeed, because it takes effort to be aware when we’re falling prey to this particular human cognitive issue. That’s why the correct question is not whether there is an association between vaccination and autism, but rather whether there is an association between vaccination and autism that is greater than could be explained by random chance alone. The question has been studied time and time again and shows that there isn’t.
Still, human beings are pattern-seeking animals. This pattern-seeking behavior is not well-suited to a task like evaluating drug safety. Many of us will conclude, after taking a drug or receiving a vaccine, that anything bad that happens soon afterward was likely caused by the drug or the vaccine, even when it is far more likely that it was random chance (i.e., coincidence), and nothing more. Such is the case with vaccines and autism. The ages during which children receive a lot of vaccines just happens to correspond to the ages where parents most frequently first start noticing the signs of autism spectrum disorders. In the case of the rollout of the COVID-19 vaccines, this pattern-seeking behavior will lead many people, particularly those predisposed to believe that COVID-19 is no big deal or that vaccines are harmful and ineffective, to blame all manner of AEs that occur after vaccination on the COVID-19 vaccine. It’s true that some of those AEs might actually have been caused by the vaccine, but most of them will not have been. It will take careful study to figure out which AE falls into which category.
In the meantime, whenever you see breathless media reports of some horrific AE after COVID-19 vaccination or antivaxxers blaming the COVID-19 vaccine for this or that health problem, remember all these considerations and remain calm. Most of these AEs will not pan out as having been caused by the vaccine, but, frustratingly, it will likely require time for the FDA and public health authorities to work out which one is which.
My experience with side effects of the COVID-19 vaccine

Dr. Gorski was just fine after receiving the COVID-19 vaccination.
Those who follow me on Twitter might be aware that I was fortunate enough to get my first dose of the Pfizer/BioNTech vaccine on Friday afternoon. It went just fine, but I won’t lie. In my case, the vaccine did cause some side effects, although none of them were unexpected or dangerous. First, the vaccine made my shoulder more sore than most (but not all) vaccines I’ve had in the past. The only ones that were as bad were flu vaccines a couple of years in the past and the second dose of the Shingrix vaccine. Second, I experienced a fair amount of muscle aches on Saturday, but timely slugs of ibuprofen provided great relief. Finally, on Saturday afternoon and Sunday, I felt tired and a bit lethargic. Immediately after my stationary bike ride Saturday afternoon, I went upstairs to take a shower and afterward found myself horizontal on my bed. No, I didn’t pass out. I just felt tired and thought I’d lay down for a few minutes. That few minutes turned into a three and a half hour unplanned nap. I also had trouble sleeping Saturday night. By Sunday afternoon, however, I felt fine. Unfortunately, what this meant was that I didn’t accomplish nearly as much work over the weekend as I had planned to do.
Which brings me to what antivaxxers are doing now:
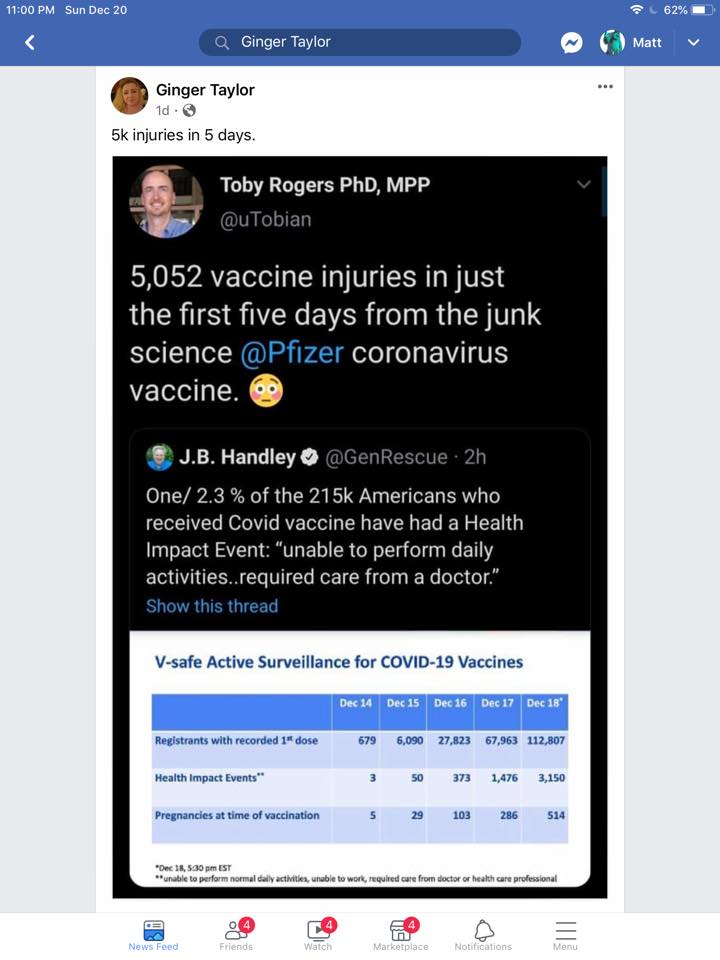
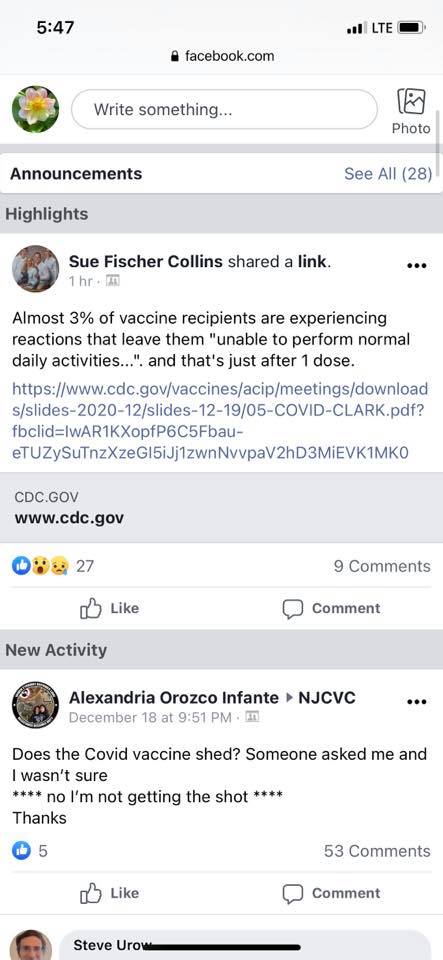
Yes, I suppose that by antivax standards, I had such a reaction to the COVID-19 vaccine. Similarly, since right now it’s mainly healthcare workers who are being vaccinated, a reaction that prevents them from working could be as mild as a fever. Since the pandemic began, healthcare facilities have been screening visitors and workers for symptoms and do temperature checks. If workers have a fever, they are not allowed to work. Basically, antivaxxers are portraying reactions like mine (and milder) as some sort of horrible “vaccine injury” when in fact they are common reactions after effective vaccines. In fact, they’re evidence that the vaccine is doing what it’s supposed to do, provoking an immune response.
Finally, I relate this experience not to frighten anyone out of getting the vaccine but to agree with those reminding people that vaccines, given that their purpose is to result in an immune response, can have effects like this. That is why some healthcare systems have staggered their COVID-19 vaccinations, so that there aren’t too many workers who can’t come to work the next day or two after vaccination. I’ve also heard from colleagues who had similar reactions, which are not really much different or more severe than many vaccines, but I’ve also hear from colleagues who’ve had little or no reaction. Personally, I view my reaction as evidence that the vaccine is working, and it’s good that I plan to have my second dose on a Friday too.
The point is that there will be all sorts of scary stories about COVID-19 vaccines in the coming weeks and months, and a lot of people will have reactions similar to mine. Again, most symptoms other than the sort that I experienced will turn out not to be due to the vaccine, and the benefits of getting vaccinated against COVID-19 far outweigh the very small risk, particularly in a pandemic. Don’t let antivaxxers and COVID-19 cranks frighten you to believe otherwise.
And remember, mRNA-based COVID-19 vaccines will most definitely not permanently alter your DNA.