
{kind=link}
“OK Mrs. Splanchnic, everything looks good. We’ll see you again in six months.” Dentists and dental hygienists all over the world repeat this phrase countless times each and every day. Sometimes however, our patients don’t get off so lucky; they will have to come back to have some procedure done – perhaps a filling, a crown, or (if they’re really unlucky) a toxic root canal. But if you are one of those people who have been told “see you in six months,” did you ever stop to consider why we say that to you? Why six months? Is it by coincidence or some grand design of nature it conveniently works out that 90% of people’s teeth just happen to get grungy enough to clean precisely at that six month mark? Are we just greedy and looking for ways to drag patients back in in order to fund the second Jacuzzi in our Gulfstreams? Or is there an evidence-based rationale for this time honored protocol?
Gather ‘round and settle in folks, because we have a lot of unpacking to do. And if you’re expecting some cut and dried science based answers, boy are you going to be disappointed!
First off, some basics
Prevention is the hallmark of modern healthcare. Despite claims by ideologically driven individuals accusing physicians, dentists, and “Big Pharma” of wanting to keep people sick because we can make more money by treating the disease, this is assuredly not the case. In dentistry, prevention takes many forms: from encouraging people to brush and floss, to eating a healthy diet (especially one low in cavity promoting carbohydrates), to the fluoridation of toothpastes, mouthwashes, and community water supplies.
In the dental office, prevention typically takes the form of the semi-annual examination and dental prophylaxis (or “prophy” if you want to use the cool lingo), also known as “The Check Up,” “The Six Month Recall,” or just “A Cleaning.” To keep it simple and consistent for the purpose of this article, I’m going to refer to it as the “Examination and Prophy” or E&P. Please note, Dude, that this is not the preferred nomenclature; it’s just the one I’m going to use here because I’m too lazy to think of anything better.
The E&P looks a little bit different in each office, and all of these steps aren’t done in every office at every appointment, but the basic components of the preventive dental appointment consist of:
- Review and update medical and dental history
- Blood pressure screening
- Oral cancer examination
- Examination of the teeth and periodontal tissues (i.e. gum tissue and supporting bone). This includes a visual examination for signs of dental caries (cavities), other problems with the teeth (chips, broken fillings, etc.), looking for signs of inflammation and infection, and periodontal probing, which measures the depth of the gum pocket. Just as in golf, the higher the number, the worse off you are.
- Radiographic exam. The content and timing of dental x-rays can vary and are customized to the needs and disease susceptibility of the patient. The dental team weighs risk vs. benefits when taking dental x-rays, keeping radiation exposure to a minimum using the ALARA (As Low As Reasonably Achievable) Principle. And no, dental x-rays don’t cause meningiomas or pose any significant risk to health. We do, however, go out of our way to make the x-ray packets (or sensors) as pointy and gaggy as possible. You’re welcome.
- We also do some specialized exams, depending on circumstances. If you are wearing a denture or a partial denture, for example, we’ll check those out. Kids with retainers, patients with sleep apnea or TMJ appliances, patients who are bleaching their teeth, etc.- we’ll review them as well.
- Then comes the actual prophylaxis (cleaning). This is the fun part where we scrape your teeth with metal hooks and/or use a power washer/jackhammer device to remove the calculus (tartar) and biofilm (plaque) from your teeth, followed by polishing them with sand.
- Application of a topical fluoride agent, when indicated.
- Usually at the end of the appointment, the dentist will come in and review all the findings and radiographs, make any necessary diagnoses, and recommend treatment, if indicated. If everything looks nice and healthy, he or she will say “OK, Mrs. Splanchnic, we’ll see you again in six months.” Which is awkward if your name is Mr. Glorb, but we dentists aren’t very good with names.
The legend of the six month recall
As the story goes (and it’s fairly well documented, so I do believe it is legit), the “scientific” basis of the twice a year cleaning came not from bespectacled dentists in the lab or in the clinic, meticulously studying the issue with experimental groups, control groups, and double-blinding; no, it was actually the fabrication of an advertising genius named Claude Hopkins in the early 1900s. Mr. Hopkins was the ad wizard who boosted Schlitz beer’s sales by claiming that Schlitz cleaned their bottles with “live steam” (failing to mention that all of the other brewing companies did too).
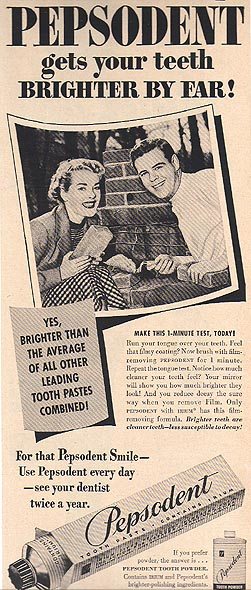
One day, a friend of Mr. Hopkins’ approached him with a new product, a minty, foamy toothpaste called Pepsodent. At the time, toothbrushing was rare; fewer than 7% of households had a tube of toothpaste (or can of tooth powder, as the case may be) in their medicine cabinets. Dental decay at the time was such an enormous public health issue that the U.S. Army declared it to be a national security risk during World War I. Hopkins agreed to launch an advertising campaign, and within five years he turned Pepsodent into one of the most famous brands on earth by associating brushing one’s teeth with health and beauty. Soon everyone, including Clark Gable and Shirley Temple, were promoting that “Pepsodent Smile.” “You’ll wonder where the yellow went when you brush your teeth with Pepsodent!” Within ten years of being introduced, an estimated 65% of households had a tube of Pepsodent in their medicine cabinet.
{kind=link}
After World War II, Pepsodent – still the leading toothpaste brand – created a new marketing catchphrase: “Use Pepsodent every day – see your dentist twice a year.”
Sadly, until that time, very little was being done in preventive dentistry. Most people did not have their teeth cleaned regularly and they would wait until something hurt or broke before they sought care. Cavities were painfully drilled out with a belt-driven slow speed handpiece (usually without anesthetic) and large amalgam fillings were placed. Root canal therapy was rarely done, implants were years away, and if a tooth was painful, it was summarily extracted. Dentures were the rule in people over sixty years old, not the exception like it is today.
Pepsodent helped to change all that. Behind the strength of its brand and the popularity of its product, its marketing slogans helped make toothbrushing a ritual in homes and embedded the importance of seeing a dentist for preventive care into the psyche of the American consumer. By the 1960s and 70s, other preventive measures appeared on the dental stage, namely the widespread addition of fluoride into toothpastes and municipal water supplies, and pit and fissure sealants, resin coatings applied to the grooves in the biting surfaces of back teeth where tooth decay is most likely to form. Tooth decay rates plummeted, and when cavities did occur, they tended to be smaller and easier to restore. Improvements in equipment (namely the high speed handpiece) and materials improved the quality of care as well. In the 1970s the insurance companies got into the dental game, covering many dental procedures. They soon learned that if they covered preventive care, their costs would be lowered down the line, so most dental insurance plans began paying for two cleanings per year, which further encouraged this interval. How did the insurance companies arrive at the six month figure? Insert shrug emoji here. My hypothesis is that they bought into the Pepsodent narrative.
{kind=link}
The actual science behind the six month recall
OK, so now we’ve established and accepted that the six month recall is the cornerstone of modern preventive dentistry. It’s taught in dental and dental hygiene schools worldwide and is practiced almost universally. It’s been elevated to the level of dogma, handed down on stone tablets from the dental gods on Mt. Sinai. So what does the science say? If you’ve read some of my previous Science Based Medicine posts or have listened to the podcast I co-host with fellow Science Based Medicine contributor Clay Jones, it won’t surprise you to learn that the science behind the six month recall is pretty lame, just like a lot of research is in dentistry.
{kind=link}
Insert sad trombone sound here.
I suppose at this point I should discuss what evidence actually does exist to support or refute the health benefits of a six month recall schedule. This is the Science Based Medicine blog after all, and they’re paying me big shill bucks to write this piece. Better give them what they want.
There are some research papers, including meta-analyses, that cover the recall interval as it pertains to various outcomes. A 2007 Cochrane Review by Beime, et. al. concluded that:
There is insufficient evidence from randomised controlled trials (RCTs) to draw any conclusions regarding the potential beneficial and harmful effects of altering the recall interval between dental check-ups. There is insufficient evidence to support or refute the practice of encouraging patients to attend for dental check-ups at 6-monthly intervals.
Across the pond, a 1977 Lancet article by Sheiham concluded:
Persons having dental examinations at intervals longer than 6 months were not at a disadvantage. They did not have more severe dental caries or periodontal disease than those attending at intervals of 6 months. Neither was there any evidence that an interval of more than 6 months would affect the prognosis for orthodontic treatment. Oral malignancies are rare in British populations, and routine 6-monthly screening to detect oral malignancies is unreasonable.
And in the British Dental Journal (2003), Davenport et. al. in a systematic review stated:
There is no existing high quality evidence to support or refute the practice of encouraging six-monthly dental checks in adults and children.
Insert embarrassed emoji here.
Are you starting to get the picture? Let’s press on and see what else is out there.
Another Cochrane Database Systematic Review by Riley et. al. (2013) concluded pretty much the same thing as everyone else, saying:
There is no evidence to support or refute the practice of encouraging patients to attend for dental check-ups at six-monthly intervals. It is important that high quality RCTs are conducted for the outcomes listed in this review in order to address the objectives of this review.
Studying whether recall intervals of varying lengths would have an effect on dental caries, Patel, et.al. summarized:
The authors conclude that the evidence for using a one-recall-interval-fits-all protocol to reduce caries incidence was weak. Studies that addressed the impact of recall interval on caries incidence were methodologically weak. The evidence was not strong enough to support using any specific one-recall-interval-fits-all protocol for all patients.
As you can see, there isn’t a lot of good data to support our recommendation for the routine six month cleaning. Part of it has to do with the quality and quantity (or lack thereof) of good dental research. Perhaps if a really robust and powerful study was done, it would support the six month recall. But then again, it might not. The other aspect to consider is that there are so many variables that each patient brings to the table, how could we even think a “one size fits all” approach would be appropriate in the first place? Factors such as age, diet, smoking, medical cofactors (e.g. diabetes), oral hygiene effectiveness, medications, genetics, socio-economic status, etc. all play into this mystical and complex algorithm. So what is a conscientious, science based dental patient to do?
Confused emoji.
Conclusion: Um…it isn’t not science based…
Warning: You are being redirected from the Science Based Medicine website to the Opinion Based Dentistry website.
I’ll repeat: What is a conscientious, science based dental patient to do?
Despite the lack of clear evidence in this area, I do believe some rational and logical recommendations can be made. First, I’ll describe what I and most of my science based colleagues do in our practices, and while we won’t be able to back up our rationale with solid evidence (see blog post above), I believe that it falls within the realm of biological plausibility and common sense. My medical colleagues are in the same boat in many areas: what is the appropriate interval for colonoscopies? Mammograms? There are guidelines to be sure, but it’s not a precise science.
Most of my patients are on a six month recall. There, I said it. Why? Because like it or not, that’s what patients expect, that’s what insurance pays for, it is an appropriate interval which keeps the majority of our patients mostly healthy, and I take comfort knowing that if a patient is in the early stages of gum disease or tooth decay, we can identify it early. I call this the Dental Recall Heuristic®, a “shortcut” algorithm which employs a practical method not guaranteed to be optimal or perfect, but sufficient for our immediate goals. Admittedly, I can’t back up our policy with rock solid science, but it’s the best we can do with the information we have. It might not be completely science based, but it isn’t not science based.
Many of our patients require a more frequent recall interval to maintain their oral health. Almost always these are patients with ongoing periodontal disease, and more frequent debridements and removal of plaque is often indicated to prevent progression of the disease. Some need more extensive periodontal treatment with a specialist. Conversely, some of our patients only need to be seen annually. Yes, a minority of our patients just have “good teeth.” For some in this hallowed demographic, it’s because they work really hard, brush and floss constantly, eat well, follow our advice, and help old ladies cross the street. Most in this category, however, are just lucky. They hit the nature/nurture lottery. They abuse their teeth just as much as the next guy or gal and aren’t that great at brushing or flossing, but for some reason they are decay and gum disease resistant. They don’t need to be seen every six months; it would confer very few benefits to them. I need to point out that we don’t make any money on these selfish people who only think of themselves. Some choose to have their teeth cleaned because they like it when their teeth don’t feel fuzzy, but that’s their choice, not our recommendation.
So circling back to what is appropriate for those dental consumers who are reading this post, here’s what I would recommend. If you are a “typical” dental patient, in the humpy middle part of the dental Bell Curve – i.e. you don’t get that many cavities, and while your dental hygienist may nag at you for not flossing enough, otherwise he or she says your gums are in “pretty good shape” – then go every six months. Just like changing the oil in your car regularly, it’s a good habit and it will help keep you in a state of dental health for your entire life. If, however, you have a history of periodontal disease, tooth loss, bleeding gums, deeper pocket depths (e.g. >3 mm), then it may be in your best interest to be seen more frequently. Discuss this with your dentist and/or dental hygienist to weigh the pros and cons for your particular situation. Don’t be afraid to ask questions, and your dental team should always be able to support their recommendations. Conversely, if you are a “golden child” like the ones I mentioned above – perfect teeth and gums, no issues, everything is happy happy clappy clappy – then you may be someone who can lengthen their recall interval to nine or even twelve months. Again, have the discussion with your dentist and/or dental hygienist.
On the other hand, if you’re not content to trust your oral health to Claude Hopkins’ ad campaign slogans, then I recommend some of the following resources to investigate the fascinating world of teeth and gums: The American Dental Association Center for Evidence Based Dentistry is a fantastic resource, easily searchable, and up to date; the Cochrane Database of Systematic Reviews; and of course PubMed.
Smart person emoji.
When there isn’t good evidence to support our claims or practices, we dentists are fond of saying “Dentistry is an art and a science!” This is one of those cases, but in the end, despite treading on shaky evidential grounds, it’s possible to maintain the health of your teeth and gums for a lifetime. So don’t forget to brush your dentist twice a day and visit your toothbrush once a year!