
{kind=link}
Last week, I wrote about an experimental treatment for COVID-19 that repurposes old drugs. One version of the treatment uses chloroquine (which is sold under the trade name Aralen and others), an anti-malaria drug that’s also used to treat autoimmune diseases. Another version, the one that at the time was getting the most press, claimed that the combination of hydroxychloroquine (trade name Plaquenil, and it’s a drug which is very similar to chloroquine) and the antibiotic azithromycin (often prescribed in the famous “Z-Pak”) could completely render SARS-CoV-2, the virus that causes COVID-19, undetectable in patients. As I described, it was a horrible, horrible study about which I later found out things that make me suspect that its awfulness could have been due to more than mere incompetence and instead might have been scientific fraud. Meanwhile, the only existing randomized trial of chloroquine in COVID-19 was negative. As I said at the time, that doesn’t mean that the drug doesn’t work, but it does strongly suggest that its effects are probably not dramatic, although it is also possible that the dose used was too low.
Professor Didier Raoult releases another COVID-19 study
With that background in mind, as I was thinking about what to write this week, I wasn’t planning on writing about this particular issue again, but then I observed two developments. First, Professor Didier Raoult, who published the hydroxychloroquine/azithromycin study, published another trial that’s being flogged as evidence that his combination works. Second, in the conspiracy fever swamps on social media and even on traditional media an emerging narrative was being promoted late last week. It came in the form of articles like this one by a local Pacific Legal Foundation member named Kathy Hoekstra, “Michigan’s doctors fight coronavirus, and governor’s office“. First, let’s discuss the new study of azithromycin and hydroxychloroquine, because I know that’s what will likely most interest people. Again, it’s from Raoult’s group and is entitled “Clinical and microbiological effect of a combination of hydroxychloroquine and azithromycin in 80 COVID-19 patients with at least a six-day follow up: an observational study“.
Unsurprisingly, the first thing I noticed about the study is that it is a single arm, unrandomized trial with no control group. Right there that tells you it’s not going to produce good evidence for the efficacy of azithromycin and hydroxychloroquine against COVID-19. Before I dive into the weeds, let’s just say that I like this description of the trial:
@schneiderleonid @MicrobiomDigest https://t.co/l62Wm7WIYH
Have fun. This paper is so empty that it looks like a cohort description… Without any control group.
— Mathieu M.J.E. Rebeaud, ½PhD #StayTheFuckHome (@Damkyan_Omega) March 27, 2020
In the introduction to the paper, Raoult touts his previous study:
In a preliminary clinical trial on a small cohort of COVID-19 patients, we demonstrated that those treated with hydroxychloroquine (600 mg per day, N=20 patients) had a significant reduction in viral carriage at D6-post inclusion, with 70% of patients testing negative for the virus through nasopharyngeal PCR, compared to untreated controls (N=16) with only 12.5% patients testing negative using PCR at D6-post inclusion (16). In addition, of the twenty patients who were treated with hydroxychloroquine, six received azithromycin for five days (for the purposes of preventing bacterial super-infection) and all (100%) were virologically cured at D6-post inclusion, compared to 57.1% of the remaining 14 patients (16). By contrast, a Chinese study conducted in 30 COVID-19 patients showed no significant differences between patients treated with 400 mg per day during five days (N=15) and controls (N=15) regarding pharyngeal carriage of viral RNA at day7, however, patients received multiple additional treatments including antivirals (17).
As I discussed before (as did others), this study showed nothing of the sort, given the missing PCR data, the inconsistent methodology for reporting PCR data, the lack of an “intention to treat” analysis, the exclusion of six patients in the experimental group who got sicker, and more. It was a terrible, terrible study, but Didier Raoult touted it as evidence that his drug combination could potentially “cure” severe COVID-19 infection.
So what about this new paper? The experimental design is…odd. Basically, Raoult studied 80 patients with PCR-documented SARS-CoV-2 RNA from a nasopharyngeal swab who were admitted to the infectious diseases ward at the University Hospital Institute Méditerranée Infection in Marseille, France. Here, the patient cohort is described:
Upon admission, patients were grouped into two categories: i) those with an upper respiratory tract infection (URTI) presenting with rhinitis and/or pharyngitis, and/or isolated low-grade fever and myalgia, and ii) those with lower respiratory tract infections (LRTI) presenting with symptoms of pneumonia or bronchitis. The time between the onset of symptoms and admission, and the time between the onset of symptoms and treatment was documented.
Risk factors for severe COVID-19, including older age, cancer, cardiovascular disease, hypertension, and diabetes (4), as well as chronic obstructive pulmonary disease, obesity and any immunosuppressive treatments were documented. The national early warning score (NEWS) for COVID-19 patients, was collected upon ward admission and during follow up. The NEWS score was calculated based on the following parameters: age, respiratory rate, oxygen saturation, temperature, systolic blood pressure, pulse rate and level of consciousness (19). We defined three risk categories for clinical deterioration: low score (NEWS 0-4), medium score (NEWS 5-6), and high score (NEWS≥7) for COVID patients.
The need for oxygen therapy, transfer to the intensive care unit (ICU), death, and length of stay in the ID ward were documented.
Again, it was maddening to read the methods section describing how the virus was assayed. Like the case in the previous paper, the methods were not well described. For instance, at one point the authors state that cultures “were attempted in a random selection of patients” without describing how “random” patients were chosen for an attempt to culture the virus from their nasopharyngeal swab. Be that as it may, here are the patient characteristics:
A total of 80 patients with confirmed COVID-19 were hospitalised at the Méditerranée Infection University Hospital Institute (N=77) and at a temporary COVID-19 unit (N=3) with dates of entry from 3–21 March 2020. All patients who received treatment with hydroxychloroquine and azithromycin (16) for at least three days and who were followed-up for at least six days were included in this analysis. The median age of patients was 52 years (ranging from 18 to 88 years) with a M/F sex ratio of 1.1. 57.5% of these patients had at least one chronic condition known to be a risk factor for the severe form of COVID-19 with hypertension, diabetes and chronic respiratory disease being the most frequent. The time between the onset of symptoms and hospitalisation was on average five days, with the longest time being 17 days. 53.8% of patients presented with LRTI symptoms and 41.2% with URTI symptoms. Only 15% of patients were febrile. Four patients were asymptomatic carriers. The majority of patients had a low NEWS score (92%) and 53.8% of patients had LDCT compatible with pneumonia. The mean PCR Ct value was 23.4.
I was scratching my head as I read this. By this description, these patients mostly had mild disease. Only 15% had fever? Fever is a prominent feature of symptomatic adults with COVID-19. Only 53% had lower respiratory tract infection symptoms? Four of the patients (5%) were asymptomatic? 92% had low COVID-19 severity scores as measured by the National Early Warning Score (NEWS)? Why were they even admitted in the first place, rather than instructed to isolate themselves in their homes? That’s what’s generally done; asymptomatic SARS-CoV-2-positive patients and patients with mild COVID-19 symptoms are generally just told to stay home for at least two weeks and call if their symptoms worsen. Later in the paper, we learn that only 15% of these patients required oxygen, while only three required ICU admission, with one death.

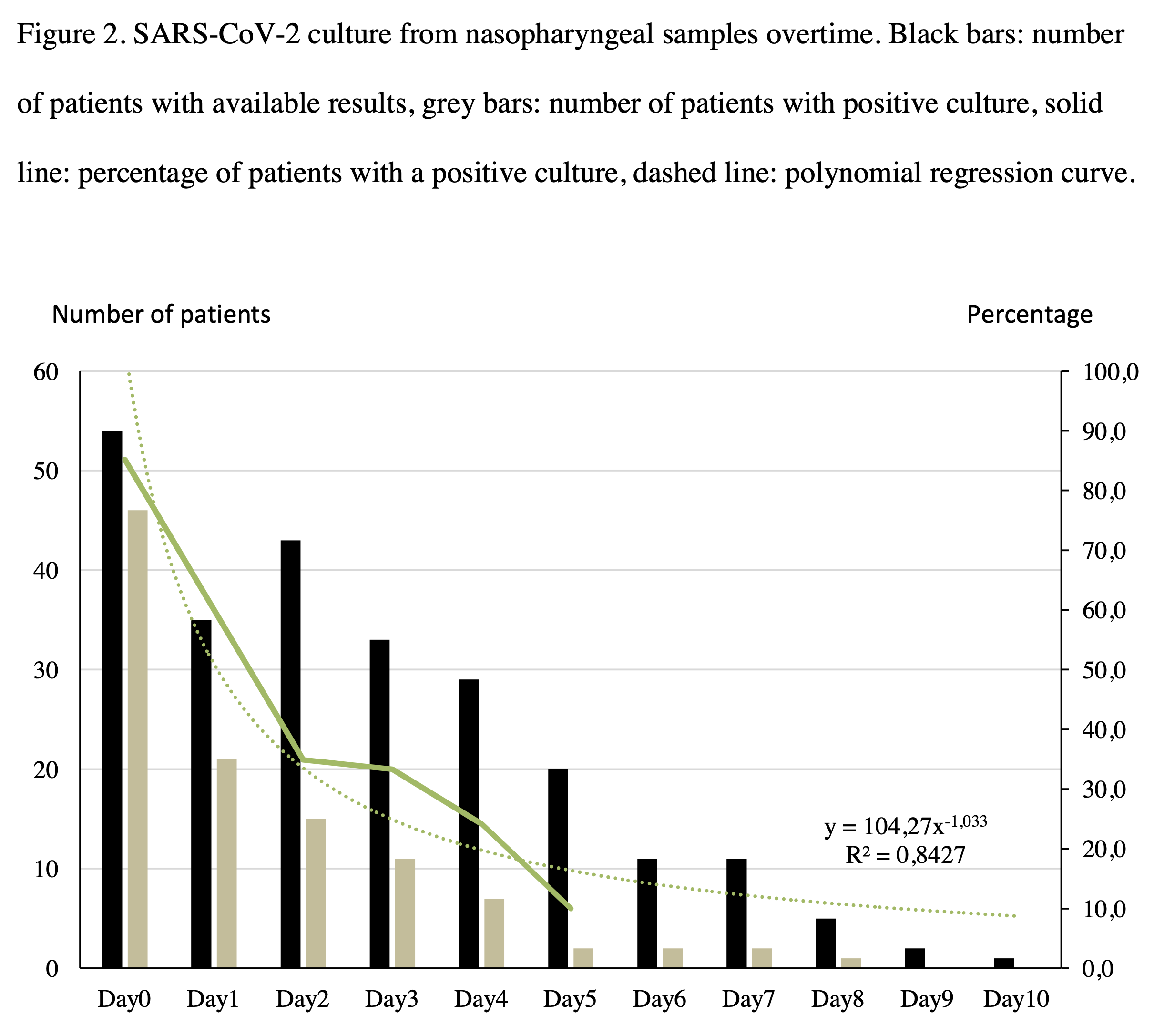
This is a curious way to present the data. First, there is a totally pointless use of a polynomial regression analysis, given that if you use enough variables you can fit almost any curve to an equation. Let’s just put it this way; those R2 values are pretty much meaningless, as are the equations to which these curves were fitted. Why is the equation a quadratic equation for Figure 1 and an exponential equation for Figure 2? Who knows? It sure does produce some nice R2 values, though.
Basically, this is a nothingburger of a paper. It studied patients with low severity or even asymptomatic COVID-19 disease, the vast majority of whom would likely have cleared the virus just as fast without the medications. Again, this is such a useless paper, even as an observational paper, that it tells us, in essence, nothing new.
Meanwhile, Raoult was on Twitter yesterday bragging about “curing” COVID-19:
1003 patients traités à l'@ihu_marseille avec le protocole hydroxychloroquine-azithromycine.
Notre priorité est de guérir les patients diagnostiqués positifs au COVID-19.
Merci aux équipes de diagnostic et de soin qui se mobilisent jour et nuit.#SFMPhttps://t.co/V6HiXiuHUM pic.twitter.com/ohKeHctkYr— Didier Raoult (@raoult_didier) March 29, 2020
Translation: “1003 patients treated with @ihu_marseille with the hydroxychloroquine-azithromycin protocol. Our priority is to cure patients diagnosed with COVID-19. Thank you to the diagnostic and care teams who are mobilized day and night.”
I did like this response:
Donc d'apres les statistiques : 80% de formes bénignes donc 800 traitements pour rien + 20 % de patients traités avec un médicament sans aucune preuve soit 200 environs que vous avez exposés a un risque. Donc 100% d'inutilité et de piétinement de la médecine. Bravo ! #Covid_19
— L'interne des temps modernes (@InterneDTM) March 29, 2020
Translation: “So according to the statistics: 80% benign forms, therefore 800 treatments for nothing + 20% of patients treated with a drug without any evidence, or around 200 that you exposed to a risk. So 100% uselessness and trampling medicine. Well done! #Covid_19”
A new narrative about chloroquine, hydroxychloroquine, and azithromycin
Let’s circle back now in light of yet another uninformative trial on COVID-19 from Prof. Raoult. To understand Hoekstra’s attack against the State of Michigan, you first have to know that late last week Michigan’s Department of Licensing and Regulatory Affairs issued a warning letter about physicians prescribing hydroxychloroquine and chloroquine to family members with the intent to stockpile, thus creating shortages. The letter, signed by Deb Gagliardi, Director of the Bureau of Professional Licensing, and Forrest Pasanski, Director of the Enforcement Division, warned:
Prescribing hydroxychloroquine or chloroquine without further proof of efficacy for treating COVID-19 or with the intent to stockpile the drug may create a shortage for patients with lupus, rheumatoid arthritis, or other ailments for which chloroquine and hydroxychloroquine are proven treatments. Reports of this conduct will be evaluated and may be further investigated for administrative action. Prescribing any kind of prescription must also be associated with medical documentation showing proof of the medical necessity and medical condition for which the patient is being treated. Again, these are drugs that have not been proven scientifically or medically to treat COVID-19.
The letter further reminded pharmacists that they should not fill prescriptions if the pharmacist “believes the prescription will be used for other than legitimate medical purposes or if the prescription could cause harm to a patient” and reminded health care workers that they are “required to report inappropriate prescribing practices.” It was, of course, a reasonable thing to do in order to try to stop some very unethical prescribing that was causing shortages and making it difficult or impossible for lupus patients, for example, to obtain their chloroquine. A followup letter on Friday cited a joint statement by the Michigan State Medical Society and the Michigan Pharmacists Association and a second joint statement by American Medical Association, American Pharmacists Association, and American Society of Health-System Pharmacists.
Unsurprisingly, to Hoekstra, who cited the azithromycin/hydroxychloroquine study that I discussed last week as evidence that these drugs provide great hope, this action was an unconscionable affront to physician autonomy in prescribing off-label medications and saying that ” if you live in Michigan, and you or a loved one is infected with this potentially lethal disease, you’re out of luck.” She also noted that Henry Ford Hospital and the University of Michigan have protocols that include these drugs, further noting:
With his state now the nation’s pandemic epicenter, and with the blessing and help of the president and FDA, New York Gov. Andrew Cuomo brought in 70,000 doses of hydroxychloroquine, 10,000 doses of Zithromax and 750,000 doses of chloroquine.
The implications of Whitmer and her administration’s knee-jerk scare tactics should terrify all Michigan residents. Not only is our state’s top leader threatening the selfless health care workers who are on the frontline trying to save lives, but she’s denying possible life-saving medications to actual COVID-19 victims.
It was a profoundly dishonest article, given that there really is no good evidence that these drugs impact the course of COVID-19 and, worse, they are not benign drugs. the chloroquine drugs can cause dangerous cardiac arrhythmias. It’s an uncommon side effect, but common enough that most protocols using these drugs against COVID-19 require the patient to be on a cardiac monitor. Moreover, the therapeutic window (the difference between the lowest therapeutic dose and a toxic dose) of the chloroquine derivatives is narrow. In any event, you get the idea. It’s a conspiracy theory fueled by those promoting the drugs as miracle cures for COVID-19 that states that there is a cure for COVID-19 that “they” don’t want you to know about. In that, it’s now different than a lot of cancer cure conspiracy theories.
Anecdotes and miracle cures
So what’s driving the narrative about the chloroquine drugs? It certainly isn’t sound clinical trial evidence and science, at least not yet. No one would be happier than I to see some combination of hydroxychloroquine, chloroquine, and/or azithromycin to be validated as effective against COVID-19 in a clinical trial or, even better, validated as prophylaxis against the disease. We’re just not there yet, unfortunately, although there are multiple clinical trials looking at the question now. Until those trials are completed, what’s really driving the narrative are “miracle cure claims,” like this one Tweeted out by President Trump a week ago:
A great early result from a drug that will start tomorrow in New York and other places! #COVIDー19 https://t.co/4F4Qk4WFtK
— Donald J. Trump (@realDonaldTrump) March 23, 2020
The story is about a man named Rio Giardinieri, a 52-year-old who developed severe COVID-19 disease. He’s been showing up all over the media telling this story of how a single dose of chloroquine saved his life:
After more than a week, doctors told him there was nothing more they could do and, on Friday evening, Giardinieri said goodbye to his wife and three children.
“I was at the point where I was barely able to speak and breathing was very challenging,” Giardinieri said. “I really thought my end was there.”
Then a friend sent him a recent article about hydroxychloroquine, a prescription drug that’s been used to treat malaria for decades and auto-immune diseases like lupus.
If you’ve read testimonials for alternative medicines for cancer or even testimonials for Stanislaw Burzynski, you know what’s coming next. Giardinieri’s testimonial is essentially the same thing:
Giardinieri said he contacted an infectious disease doctor about the drug.
“He gave me all the reasons why I would probably not want to try it because there are no trials, there’s no testing, it was not something that was approved,” said Giardinieri.
“And I said, ‘Look, I don’t know if I’m going to make it until the morning,’ because at that point I really thought I was coming to the end because I couldn’t breathe anymore,” Giardinieri continued.
“He agreed and authorized the use of it and 30 minutes later the nurse gave it to me.”
After about an hour after taking the pills, Giardinieri said, it felt like his heart was beating out of his chest and, about two hours later, he had another episode where he couldn’t breathe.
He says he was given Benadryl and some other drugs and that when he woke up around 4:45 a.m., it was “like nothing ever happened.”
He’s since had no fever or pain and can breathe again. Giardinieri said doctors believe the episodes he experienced were not a reaction to the medicine but his body fighting off the virus.
Sounds pretty dramatic, doesn’t it? In actuality, reading this testimonial made me think more than ever that it wasn’t the chloroquine that was responsible for Giardinieri’s remarkable recovery. He had only gotten one dose. Antivirals don’t usually work that fast. This is almost certainly a case of confusing correlation with causation. One also wonders if that “pounding heart” was a cardiac arrhythmia brought on by the drug. There’s no way of knowing for sure, though. In any event, no one’s listening to the caveats and the reasons to doubt these anecdotal stories. They’re only hearing this:
“To me, there was no doubt in mind that I wouldn’t make it until morning,” said Giardinieri. “So to me, the drug saved my life.”
This is the message people are getting. Meanwhile, here in Michigan, in response to the letter warning against hoarding and inappropriate subscribing of chloroquine and hydroxychloroquine, a man named Jim Santilli wrote a Facebook post complaining and describing his own “miracle cure” with hydroxychloroquine and azithromycin:
Of note is this passage. Note how similar to Giardinieri’s story Santilli’s story is:
On March 18th, I had a sudden onset of severe respiratory and cardiac issues. I immediately went to the hospital and they did a COVID-19 test. While waiting for the test results in the hospital, my breathing continued to worsen as treatment was received. On the morning of March 21st, I was not doing well and it was a major struggle to breathe. Feeling like I was slowly drowning, I honestly believed I would not live to see midnight. The x-ray that morning also showed my condition was worsening, including some collapsing in the lungs. Luckily, the infectious disease physicians decided to try a non-approved, experimental combination (Hydroxychloroquine and Azithromycin). After my first dose, I had a major improvement. My gasping for air stopped, and I was in tears of happiness due to having hope restored. I finally felt I would beat COVID-19 and it was no longer beating me. On March 22nd, I remained about the same. However, March 23rd brought a significant improvement. I continued to recover and was miraculously able to go home on March 24th to continue the treatment.
These are the narratives being promoted in the press and on social media. Indeed, Santilli’s story is showing up on the local Fox News broadcast, with a slanted report that makes it sound that the drug combination is definitely what saved him. Were hydroxychloroquine and azithromycin responsible for these handful of “miracle recoveries”? We really have no way of knowing without a randomized clinical trial. One thing is for certain. As is the case for alternative cancer cure testimonials, nothing will convince these patients that the “miracle drug” probably wasn’t what resulted in their improvement, and their stories sound convincing to the medically untrained. Worse, I predict that, even if the clinical trials are clearly negative, these sorts of stories will drive conspiracy theories that “they” (e.g., big pharma) covered up the evidence that these drugs work. Maybe the worst possibility of all is that we will never know for sure if these drugs work because the premature hype precludes completing a decent randomized clinical trial of sufficient power to answer the question definitively because no one will agree to be randomized to placebo. That is a distinct possibility, especially now that the FDA has caved to pressure and approved the use of these drugs against COVID-19 despite the extreme paucity of clinical effectiveness.
Enter the grifters and snake oil salesmen
Unsurprisingly, America’s Quack, Dr. Mehmet Oz, has jumped on the chloroquine bandwagon (because of course he has—it’s the sort of thing he does). Here is Mr. Giardinieri being interviewed by Dr. Oz on a segment on The Sean Hannity Show:
Dr. Oz on benefits, risks of using hydroxychloroquine to treat Coronavirus
Cardiac surgeon Dr. Mehmet Oz discusses benefits and risks of using hydroxychloroquine 'off-label' to treat coronavirus
Posted by Sean Hannity on Wednesday, March 25, 2020
Note that Dr. Oz’s take on Raoult’s study is completely credulous, and he says that he interviewed Raoult, because of course he has. He also reported that Raoult now asserts that it’s unethical to withhold hydroxychloroquine and azithromycin from COVID-19 patients, which just goes to show that he has no clue about the concept of clinical equipoise. Even worse, he’s parroting anecdotes while referring to them as “studies.” (None of them, other than Raoult’s studies and the negative Chinese study of chloroquine are published yet.) In fact, it’s profoundly unethical of Dr. Oz to promote this as yet unproven treatment. Looking over Dr. Oz’s website, it exploded yet another of my irony meters to see that his Thursday show this week will be “The COVID-19 Pandemic: Beware of Scammers Trying to Take Advantage of Your Fear of the Virus.”
Just look at Dr. Oz’s interview with Prof. Didier Raoult if you don’t believe me. Unsurprisingly, when Dr. Oz asks Prof. Raoult if there were any differences in clinical outcomes in the patients treated with his combination, he dodged the question.
Meanwhile, we have doctors like Dr. Vladimir Zelenko in New York is promoting an unproven drug cocktail involving hydroxychloroquine and posting videos like this that prove nothing:
🚨WATCH: The latest video from a leading physician in Kiryas Yoel, NY, Dr. Zelenko, regarding the his findings after treating a select high risk group of 699 patients in the past week w the chloroquine combination drug approved to treat COVID19 patients #COVID19 #Corona #hope pic.twitter.com/bLnWC82YSB
— Michalli 🦋 מיכל (@86thatplease) March 27, 2020
Meanwhile, he’s making incredibly irresponsible claims:
Zelenko is one of a handful contending it should be in widespread distribution to people at higher risk of having a serious case of Covid-19 with mid-level symptoms, most often without even confirming their illness is in fact connected to coronavirus.
He wrote in the emails sent on Friday that his clinic had so far given 669 outpatients the drug cocktail, and that none had died. He attached a spreadsheet in which he listed 54 high-risk cases, including three who required hospitalization.
In an interview Friday, Zelenko encouraged doctors to resist calls from infectious disease experts to prescribe the drug only as part of clinical trials and to critical patients.
“This is a World War III situation — it’s the virus versus humanity,” he said. “If we were to adopt their approach, there would be an extra million dead people.”
There is zero evidence that withholding hydroxychloroquine from mild cases will result in an extra million deaths. Dr. Zelenko’s actions and words are irresponsible and unethical.
It’s even worse, though. It’s not just hucksters like Dr. Oz and irresponsible doctors like Dr. Zelenko. Now, a shadowy conservative business group founded by a big time political donor to the Republican Party is entering the fray:
A conservative business group founded by a prolific Republican political donor is pressuring the White House to greenlight an unproven COVID-19 treatment, saying in an online petition that the country has plants in the U.S. ready to produce a drug but can’t because of “red tape, regulation, and a dysfunctional healthcare supply chain.”
In recent days, Home Depot co-founder Bernard Marcus’ Job Creators Network has placed Facebook ads and texted supporters to sign a petition urging President Donald Trump to “CUT RED TAPE” and make an anti-malarial drug called hydroxychloroquine available for treating those sickened with the virus, one such message obtained by ProPublica reads.
Mark my words, the same people who foisted the deceptive “right-to-try” law on us in order to weaken the FDA will take full advantage of the COVID-19 pandemic to further weaken the FDA in the name of “speeding up cures” and “cutting red tape.”
Finally, are stem cell quacks getting in on the action? I think you know the answer to that question:
Today we were joined by a very prominent guest in the medical field!
He sits down with us to discuss a very promising development, stem cell therapy to bolster immunity and ultimately defeat the disease.
Head to https://t.co/J0eGAZktZ8! pic.twitter.com/1F4FJjlOg6
— Rudy W. Giuliani (@RudyGiuliani) March 28, 2020
Yes, Rudy Giuliani is promoting not just hydroxychloroquine, but he’s also promoting stem cell quackery and cells from placentas:
Our special guest today on Common Sense describes the process of extracting placenta ”Killer Cells” and their effectiveness in attacking cancer and virally infected cells.
Trials need to be EXPEDITED.
Head to https://t.co/J0eGAZktZ8
— Rudy W. Giuliani (@RudyGiuliani) March 28, 2020
I fear that, when all is said and done, the COVID-19 pandemic will be the single greatest opportunity for grifters and snake oil salesmen I’ve seen in my lifetime. Until a vaccine and/or effective treatment is developed, the grift will continue.
In the meantime, we wait the results of clinical trials and for science to do what it always does, as I find myself living in one of the hottest COVID-19 hotspots in the US.