{kind=link}
![]()
October is National Chiropractic Health Month (NCHM) and chiropractors can’t resist the opportunity to overstate, obfuscate, and prevaricate in celebration.
They do this in the face of some unfortunate (for them) statistics revealed by a recent Gallup Poll. The Poll was paid for by Palmer College of Chiropractic as part of an effort to increase the chiropractic share of the health care pie. (There is also a secondary analysis of the poll in the Journal of Manipulative and Physiological Therapeutics.) We’ll get to those stats in a few minutes.
But first, in celebration of NCHM, the American Chiropractic Association (ACA) has produced a set of six graphics chiropractors can download and display. Four of them fudge on the facts. Let’s take a look at these graphics, compare them to the evidence cited in support of their claims, and see where the ACA went astray. (The ACA also hosted a twitter chat yesterday with the hashtag #PainFreeNation.)
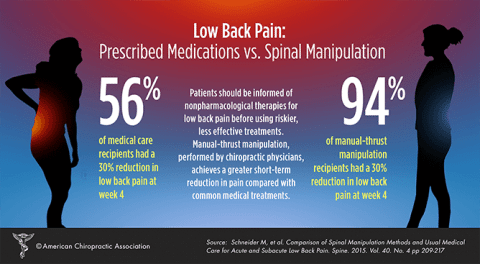
The study cited as evidence for this graphic actually compared both manual thrust manipulation (MTM) and mechanical-assisted manipulation (MAM) to each other as well as manipulation versus usual medical care (UMC). Although MAM, such as the Activator Method, is the second most common manipulation technique used by American chiropractors, is increasing in popularity among them, and is touted to be a safe and effective alternative to MTM, this study found that MTM is more effective (at 4 weeks) than MAM and that MAM had no advantage over UMC. But you don’t see that in this graphic.
The study did not look at “Prescribed Medications vs. Spinal Manipulation” at all. UMC consisted of this:
participants were told that most new episodes of back pain are typically self-limiting, were prescribed over-the-counter analgesic and nonsteroidal anti-inflammatory drugs medications [sic], given advice to stay physically active and avoid prolonged bed rest.
Other limitations not revealed in the graphic, but discussed in the study:
- no placebo control,
- participants were unblinded as to treatment,
- the differences among the groups at 4 weeks were not significant at 3 and 6 months,
- modest size of study, and
- 3 UMC visits versus 8 for the chiropractic treatments.
Also not mentioned was conflicting evidence from other studies, including a 2013 Cochrane Review Update, which concluded that SMT (spinal manipulative therapy):
is no more effective for acute low back pain than inert interventions, sham SMT or as adjunct therapy. SMT also seems to be no better than other recommended therapies.
Most importantly, given that most acute back pain will get better on its own, the authors said:
We could not determine what portion of the healing response was attributable to natural history, direct treatment effect, and/or nonspecific factors, because there was no natural-history control.
Plus, there was this gem from the study’s authors: “Segmental levels where the manipulation was applied was determined by using palpation and the Activator method of leg length analysis,” a totally bogus diagnostic method. And here we’ve been promised that NCCIH, which funded the study, wasn’t going to do this sort of thing anymore. By the way, how did this nonsense slip pass the University of Pittsburg Institutional Review Board?
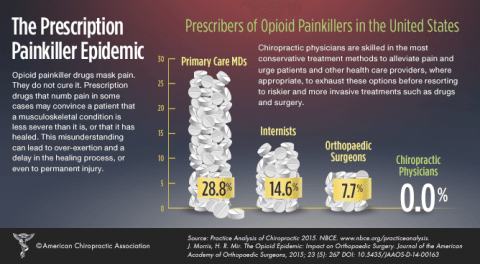
This is yet another attempt by “CAM” practitioners to exploit current concerns regarding overprescribing of opioid painkillers to shill for their own practices. It is ironic that the red flags of over-prescription were raised by, and are being addressed by, the medical community, in an honest attempt to face up to the problem and find solutions. You will find almost no comparable public discussion of the many deficiencies of chiropractic practices by chiropractors.
This sensationalistic graphic is meaningless in the context of chiropractic practice. It is entirely correct that chiropractors don’t prescribe opioids, because their practice acts don’t allow it, the reason being that they lack the proper education and training. The ACA didn’t even get the citation right. The statistics are from Volkow NC, et al., “Characteristics of opioid prescriptions in 2009.” JAMA. 2011; 305(13): 1299-1301. These are simply raw statistics that do not account for why the prescriptions were written or whether prescribing was appropriate.

I’m afraid not. The study cited by the ACA as evidence did not say anything about cost effectiveness. Funded by the ACA (so they, of all people, should know the results), it analyzed the experience of one Tennessee-based general health insurer and found that its claimants “had lower overall episode costs for treatment of low back pain if they initiated care with a DC, when compared to those who initiated care with an MD.”
As Scott Gavura said, don’t call CAM cost effective unless it is actually effective. And as Harriet Hall pointed out, you can reduce costs to zero by eliminating care altogether, which we can all agree is not a good solution.

Once again, the ACA can’t even get the title of its graphic right. They would have you believe that all of these are treatments are for “neck pain.” In fact, none of them are exclusively for neck pain. Spine surgery includes all spine surgery. Cervical spine surgery includes surgery for such things as scoliosis and fractures. NSAID/aspirin use comprises many uses, including those not according to directions. This is likely true of opioid use as well, although we are not provided with the actual content of the e-mail on which they rely for this figure. (And, I would imagine, includes criminal use.) Even cervical manipulation isn’t always for neck pain. Chiropractors “adjust” the neck if the putative “subluxation” is found there, no matter what the patient’s complaint.
But wait, that’s not all:
- No risk-benefit analysis. No matter how small the risk, no treatment is worth it if it confers no benefit. For example, there is no benefit from neck manipulation for “maintenance treatment.”
- No information on pre-existing conditions that may complicate treatment. It may well be that the 80-year-old with cardiovascular disease had a surgical complication. How do you compare that to the healthy 20-year-old who suffered a stroke following chiropractic neck manipulation?
- Lack of uniformity in outcomes. Why are all serious side effects from cervical spine surgery counted but all not serious side effects of cervical manipulation?
This is simply a grab bag of statistics thrown together to tamp down any legitimate criticism of the risks of neck manipulation, which is, in any event, not accurately reflected in this chart. The study cited used chiropractic malpractice claims, which are not indicative of actual risk. Other studies report a range of one in 400,000 to one in 5.8 million manipulations
Of course when you are facing:
- The American Heart Association and the American Stroke Association (with approval by the American Academy of Neurology), stating: “practitioners should both strongly consider the possibility of CD [cervical dissection] and inform patients of the statistical association between CD and CMT [cervical manipulative therapy], prior to performing manipulation of the cervical spine.”
- A lack of evidence that cervical manipulation is beneficial even for a plausible use, that is, neck pain.
- A recent, and unflattering, analysis of the Cassidy study: “Prior studies grossly misclassified cases of cervical dissection and mistakenly dismissed a causal association with manipulation. Our study indicates that the OR [Odds Ratio] for spinal manipulation exposure in cervical artery dissection is higher than previously reported.”
- A Gallup poll showing that almost 25% of the public thinks chiropractic is dangerous.
you simply do what you have to do.
The deficiencies in the ACA’s celebratory graphics I found are based on a layman’s interpretation of the evidence. A more sophisticated analysis might well discover more problems. (And you are welcome to point them out.) The ACA fully realizes that few people will actually look behind their claims and even fewer would be able to decipher the evidence they cite.
Galluping right along
As promised, back to that Gallup Poll, which, as noted, is decidedly a mixed bag for chiropractors. In spite of this, the ACA, the International Chiropractors Association (ICA), and Palmer Chiropractic College are soldiering on, trying to spin the poll to achieve a positive result. I’m not so sanguine.
Undoubtedly, the most distressing among the stats was the revelation that an MD is the first choice of 54% of American adults when choosing a health care provider for back or neck pain, versus only 29% who would choose a chiropractor. In fact, of all health care providers listed, 69% would not choose a chiropractor first. (This question was predicated on the assumption that the cost was about the same.) When your bread and butter is back and neck pain, this is not particularly good news.
Nevertheless, Palmer Chiropractic College made the most of it with this graphic:

Wait a minute. Where’d the 57% come from? This was determined by asking those surveyed about their choices six ways from Sunday. Of those whose first choice was a medical doctor, physical therapist, massage therapist, acupuncturist or other provider, 58% said they would see a chiropractor only if all other treatment methods didn’t work. However, somehow they picked out a group of “expected users” and “likely users” by rejiggering the numbers and reached the conclusion that 57% were actually “likely to see” a chiropractor for neck or back pain, even though this number includes those whose first choice was not a chiropractor. Go figure.
Perhaps to boost these disappointing numbers, Palmer also includes the misleadingly named “neck treatment” comparison available from the ACA.
To be fair, there is another graphic with the all stats comparing health care providers, but, of course, no one has to show that one if they don’t want to.
{kind=link}
61.4% of those surveyed agreed that chiropractic was effective in treating back or neck pain. Again, considering that back and neck pain is the chiropractor’s bread and butter, it would be cold comfort to learn that almost 40% of adults did not think you were effective at your job. There was a similar result on the question of trustworthiness. A little over half of respondents agreed that chiropractors were trustworthy, which means a little under one-half don’t think they can be trusted.
This did not dampen the ICA’s enthusiasm for the poll’s results. The ICA announced, in an email, that “nearly 70 percent of the study participants indicat[ed] that chiropractic care is effective with neck and back pain.” When I took math, if we were measuring in 10s, 61.4% would be rounded down to 60%, not up to 70%, which appears to be what happened. And a poll is not a “study,” nor can it determine the effectiveness of a treatment. Undeterred by such subtleties, the ICA’s headline for this announcement claimed:
Gallup study highlights chiropractic effectiveness and popularity with neck/back pain.
70% of those surveyed believe they know what chiropractors do. Which is interesting because chiropractors themselves can’t agree what it is they do. Some chiropractors think they are primary care physicians and should be able to prescribe drugs. Others think they are spine care specialists who treat musculoskeletal problems. Still others hold on to the notion that phantasmagoric blockages in “nerve energy” running through the spine (the illusory “vertebral subluxation“) can affect bodily function and that chiropractic “adjustments” are effective for all manner of ills.
So what is it that everyone else thinks chiropractors do, even if they don’t know themselves? Of the 12% of respondents who have actually seen a chiropractor in the last 5 years (“chiropractic users”), 41% want to see a chiropractors only for back and neck pain, while the same percentage disagree that they would see their chiropractor for these health issues only, although we are not told just what other problems they would see a DC for.
60% of chiropractic users want to see a chiropractor only if they are in pain, but 31% want to see a chiropractor on a regular basis, even if not in pain. (Again, this is 31% of the 12% who have actually seen a chiropractor within the last 5 years.) I would bet that many of these have been lured into regular treatments for “maintenance care,” based on the totally unproven and highly implausible idea that regular spinal “adjustments” are necessary to maintain one’s health.
There’s bad news here for the “DC as PCP” proponents: of chiropractic users, only 9% would choose their chiropractor as the first healthcare provider they want to talk to about their health. (You can find the entire SBM series on the “DC as PCP” here.) Even then, “talk about their health,” which is the way the question was phrased, is pretty general. I have to imagine a much different result if you started naming specific health issues normally treated by PCPs, such as cardiovascular disease or diabetes. Or even the question: “Do you regard your chiropractor as your PCP?” More users (22%) would talk to their chiropractors about general wellness issues, such as diet and nutrition, but almost 60% of users would not.
They can’t blame the MDs for the bad news. Only 13% of respondents said they had been discouraged from going to a chiropractor by an MD, although that figure rose to 21% for the chiropractic users.
Finally, nearly half of all respondents think chiropractors need only 4-6 years of education beyond high school to become a chiropractor. Palmer is all over this one with another graphic. Obviously, the implication here is that the “degree requirements” for a D.C. degree are about equal to that of an M.D. or D.O. degree. I have no idea if these figures are even correct because I couldn’t find them anywhere in the source listed.

Using this same measure of comparison, I can make the argument that high school is more than equal to college:
High school: 3,600-4,000 “educational hours”
College: 2,160-2,700 (also here) “educational hours”
See how easy it is?
Conclusion: Lies, damned lies, and statistics
Figures often beguile me, particularly when I have the arranging of them myself; in which case the remark attributed to Disraeli would often apply with justice and force: ‘There are three kinds of lies: lies, damned lies, and statistics.’
Mark Twain, Chapters from My Autobiography
{kind=link}