{kind=link}
The headlines from the start of the pandemic were horrific. “Shocking Video Shows The Bodies Of NYC Coronavirus Victims Being Forklifted Into A Refrigerated Truck Used As A Temporary Morgue” said one. “Bodies Of 750 Covid-19 Victims In New York City Remain In Refrigerated Trucks“, said another. There are many videos and photos documenting all this. Prisoners were asked to dig graves. Children who lost their parents described their loss. Myself and many countless healthcare workers wrote about what we witnessed. War analogies were common. One traveling nurse, who served in Iraq and Afghanistan, estimated that he saw 3,000 people die of COVID, saying “War doesn’t even compare to this…I would rather die, any other way of dying, than dying with coronavirus”. A doctor at Elmhurst Hospital in Queens said:
If you watch a war movie to see people shooting from all over, that’s what this almost felt like. One thing after the next after next, you can’t even catch up with what has to happen.
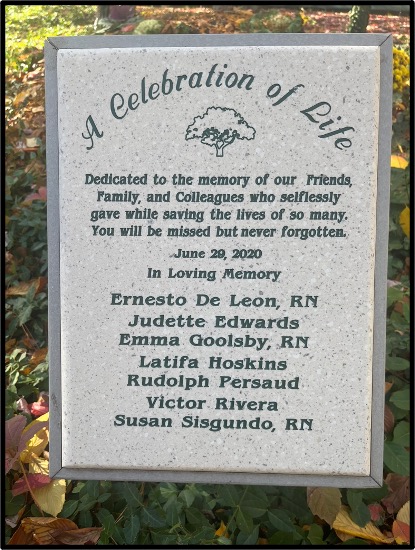
Many healthcare workers contracted COVID themselves, and not all of them survived, including friends of mine. This plaque now sits outside Bellevue Hospital to memorialize workers there who died during that first wave.
I say this all to make an important but simple point. You don’t need hard data to know that COVID hit New York City badly in the spring of 2020. Of course, variations of this would soon play out around the world. New York City was hit hard and early, but our experience didn’t turn out to be that much of an outlier, sadly. Hospitals continued to be deluged even after vaccines were available.
However, clever internet sleuths, safe on their couches, claim to have discovered something remarkable: None of this really happened. Myself and many thousands of others are said to have hallucinated or even caused the entire thing. I am referring to an article by Dr. Jessica Hockett, an educational psychologist, titled “More Questions about Spring 2020 Covid in New York City Hospitals“, which was recently posted at the anti-vaccine site, The Brownstone Institute. It claimed that “New York City’s hospital emergency departments were not at a breaking point in spring 2020. In fact, they were relatively empty and saw a 50% drop in visits”. This startling conclusion was based on five “observations”:
- NYC Emergency Departments weren’t overrun by people with COVID-19 (this is false).
- NYC Emergency Room respiratory visit spike may have been panic-driven (this is false).
- Most people who visited NYC emergency rooms between March 2020 and June 2021 for respiratory symptoms were not admitted to the hospital (many were admitted to the hospital).
- Many patients counted as COVID hospitalizations in spring 2020 were not admitted with COVID-like illness (CLI; this is false).
- The relationship between hospital inpatient deaths with COVID on the death certificate and people who were hospitalized because they had COVID is unclear (this is false).
The article (falsely) concluded that doctors may have been deadlier than the virus. It said:
It’s no wonder Michael Senger, Ethical Skeptic, and other analysts (including me) have said it was misuse of ventilators, protocol-induced staffing shortages, isolation, failure to treat, similar factors that resulted in thousands of Spring 2020 iatrogenic deaths in New York City and elsewhere.
Dr. Eric Burnett, an internist at Columbia University, deconstructed Ms. Hockett’s five “observations” on Twitter. It’s worth quoting his entire thread [Editor’s note: minor changes were made for readability and clarity].
This is absolute rubbish, coming from a non-clinician who never once treated a patient, let alone treated patients in the epicenter of a global pandemic. So allow me, a NYC hospitalist, to break apart this “analysis”. A brief look at this “analysis” shows that she relied heavily upon medical billing codes during the pandemic. This is not an accurate reflection of what we were actually seeing in the hospital as I will get to later. But let me address each of her claims one by one.
Her first claim: “NYC Emergency Departments weren’t overrun by people with covid-19.”
This is objectively false. Our ERs were over capacity for weeks during the initial surge. We had critically ill, ICU level patients intubated and vented in our ED, this hasn’t happened before. She backs this claim up by saying “Only 3% of the people who came to New York City hospital EDs during the spring 2020 March [were diagnosed – Ed.]” this is because we had little to no testing in March of 2020! The testing we did have was reserved for people who traveled from mainland China.
When we secured a test it took a week to get back bc there was only one lab that ran the PCR. We had to test patients for Flu and other resp viruses. When those were neg we gave them a presumed dx ofC19 (along with the clinical presentation supporting the diagnosis).
Saying our EDs weren’t overrun bc you didn’t see a lot of lab confirmed C19 at that time is ridiculous. On a personal note, we lost an ED physician to suicide bc of the sheer amount of devastation she bore witness to. It’s extremely disrespectful to suggest a this.
Claim number 2: NYC Emergency Room respiratory visit spike may have been panic-driven.
She backs this claim up by saying “But most emergency room visitors with respiratory symptoms were not diagnosed with covid. Huh.” I’ll refer you to my point about lack of testing above.
The amount of pts p/w acute hypoxemic respiratory failure was so great we had to train non pulm faculty on how to manage vents, HFNC, and BiPAP. We had ethics meetings about the possibility of scarce resource allocation should we run out of ventilators. This is not a normal.
Point 3: Most people who visited NYC emergency rooms between March 2020 and June 2021 for respiratory symptoms were not admitted to the hospital
We literally had to convert non-clinical spaces like our lobby into patient care units.
We had to convert a football field into a patient ward. We needed to expand hospital capacity in the state by 50% to accommodate admissions. Our traditional hospitalist census is around 100-110 patients, that ballooned to 250 during the worst of the surge. save me this excuse.
She backs this up by saying “Peak hospital admissions for covid-like illness (CLI) were 40% of respiratory emergency department visits”
We didn’t admit everyone with a respiratory illness. If they weren’t hypoxic then they didn’t get admitted.
That’s because our hospitals were over capacity and we couldn’t admit every single person with resp symptoms. It’s called triage, you should look it up. Only the sickest covid patients were admitted to the hospital.
Claim 4: Many patients counted as covid hospitalizations in spring 2020 were not admitted with covid-like illness (CLI). Data indicate that approximately 40% of inpatients with a covid diagnosis[…]from mid-March through April 2020 had not been admitted with covid-like illness.
This is what happens when you rely solely upon medical billing codes rather than talking to actual HCW. NYS issued immunity from record keeping liability during the worst of the pandemic. Medical coding [didn’t] accurately reflect the reality.
re medical record keeping liability:
“Including, but not limited to, requirements to maintain medical records that accurately reflect the evaluation and treatment of patients, or requirement to assign diagnostic codes, or to create or maintain other records for billing purposes.”When a patient came in with covid we documented it, but didn’t always list every other symptom they had. Medical billing and coding took a backseat to admitting and treating our patients, running codes, updating families, and trying to keep our patients alive.
Claim 5: The relationship between hospital inpatient deaths with covid on the death certificate and people who were hospitalized because they had covid is unclear.
This is also ridiculous. There is clear evidence of a spike in deaths during the peak of the pandemic. We needed morgue trucks to accommodate the overflow of dead patients as a result of this disease.
She attributes these deaths to iatrogenic causes without a shred of evidence to back it up. It’s clear she’s never taken care of a critically Ill covid patient. My guess is she never had to call a family member and tell them that their loved one died despite our best efforts.
She doesn’t have to live with the pain of making those calls. She never laid in bed awake at night worrying if her patients were still going to be there in the morning.
This is pure gaslighting at a time when healthcare workers are burnt out and leaving the profession in record numbers. If Jessica would like to join me on rounds this fall/winter during our respiratory virus surge I would be happy to accommodate her.
Something tells me Ms. Hockett will decline this invitation.
However, we again have the opportunity to witness a pernicious medical myth being created in real time. Despite abundant evidence to the contrary, sheltered disinformation agents will successfully convince many Americans that COVID’s threat was always overblown. Their message can be summarized as: Don’t believe the newspapers. Don’t believe the videos or photographs. Don’t believe the official death statistics. Don’t believe thousands of healthcare workers. Don’t believe gravediggers. Don’t believe those who lost multiple family members. We told you COVID wouldn’t be that bad in the spring of 2020, and we were right. Frontline doctors were always to blame.
Asking for “evidence” that New York City got hit hard by COVID makes as much sense as asking for “evidence” that New York City exists in the first place. George Orwell understood this all very well.