
{kind=link}
Before the pandemic, a frequent topic of this blog was the documentation of how rank quackery was being “integrated” into medicine to produce an unholy fusion dubbed “integrative medicine” or “integrative health” by its advocates. Rebranded from its previous name, “complementary and alternative medicine”—with the pithy acronym CAM, which was tossed aside because CAM adherents didn’t want the nostrums that they added to science-based medicine to be described as “alternative”—”integrative medicine” falsely promised patients the “best of both worlds,” the assumption being that there was a “best” of unscientific medicine based largely on religious prescientific understandings of how the body works and what causes disease to “integrate” into science-based medicine. Then the pandemic hit, and blogging about COVID-19 seemed to push nearly every other topic aside (for me, at least). However, just because we haven’t been paying as much attention as we used to do to the infiltration of what we used to like to call quackademic medicine into medical academia and then into community medical centers doesn’t mean that it didn’t continue during the pandemic, and not just in the form of claiming that various forms of alternative medicine could be used to treat or prevent COVID-19.
I was reminded of the continued creep of pseudoscience into medicine during the pandemic last week, which led me to write about a published four year follow-up of a negative study of acupuncture for debilitating joint pain caused by aromatase inhibitors (AIs), a class of drugs frequently used to treat breast cancer, that was spun as positive. Expecting that I’d come back to a COVID-19-related topic this week, I never expected that I’d be reminded yet again of how much quackery is infiltrating oncology and, worse, how much that quackery is being endorsed and promoted by the largest oncology professional society, but I was. That reminder came in the form of a news story from Healio, “Guideline provides recommendations for integrative approaches to manage cancer pain“, and the guidelines that it was referencing recommending some forms of “integrative medicine” to manage cancer pain. The guidelines were a joint project involving the American Society of Clinical Oncology (ASCO) and the Society for Integrative Oncology (SIO). Somehow I missed their original online publication back in September, which is why I’m grateful that the Healio publication popped up in my feed over the weekend.
The spin in the Healio story was clear:
The study — the first meta-analysis to examine natural, nonpharmacologic approaches to treat cancer pain — resulted in development of guidelines published in Journal of Clinical Oncology.
Healio spoke with researcher Jun Mao, MD, chief of the integrative medicine service at Memorial Sloan Kettering Cancer Center, about the importance of the study and the implications of the findings.
Dr. Mao summarizes the key findings of the study thusly:
- Recommend acupuncture for joint pain due to AI therapy.
- Recommend acupuncture for general pain management in cancer patients.
- Recommend massage therapy for palliative care of patients with pain due to advanced cancer. (I’ll note right here that, of the recommendations, this one is the least objectionable because, even if massage is generally a placebo, it is relaxing and feels good, something that I would never object to promoting in patients with advanced cancer.)
There are actually several more recommendations in the guidelines, which is why I find it rather interesting that Dr. Mao chose to focus on these three (two, actually, if you count recommending acupuncture for pain due to cancer or cancer treatment to be one recommendation). In particular, you’d think that he would have been interested in highlighting more plausible “integrative” treatments, such as herbal medicines, which, depending on the specific herbs, might actually contain pharmacologically active components, in particular given that the paper itself states that the panel constructing the guidelines had sought to answer two questions:
- What mind-body therapies are recommended for managing pain experienced by adult and pediatric patients diagnosed with cancer?
- What natural products are recommended for managing pain experienced by adult and pediatric patients diagnosed with cancer?
It interested me how little verbiage was devoted to the second question compared to the first.
Also, there are two things you need to know before I dig in. First, Dr. Mao is a past president of SIO. Second, the Journal of Clinical Oncology (JCO) has been thought to be one of the best oncology journals out there. Certainly, it’s one of the most read and influential, with an impact factor of 50.717, placing it among the top 1% of academic journals. This is an astoundingly high IF for a specialty journal. By comparison, for example, the New England Journal of Medicine, a generalist medical journal, has an IF of 176.079; Nature, 69.504; and Science, 63.714. I do realize the problems with impact factors as measurements of a journal’s reach and influence, but by any standard, JCO is in at least the top 20 journals in the world, and it is widely read by pretty much every oncologist, as well as radiation oncologists and surgical oncologists (like me). So promoting “integrative oncology” in JCO is a big deal, with ASCO clearly putting its considerable weight behind these guidelines. It’s an indication that, depressingly, ASCO has gone all-in with integrative medicine quackery.
“Integrating” magical quackery with medicine
When it comes to “integrative medicine” or “integrative oncology,” framing is everything, as has been discussed more times than I can remember on this very blog. So it’s useful to see how Mao et al. frame the questions to be answered and the existing evidence base that led them to undertake this review. After correctly emphasizing that pain is a common problem in cancer patients and can be due to cancer, cancer treatments (surgery, radiation, and chemotherapy), or a combination of the two, Mao et al write:
As pain in patients and survivors of cancer is complex with different etiologies (eg, tumor burden, treatment-related, and non–cancer-related) and varying presentations (eg, neuropathic and musculoskeletal) and duration (eg, acute and chronic), pain management requires an interdisciplinary approach and should include both pharmacologic and nonpharmacologic treatments, where appropriate.
Of course, no one—and I do mean no one—would disagree with such a general and unobjectionable representation of pain management, even those of us here at SBM, who have long lamented the infiltration of quackery into medicine. The question, of course, is what is defined as “nonpharmacological treatments.” As I’ve discussed many times, evidence-based “nonpharmacological treatments” for pain are not the same thing as CAM or “integrative medicine,” no matter how much advocates try to conflate the two in order to persuade you that their nostrums are science- and evidence-based. Again, this is a common framing by integrative medicine advocates, which leads to the predictable follow-up:
An estimated 40% of patients with cancer use integrative medicine on an annual basis. The key guiding principle of integrative medicine is to use these interventions along with conventional pain management approaches (eg, medications, radiation, injections, and physical therapies) and it is not intended to replace conventional interventions.
Patients often seek integrative medicine because they perceive that conventional medical treatment is not completely meeting their needs, fear side effects from pharmacotherapies, prefer a holistic approach, or because it has been recommended by their family or health care providers. A growing number of well-conducted randomized controlled trials (RCTs) have found that interventions such as acupuncture or massage can alleviate pain in patients and survivors of cancer.
It’s a very common framing by “integrative medicine” advocates: First, present the unmet medical need in an unobjectionable manner that can’t really be argued against very strongly, if at all—in this case, better pain management in cancer patients. Next, frame “integrative medicine” as “nonpharmacological treatment” for that unmet need. Then appeal to the popularity of “integrative medicine”—40% use it!—while citing studies that define it as broadly as possible in order to come up with such large percentages. Finally, hype data that purportedly shows that theatrical placebos like acupuncture “work” in order to justify your study, which you know will be “positive” in at least some way.
So how were these guidelines arrived at? In brief, they were developed using a methodology that is often used to develop expert consensus guidelines, specifically an “Expert Panel was convened to develop clinical practice guideline recommendations on the basis of a systematic review of the health literature,” which was done thusly:
This SR-based guideline product was developed by an international multidisciplinary Expert Panel, which included a patient representative and a health research methodologist (Appendix Table A2, online only). The Expert Panel met via video conferences and corresponded through e-mail. Based upon the consideration of the evidence, the authors were asked to contribute to the development of the guideline, provide critical review, and finalize the guideline recommendations. The guideline recommendations were sent for an open comment period of two weeks allowing the public to review and comment on the recommendations after submitting a confidentiality agreement. These comments were taken into consideration while finalizing the recommendations. Members of the Expert Panel were responsible for reviewing and approving the penultimate version of the guideline, which was then submitted to the Journal of Clinical Oncology (JCO) for editorial review and consideration for publication. All SIO-ASCO guidelines are ultimately reviewed and approved by the Expert Panel, the SIO Clinical Practice Guidelines Committee, and the ASCO Evidence Based Medicine Committee before publication. All funding for the administration of the project was provided by SIO.
Of note, the members of this panel and the authors of these guidelines are all believers. Indeed, a number of names on the author list are familiar. Some are past presidents of SIO, such as Heather Greenlee, who is a—cringe—naturopath and an author on the study of acupuncture for AI-induced joint pain that I discussed. She’s also been associated with a number of efforts by SIO over the years to “integrate” quackery with oncology, in particular the care of breast cancer patients, although she has been instrumental in promoting “integrating” magic into oncology for all cancer patients as well. Claudia Witt also came to mind. She is Director of the Institute for Complementary and Integrative Medicine at the University of Zurich. Worse, she’s a believer in homeopathy, as Mark Crislip noted way back in 2010. Dr. Witt has argued that CAM is cost effective without actually showing that it’s effective and was lead author on a desperate attempt to define just what the heck “integrative oncology” is. Then there’s Ting Bao, immediate past president of SIO and believer in acupuncture.
Personally, whenever I look at guidelines, I like to look at the very strongest recommendation that the guideline panel comes up with, examine the evidence used for it, and then judge whether the recommendation is justified. For this set of guidelines, there’s clearly one recommendation that is first and strongest, that acupuncture should be offered to patients experiencing AI-associated joint pain:
Recommendation 1.1.
Acupuncture should be offered to patients experiencing AI-related joint pain in breast cancer (Type: Evidence based, benefits outweigh harms; Evidence quality: Intermediate; Strength of recommendation: Moderate).Literature review.
Four SRs and five RCTs were conducted in the area of acupuncture and AI-related joint and muscle pain.19,27-30,44-47 The most definitive evidence is from a phase III sham-controlled RCT conducted among 226 patients with moderate to severe AI-related joint pain.19 After 6 weeks, true acupuncture reduced pain significantly more than sham acupuncture and standard of care (waitlist control; 2.05, 1.07, and 0.99 points, respectively, on a 0-10 point NRS). After 6 weeks, there were more responders who had a clinically meaningful change in pain (a two-point reduction on a 0-10 scale) 253 in the true acupuncture group compared with the sham and waitlist control groups (58%, 33%, and 31% respectively).
I wrote about the study in reference 19 in 2018, when it was first published. While it did include a waitlist, no intervention (at least initially) control group, which was good, it was not a double-blinded study. Despite the contortions that the authors went through to justify no blinding of the acupuncturists (specifically, the authors claimed that sham needles didn’t work and fooled no one, a claim not supported by other studies that did successfully use sham needles), the results of the study, given the very small effect size reported in the true acupuncture group, were actually most consistent with no clinically significant effect from acupuncture on AI-associated joint pain. Also, as I pointed out, the follow-up study published this month to examine long-term effects and treatment durability was no more positive, given how over time the differences between the true acupuncture and sham acupuncture groups fluctuated from nearly zero to still tiny and between statistically significant and mostly not statistically significant. In this, it was consistent with previous studies of acupuncture use to treat AI-associated arthralgias that we’ve written about going back to at least 2014 in that it was entirely consistent with placebo effects but spun as evidence that acupuncture is very effective against AI-associated joint pain.
I also find it rather interesting that for this, the very strongest recommendation made in this review, the best that even believers could say about the strength of the evidence was that the evidence quality was intermediate and the strength of recommendation was moderate. Let’s just say that it goes downhill rapidly from there. For example, the guidelines recommend yoga for AI-related joint pain, but the recommendation strength is weak, but based on evidence quality characterized as low. Yoga is also recommended for people experiencing pain after treatment for breast or head and neck cancers, again with low quality evidence and a weak recommendation.
In fact, rather than going through each recommendation in turn, I think I’ll just reproduce this chart from the paper, which is rather interesting in and of itself, for reasons that I’ll list after you have a chance to look at the chart without my commentary:
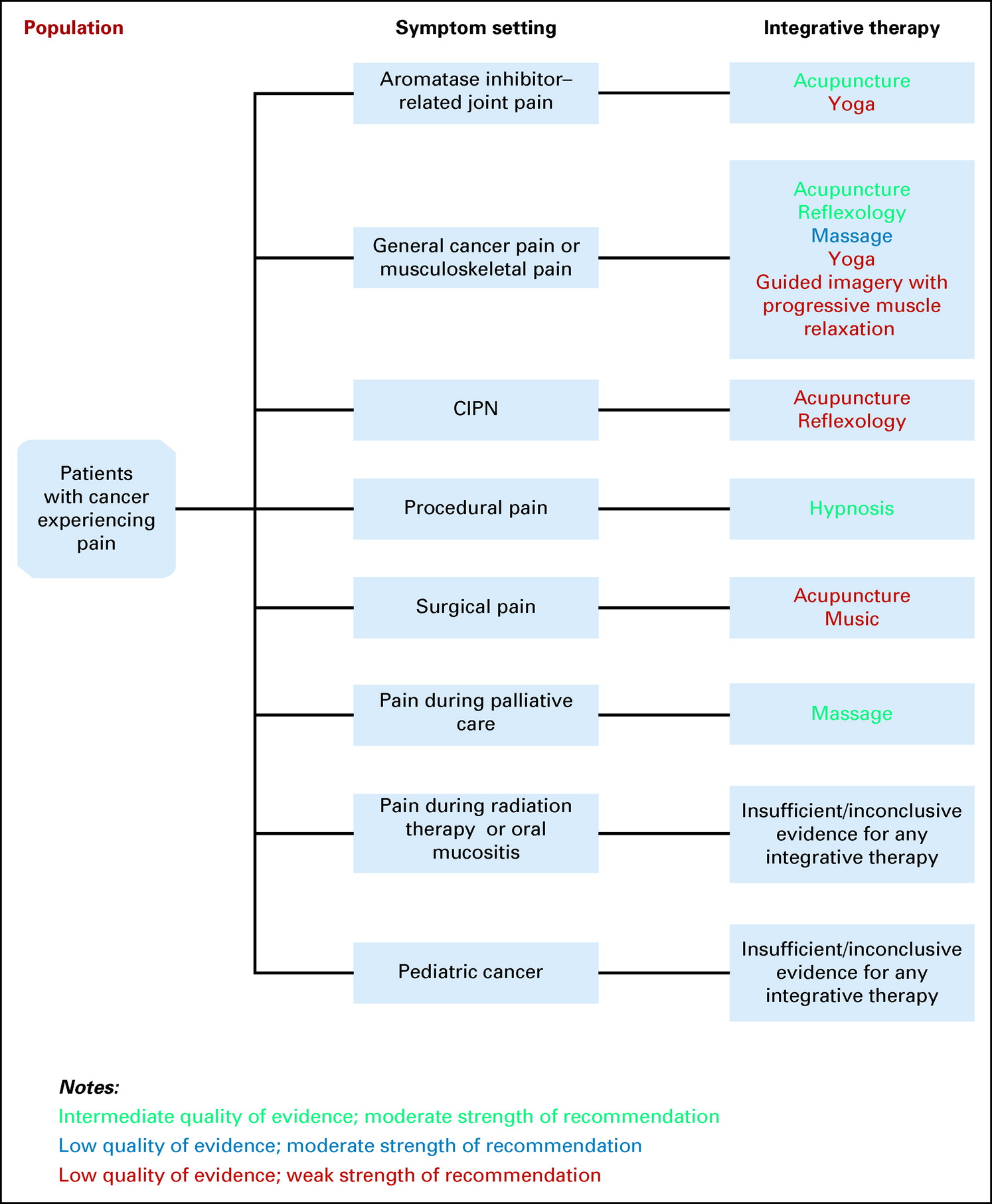
SIO-ASCO recommendations for “integrative” medicine interventions for pain related to cancer and cancer treatments.
I’ll admit that I stole a bit of the thunder here by mentioning earlier that the very strongest recommendation is “intermediate” strength and the very strongest evidence cited is “moderate,” with the disclaimer that “benefits outweigh harms.” In any event, notice how little green there is (“intermediate quality of evidence, moderate strength of recommendation”) compared to black (“insufficient/inconclusive evidence”) plus blue (“low quality of evidence, moderate strength of recommendation”) plus red (“low quality of evidence, weak strength of recommendation”). Also note the modalities listed after first noting the literature search strategy used to search randomized controlled trials (RCTs), systemic reviews (SRs), and meta-analyses:
The recommendations were developed by using a SR of evidence identified through online searches of PubMed (1990-2021) and Cochrane Library (1990-2021) of RCTs, SRs, and meta-analyses. Articles were selected for inclusion in the SR on the basis of the following criteria:
- Population: Adults and pediatric patients experiencing pain during any stage of their cancer care trajectory
- Interventions: Integrative interventions for pain management, including acupuncture, acupressure, mind-body therapies, and natural products (note: see details in the Data Supplement, online only; therapies focused on pain prevention were not included)
- Comparisons: No intervention, waitlist, usual care (UC) or standard care, guideline-based care, active control, attention control, placebo, or sham interventions
- Outcomes: Pain intensity, reduction, or change in symptoms reported as the primary outcome in published manuscript
- Sample size: Minimum total sample size of 20
Articles were excluded from the SR if they were (1) meeting abstracts not subsequently published in peer-reviewed journals; (2) editorials, commentaries, letters, news articles, case reports, and narrative reviews; or (3) published in a non-English language. The guideline recommendations were crafted, in part, using the Guidelines Into Decision Support methodology and the accompanying BRIDGE-Wiz software program.25 In addition, a guideline implementability review was conducted. On the basis of the implementability review, revisions were made to the draft to clarify recommended actions for clinical practice. Ratings for type and strength of the recommendation, and evidence quality are provided with each recommendation. The quality of the evidence for each outcome was assessed using the Cochrane Risk-of-Bias tool26 by the project methodologist in collaboration with the Expert Panel cochairs and reviewed by the full Expert Panel.
All of this is fairly standard in guideline construction. I’ll include the flow chart for the literature search and selection for a reason that you will see in a moment but hope that you’ll be able to glean a bit before I explain:
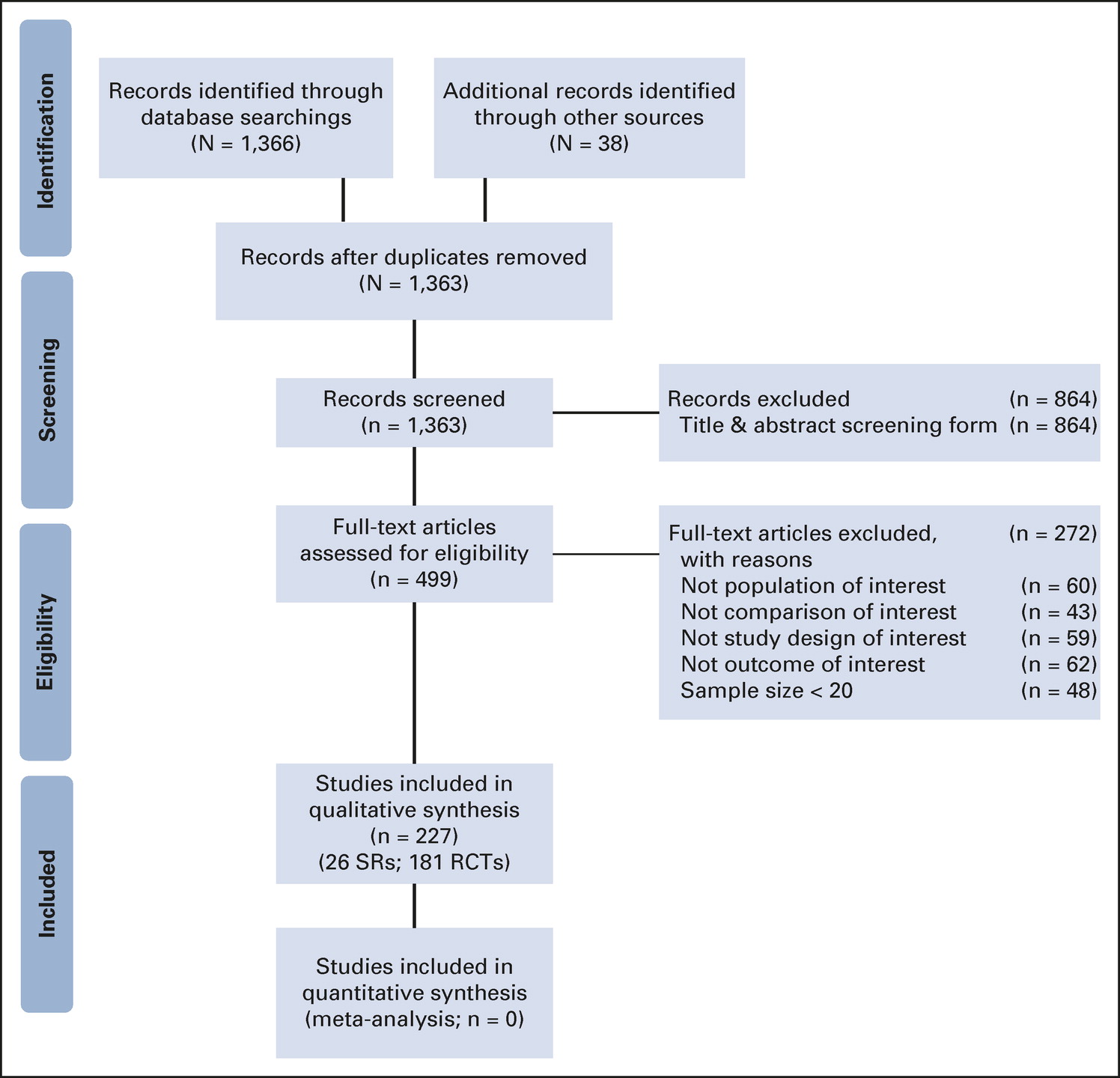
Guidelines flow chart.
While it’s not unusual for the winnowing of articles from initial search to articles used in a systemic review or meta-analysis to be severe, given the broad search strategy I was actually rather surprised at how few articles were found initially involving relatively few modalities, which boiled down to acupuncture/acupressure, reflexology, yoga, massage, hypnosis, guided imagery, and music therapy, none of which produced evidence rising above an even generous characterization of intermediate quality or recommendations above moderate strength.
Interestingly (to me, anyway), herbal products were pretty much a bust, which is why none of them made it into even the 13 weak-to-moderate strength recommendations based on low-to-intermediate quality evidence. For natural products, the evidence taken as a whole was either inconclusive, for example:
There is insufficient evidence to recommend for or against the use of Xiao Zheng Zhitong paste, Jinlongshe granule, Shuangbai San paste, or Xiao-Ai-Tong decoction for general cancer pain. Four trials tested the effects of Chinese herbal preparations on treating general cancer pain, including Xiao Zheng Zhitong paste in patients with a range of different cancer types, Jinlongshe granules in patients with gastric cancer, Shuangbai San paste in patients with liver cancer, and Xiao-Ai-Ton decoction with and without morphine in patients with a range of different cancer types. Given that there was only one trial of each treatment intervention, variability in quality of the trials, there are insufficient data to make a clinical recommendation.
Or negative, for example:
Two RCTs tested the effects of glutamine on the incidence and severity of peripheral neuropathy. The first trial was a moderate-size (N = 86) trial comparing oral levo-glutamine compared with no intervention in patients with colorectal cancer receiving oxaliplatin. Patients who received levo-glutamine had lower incidence and severity of peripheral neuropathy symptoms; however, the trial did not control for placebo effects. The second smaller trial (N = 43) compared oral glutamate to placebo in women with ovarian cancer receiving paclitaxel. There were no differences between groups in incidence of peripheral neuropathy; patients who received glutamate reported lower pain severity. No clinical recommendations can be made on the basis of these results because of low study quality and/or small sample size.
If I were going to predict something about this systematic review the guidelines that result from it, I would have predicted that there would be at least one herbal treatment that showed promise, given that herbal treatments always have the possibility of containing one or more pharmacologically active compounds, compared to something like acupuncture, which is nothing more than an elaborate theatrical placebo.
Given how often we’ve discussed the biological implausibility of acupuncture, I’ll discuss reflexology instead. If acupuncture, with its “meridians” and claim that it works by altering the flow of qi (life energy) through those meridians is pure prescientific nonsense, then what can one say about reflexology, which proposes that every one of your organs “maps” to someplace on your feet? Here’s a representative chart that I pulled up just by Googling the term “reflexology”:
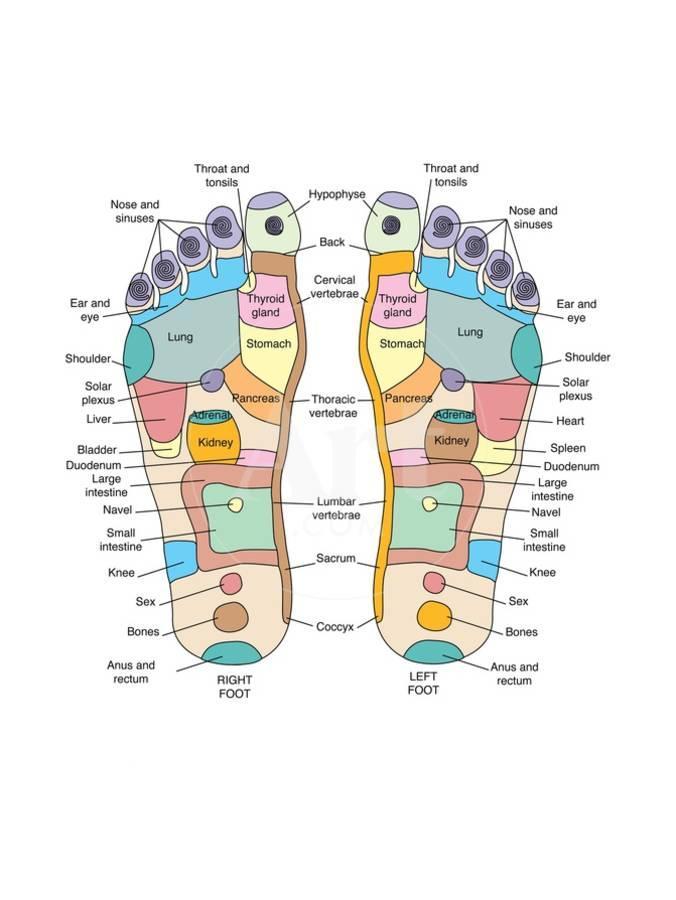
A representative reflexology foot map. This is not how human anatomy works!
The idea behind reflexology is that by applying pressure to these various locations on the foot you can impact the function of the organ to which that location supposedly maps. That’s not how human anatomy works, and attempts to “modernize” reflexology have utterly failed to make it less utterly ridiculous from an anatomical and physiological standpoint. Unfortunately, like the case for acupuncture, its scientific implausibility and lack of evidence haven’t stopped some states from licensing its practitioners.
ASCO embraces nonsense
I’ve written on a number of occasions before how ASCO has increasingly embraced the nonsensical pseudoscience behind quackery like acupuncture, reflexology, and more. I was first gobsmacked by the blatantness of its embrace eight years ago, when I attended an ASCO meeting that featured a major session on “integrative oncology” full of credulous acceptance of alternative medicine modalities. Then, a few years ago, ASCO endorsed guidelines for the use of “integrative therapies” in the treatment of breast cancer patients, thus leading to a post by me explaining just how harmful this embrace of quackery was to cancer patients. I supposed that I shouldn’t have been too surprised, given that in 2010 JCO published a very disappointing editorial about a cancer treatment that was obviously rank quackery.
Unfortunately, ASCO and its journal JCO are not alone, as this sort of “integration” of quackery with medicine is finding its way into many journals, academic medical and cancer centers, and even NCI-designated comprehensive cancer centers. There are even, increasingly, training programs claiming to produce the next generation of “evidence-based” integrative practitioners, despite the inherent contradiction between “evidence based” and “integrative” practice.
It’s hard for me not to see a connection between the infiltration of the Trojan horse that is “integrative medicine” into academic medical centers and the tsunami of COVID-19 misinformation that we’ve been enduring. “Integrative medicine” trains physicians to ignore prior plausibility and embrace treatments that are wildly implausible from a basic biology perspective, and we’ve now seen a disturbingly large minority of doctors do the same thing with respect to COVID-19. You might think I’m overreaching, and it’s possible that I am, but when you embrace unreality in one area of medicine, how do you prevent that unreality from metastasizing to other areas of medicine? We normally expect professional societies like ASCO to be champions of science- and evidence-based medicine. Unfortunately, we are not living in normal times, and haven’t been since before the pandemic. The pandemic just accelerated the embrace of unreality.