{kind=link}
The Claim: “A Positive Test For Coronavirus Does Not Mean Necessarily That This Virus Is Always Primarily Responsible For A Patient’s Demise”
Consider the following statement by right-wing rocker Ted Nugent:
They claim five hundred thousand people have died from COVID-19. Bullshit. I believe that medical examiners in all 50 states have gone, ‘I put down on the death certificate that he died of asphyxiation, but they made me put COVID.’ ‘Well, this guy was stabbed to death, but they made me put down COVID.’ ‘This guy was run over by a tandem gravel truck doing a four-wheel drift and the crows be pecking at your flesh, but they made me put down COVID-19.’
Implying that doctors have significantly inflated COVID-19 deaths without compelling evidence is an inflammatory charge. It would completely upend our understanding of the pandemic if it were true. It’s relatively easy to recognize Mr. Nugent as an ill-informed conspiracy-theorist. No journal editor would invite him to present his views in an article. Were Mr. Nugent, who after his COVID-19 diagnosis said he’s “never been so scared in all my life,” to make this claim in a medical seminar, he would rightly be jeered off the stage.
So, what is the proper reaction when a highly credentialed scientist makes nearly identical claims, only in the formal, cautious diction of scientific discourse? I am referring to Dr. John Ioannidis, a professor of epidemiology and population health at Stanford University. I greatly admired Dr. Ioannidis prior to the pandemic and quoted him favorably several times in my previous work. So, I really mean it when I say writing this article gives me no pleasure. I feel very uncomfortable and vulnerable, to be honest.
But let me share his words from an interview given in April 2020:
There is some contentious issue about what exactly should count as a COVID-19 death. For example, in the last few days (in New York City) we have seen a very large number of probable COVID-19 deaths being added to the figures, and these are deaths where we have not documented with laboratory testing the presence of the virus, so they are pretty presumptive in terms of whether these are deaths that were caused by COVID-19, COVID-19 was present, but not really a key player in the demise of the patient. So, I think we need to wait and see some mature data on what exactly the contribution of the virus has been in different deaths that we have documented. In Italy, where we have some more mature data, we see that close to 99% of people have underlying diseases, actually in most cases multiple underlying diseases and underlying causes that could also have led them to death. In the US, it seems to be less, but we would need to get some more in-depth analysis of what exactly is killing these people and how.
In the same interview he said the following:
So, the data in Italy suggest that it’s very difficult to differentiate between deaths by SARS-CoV-2 and deaths with SARS-CoV-2. Since we had close to 99% of people dying have other causes that may have contributed to their demise, it’s very difficult to dissociate and say that these people specifically died because they were infected. It’s very likely that many of them would have died anyhow, if not immediately within a very short period of time, because of these other causes of death that they had. I think this is an ongoing debate…
Countries use very different systems of recording deaths, and we know, not just from the COVID-19 era, but also from the past, that filling out death certificates can be very tricky. We know that death certificates often are pretty inaccurate, and if you create an environment where people believe that this is the cause of death, that is really the most prominent at the moment, they may subconsciously or unconsciously prefer to list COVID-19 as a major cause of death in the certificate, even though it may be less significant contributor if not an innocent bystander in some cases. This is very difficult to tell at the moment because, as you realize, the battle is still ongoing. But at some point, we need to go back and check very carefully and try to understand what exactly did the virus do to all these people.
If we do that, we will also be able to estimate how many years of life were really lost, because it’s not just the number of deaths, it’s the number of person-years lost that matters the most. If you have someone who is young and healthy and has no other problems and suddenly dies in their twenties, this is a very large number of person-years lost compared to someone who is very old and has multiple reasons to die, and is already dying from something else and you just happen to find a PCR positive test for SARS-CoV-2 in a nasal swab. The number of person-years lost is very small and you’re not even sure that SARS-CoV-2 really did contribute to their death substantially.
Dr. Ioannidis first expressed this sentiment early in the pandemic, writing on March 17th, 2020 that “A positive test for coronavirus does not mean necessarily that this virus is always primarily responsible for a patient’s demise”. Though this belief has since become widespread, this is the earliest instance I found of someone asserting that the virus might not to blame when someone dies after contracting it. The idea that many people are dying with the virus, not from the virus, remained a feature of his interviews and publications. It’s worth quoting Dr. Ioannidis’s statements in full:
- Now, your point that we’re literally counting, as opposed to estimating, deaths from coronavirus is correct. But I’ll push back that this may not yield mortality figures as accurately as people think. Because of the attention on coronavirus, we’re better at knowing that a deceased person had coronavirus than had the flu. This means we’re good at knowing when someone died with coronavirus — but not necessarily that they died from the infection. We assume that dying with coronavirus is dying from coronavirus. (Medscape)
- So, this is also an open question. Because for the data that we have more mature and detailed information, like the data from Italy that has already through the peak of their epidemic wave, we realize that 99% of people who die with this virus have other reasons as well to die. On average, they have close to three other reasons to die. On average they are 80-years-old with other comorbidities, as we say, and there’s quite some debate on whether these people would have died anyhow, if not immediately, you know, perhaps in a few days or in a few weeks or a few months. In our country we see a fairly similar picture. We see that people who are disadvantaged, poor people, creating even further inequality in the population through COVID-19, seem to be very hard hit. We see that the age of death on average is a little bit lower compared to European countries, in the range of 73 or 74-years-old, and we see again lots of comorbidities in people who die with COVID-19. It’s very hard to say how many of these people would have died anyhow and how much is the direct contribution of the virus. These data are evolving, but if anything they suggest that the burden of disease as we call it, the number of person-years lost, how many years of life are being lost, is much less than even what the number of deaths would suggest. This is not to minimize the problem. It is a serious problem. (Fox; start listening at 5:05)
- COVID-19 has become a notifiable disease, so it is readily recorded in death certificates. What we do know, however, is that the vast majority of people who die with a COVID-19 label have at least one and typically many other comorbidities. This means that often they have other reasons that would lead them to death. The relative contribution of COVID-19 needs very careful audit and evaluation of medical records. (Greek Reporter)
- Finally, a major question that should be answered is the causal contribution of SARS-CoV-2 infection to related deaths. It is difficult to differentiate between deaths with SARS-CoV-2 infection and deaths caused by SARS-CoV-2 infection because the vast majority of patients who have died had 1 or more other major pathologies (98.8% with at least 1 comorbidity, and 48.6% having 3 or more diseases) that contributed to their death. (JAMA Internal Medicine)
- When I made that tentative quote (estimating that COVID-19 will cause fewer than 40,000 deaths in the US), I had not considered the impact of the new case definition of COVID-19 and of COVID-19 becoming a notifiable disease despite being aware of the Italian experience where almost all counted “COVID-19 deaths” also had other concomitant causes of death/comorbidities. “COVID-19 death” now includes not only “deaths by COVID-19” and “deaths with COVID-19”, but even deaths “without COVID-19 documented”. (Int J Forecast)
- The number of COVID-19 deaths can be both undercounted and overcounted, and the relative ratio of over- and under-counting varies across different locations. In most European countries and the USA it is more likely to be overcounted, especially if we are talking about “deaths by COVID-19″…For COVID-19 we are in early days, and we need to be careful to dissociate deaths from COVID-19 versus deaths that happened because of the disruption induced by lockdown. (Greek Reporter)
- Another observation that has emerged is that many of these people (in Italy) probably would have had very limited life expectancy in the absence of that infection, and it still remains to be decided how many of these infections are deaths with SARS-CoV-2 versus deaths by SARS-CoV-2, meaning that the virus has the key influence on the outcome rather than just giving a final kick or participating among many other factors in shaping the outcome, but these people having multiple other reasons that they would have a very poor endpoint and eventually die, many of them. (Daily Motion; start listening at 18:45)
Likely there are other instances where he expressed similar sentiments of which I am currently unaware.
Extraordinary claims require extraordinary evidence
It’s a truism that extraordinary claims require extraordinary evidence. As evidence for his claim that “A positive test for coronavirus does not mean necessarily that this virus is always primarily responsible for a patient’s demise”, Dr. Ioannidis cited “an autopsy series that tested for respiratory viruses in specimens from 57 elderly persons who died during the 2016 to 2017 influenza season”. The study found that “influenza viruses were detected in 18% of the specimens, while any kind of respiratory virus was found in 47%”. Oddly, the embedded link does not lead to this study, but rather to a study from 2013 of other coronavirus infections in living people. This paper concluded that, “Coronavirus infections in the elderly are frequent, likely causing substantial medical disease burden”, something we all know too well today. Perhaps Dr. Ioannidis has provided additional evidence elsewhere (he’s written a lot this pandemic and I haven’t read it all), though this is all I could find. If he chooses to write a paper on this topic in the future, I will read it with interest. It should not be off-limits for discussion.
Until he writes more however, it seems that the only evidence Dr. Ioannidis provides to support his extraordinary claim is a study showing that respiratory viruses were commonly found during 57 autopsies five years ago. But it does not follow from this study that a new, different virus, namely SARS-CoV-2, is an “innocent bystander” in many deaths of people today. If it did, it would be essentially impossible to attribute a large number of deaths to a new respiratory virus ever again. I wrote Dr. Ioannidis asking if he had any further evidence for his claim and whether he had altered his opinion at all, but I did not receive a reply.
Three areas of agreement: The vast majority of covid-19 deaths occur in older people who “have other reasons as well to die”
Let me share three areas of agreement.
First, it is true that most COVID-19 deaths occur in older people who “have other reasons as well to die”. According to the CDC, “For over 5% of these deaths, COVID-19 was the only cause mentioned on the death certificate. For deaths with conditions or causes in addition to COVID-19, on average, there were 4.0 additional conditions or causes per death”. This can make it difficult, in very limited circumstances, to tell when someone dies with the virus or from the virus. During the pandemic’s peak in New York City, when morgues were overwhelmed, Dr. Oxiris Barbot, the commissioner of the city’s Department of Health said that “Any patient who has had a positive coronavirus test and then later dies — whether at home or in a hospital — is being counted as a coronavirus death”. Based on this broad definition, some deaths with incidental SARS-CoV-2 infection are assuredly included in the official statistics in the US.
Governmental agencies are of course aware of this problem, and many clearly care about getting the numbers right. The UK, for example, initially counted anyone who died at any time after a positive test, regardless of cause, as a death due to COVID-19. After restricting this time period to 28-days, they reduced their death toll by 12%. Multiple American states have also lowered (or raised) their tallies when appropriate. According to a statement from one California county that lowered its death totals,
It is important to accurately report deaths due to Covid-19 so that residents and health officials have a more precise understanding of the impact of the pandemic and response actions in our community. Using the older definition of Covid-19 deaths, a resident who had Covid-19 but died due to another cause, like a car accident this person would be included in the total number of reported COVID-19 deaths for Alameda County. Under the updated definition of COVID-19 deaths, this person would not be included in the total because COVID-19 was not a contributing factor in the death.
It’s good that governments care about reporting accurate data and are willing to lower their tallies when appropriate.
Though there’s no evidence the number is large, assuredly the COVID-19 death tallies include some individuals who contracted SARS-CoV-2 and died of a disease that would have killed them regardless of this infection. However, Dr. Ioannidis’s statement that “It’s very likely that many of them would have died anyhow, if not immediately within a very short period of time, because of these other causes of death that they had” doesn’t follow from this. Most frail 95-year-olds who are alive today will still be alive in one month. That’s how we get 96 and 97-year-olds. Most people with hypertension, diabetes, obesity, and hyperlipidemia won’t die in the next month. Though they shorten lifespans, they are considered chronic diseases precisely because people usually live with them for many years and decades. Moreover, when people with these conditions die of natural causes, their death certificates will almost always list multiple co-morbidities. How could they not? As Dr. Scott Braunstein said:
Any clinician who has had experience deciding on what to list as cause of death on a death certificate, as I have had to do for the past 15-plus years, understands that the diagnoses chosen involve a great deal of discretion and judgement. In most cases, there are multiple contributing diagnoses, and it is common practice to list more than one factor. Underlying diabetes or coronary artery disease are common diseases that contribute to mortality, even when the immediate trigger for death was pneumonia, influenza, or some other infectious process.
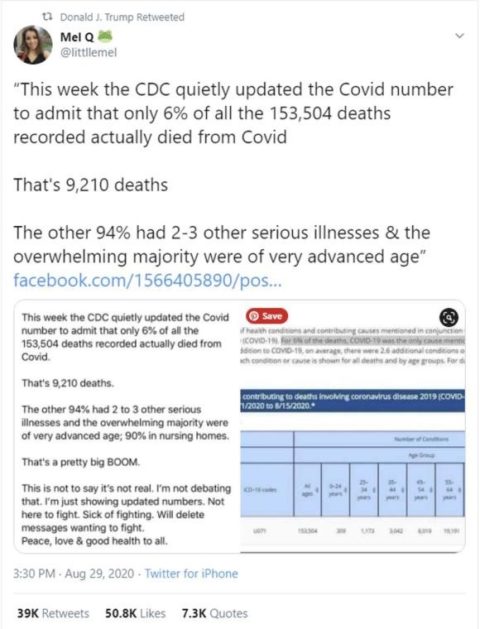
Mel Q: “94% had 2-3 other serious illnesses & the overwhelming majority were of advanced age”
Though Dr. Ioannidis may have been the first to claim that “It’s very likely that many of them would have died anyhow, if not immediately within a very short period of time, because of these other causes of death that they had”, he was definitely not the last to do so. With the help of a retweet from Donald Trump, a viral conspiracy emerged in the summer of 2020 when QAnon influencer Mel Q claimed the CDC had “quietly updated the Covid number to admit that only 6% of all the 153,504 deaths recorded actually died of Covid”, since “the other 94% had 2-3 other serious illnesses & the overwhelming majority were of advanced age”.
QAnon influencer Mel Q spreads conspiracies
Mel Q’s tweet sounds very familiar. One wonders if it was inspired by one Dr. Ioannidis’s prior statements. It is, after all, virtually identical to several of his remarks I shared previously. To pick just one, he questioned the virus’s toll by saying:
Because for the data that we have more mature and detailed information, like the data from Italy that has already through the peak of their epidemic wave, we realize that 99% of people who die with this virus have other reasons as well to die. On average, they have close to three other reasons to die. On average they are 80 years old with other comorbidities, as we say, and there’s quite some debate on whether these people would have died anyhow, if not immediately, you know, perhaps in a few days or in a few weeks or a few months.
It’s remarkable to realize there’s a fundamental agreement between Drs. Ioannidis and QAnon influencer Mel Q about core issues this pandemic. Since most COVID-19 victims are elderly people with medical co-morbidities, both agree something besides the virus likely killed many of them or if the virus did kill them, it only shortened their lifespan by a few months at most.
Of course, undercounting deaths is a problem too and American states have added deaths to their tallies as well to try to address this problem. COVID-19 can kill patients after 28-days, and early in the pandemic doctors may have been reluctant to attribute a death to COVID-19 when people died without being tested for the virus. Undercounting deaths is likely a much more substantial problem than overcounting, as I will discuss.
Three areas of agreement: Some patients who are listed as having died of COVID-19 are categorized “without COVID-19 documented”
Second, Dr. Ioannidis is correct that some patients who are listed as having died of COVID-19 are categorized “without COVID-19 documented”. But this isn’t as a big a problem as it sounds. Though it soon became widely available in the US, early in the pandemic, testing was available for only a small fraction of patients. It was almost never available for people who died at home. It is still not widely available in many parts of the world. However, this does not necessarily mean doctors are wrong to categorize certain deaths as due COVID-19 without testing.
Like many viruses, SARS-CoV-2 produces a characteristic set of signs and symptoms. In the words of Dr. David Oliver, “Doctors treating patients with COVID-19 over the past 12 months recognise a very different clinical syndrome in the sickest patients and a tide of cases of a kind, severity, and clinical course that we have not seen before”. Indeed, this novelty is what allowed the heroic Chinese ophthalmologist Dr. Li Wenliang, who tragically died from the virus himself, to recognize a new disease in the first place.
Doctors are right to put COVID-19 as the cause of death when someone who lives where the virus is circulating, develops classic COVID-19 symptoms, and then dies while gasping for air. This is true even if that person was not tested for SARS-CoV-2, though of course confirming the diagnosis with a test is ideal. As the CDC stated in its death certificate guidelines, “Ideally, testing for COVID–19 should be conducted, but it is acceptable to report COVID–19 on a death certificate without this confirmation if the circumstances are compelling within a reasonable degree of certainty”.
The argument that a positive test is required to diagnosis COVID-19 implies that the disease cannot exist without the test, which would be nice if it were true. It’s the same logic employed by Donald Trump when he said, “Cases are up because we have the best testing in the world and we have the most testing”. Of course, people contracted and died of viruses before testing was invented and even before people knew what viruses were.
Three areas of agreement: Filling out death certificates can be “tricky” at times
Third, Dr. Ioannidis is right that filling out death certificates can be “tricky” at times, though the situation is not nearly as dire as depicted. To understand how death certificates work, let’s consider a woman with a brain tumor who has a seizure while driving and gets into a nasty car crash. She undergoes several surgeries and seems to be making a good recovery. However, she later develops a wound infection and dies. Did she die of the wound infection, the car crash, a seizure, or her brain tumor? Of course, all of these contributed to her demise. Death certificates account for this complexity, allowing clinicians to select several causes of death in an ordered manner. According to the CDC,
The cause-of-death section consists of two parts. Part I is for reporting a chain of events leading directly to death, with the immediate cause of death (the final disease, injury, or complication directly causing death) on Line a and the underlying cause of death (the disease or injury that initiated the chain of morbid events that led directly and inevitably to death) on the lowest used line. Part II is for reporting all other significant diseases, conditions, or injuries that contributed to death but which did not result in the underlying cause of death given in Part I. The cause-of-death information should be YOUR best medical OPINION…When a number of conditions resulted in death, the physician should choose the single sequence that, in his or her opinion, best describes the process leading to death.
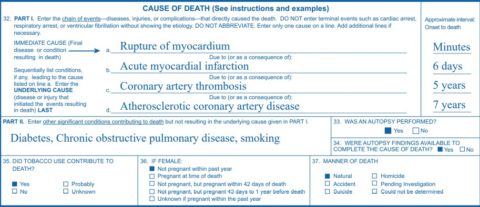
A sample death certificate
Additionally, the CDC put out specific guidelines to help standardize death certificates during this pandemic, and as stated previously, multiple states have lowered their death tallies in accordance with these guidelines.
Doctors who actually fill out death certificates are much less troubled by this process than Dr. Ioannidis. As Dr. Zubin Damania (AKA ZDoggMD) said:
Any medical professional who fills out death certificates understands how it’s done. You list the main cause of death and then anything that contributes. So the certificate can have multiple things on it. You can have things that were preexisting like diabetes, high blood pressure, obesity, and then you can have the main disease, like COVID-19, and then things that led to the main visit, like respiratory failure, respiratory arrest, cardiac arrest, heart failure, adult respiratory distress syndrome, and you list all those things on the document.
It’s true though that there’s a degree of subjectivity when determining the chain of events leading directly to death. Two doctors may not report the same chain of events in the exact same way for every death certificate. Though Part II of the death certificate allows doctors to distinguish between a patient with terminal cancer who happens to test positive for SARS-CoV-2 and those who actually die of COVID-19, some errors have certainly been made. But this doesn’t mean that doctors are largely unable to determine who dies from COVID-19 and who dies with incidental SARS-CoV-2 infection as Dr. Ioannidis suggested.
Doctors were “just going crazy, and intubating people who did not have to be intubated”
Dr. Ioannidis’s statement that “death certificates often are pretty inaccurate” and that those who fill them out “may subconsciously or unconsciously prefer to list COVID-19 as a major cause of death in the certificate, even though it may be less significant contributor if not an innocent bystander in some cases” is a shocking, unsupported indictment of the basic competence of doctors around the world. Dr. Ioannidis believes that when their patients died, doctors were often not capable or sophisticated enough to know what really killed them. He feels doctors were unable to reliably distinguish between someone who died from COVID-19 and someone who was on their deathbed for another reason when they happened to test positive for SARS-CoV-2.
I suspect Dr. Ioannidis would say he has the upmost respect for doctors working in the trenches with COVID-19 patients and would likely vigorously deny any intention to attack their competence, but it’s not really possible to read his statement any other way. Unfortunately, this was not his sole salvo on frontline doctors. On a podcast (at 1:37:25), Dr. Ioannidis said, “There is an effect of what we did, mostly wrong, in the first wave”. To be clear, Dr. Ioannidis is not referring to himself when he said, “what we did, mostly wrong,” but rather to doctors who treated patients with a completely new virus early in the pandemic. Had he been referring to himself, I suspect he would not have laughed when he said this. He then said that “a lot of lives” were lost at that time in part because of doctors “not knowing how to use mechanical ventilation, just going crazy, and intubating people who did not have to be intubated”. Dr. Ioannidis did not provide any evidence for this claim, nor did the podcast host, who agreed with him. Neither this charge, nor his claim about death certificates is likely to be true, as I will discuss.
People who worked on COVID-19 units have every right to feel legitimately proud of their work
New York’s COVID-19 surge was a painful, but inspiring time. We tried to keep the oldest doctors out of harm’s way, but almost everyone else was eager to help out. Pediatricians worked with seniors and gynecologists worked with men. Medical schools graduated students several months early so they could care for COVID-19 patients. I urge everyone to read about their experience. Medical students who were earlier in their training were properly shielded from patients. Instead, they reviewed patients’ charts and called families to keep them informed about their loved ones. The news was oftentimes not good. Other students helped make plastic face shields. Our city was saved by doctors and nurses (mostly nurses) who traveled from all around the country to help. I heard deep southern accents at the hospital that I normally hear only from tourists in Times Square. The city cheered for us every night at 7PM, even though many of us didn’t really feel we deserved it.
COVID-19 hit New York like a tsunami, one we could see coming a couple weeks before it arrived due to the experiences in Italy and Spain. I don’t know if it exists, but I had pre-traumatic stress disorder, as I was plagued by nightmares of mass death just before COVID-19 arrived. I started taking a medication to help me sleep for the first time in my life. It was just a terrifying time. We now know that PPE works very well. Working with COVID-19 patients was safer than eating in the workroom with colleagues. But we didn’t know that back then, and PPE was often in short supply. Early on, some healthcare workers had to improvise and use everyday items to try protect themselves. We all had to wear a single-use N95 mask for a week or longer. We of course worried about getting sick ourselves or bringing the virus home to our loved ones. The experience made many healthcare workers reconsider their careers. Consumed by fear and grief, some took their own lives. I know too many doctors who contracted COVID-19 to count. Some were really sick for weeks. Over 3,600 healthcare workers died in the US. I knew three of them. Some of them were very young.
Additionally, COVID-19 was a brand-new disease, and we had no idea how to treat it. As an attending doctor I had to make some really tough decisions, but even during a pandemic, much of the work was done at a computer or delegated to younger doctors. Residents, interns, nurses, EMTs, respiratory techs, pharmacists, custodial, kitchen, and maintenance staff were the true heroes of the pandemic. They kept the hospital running and the patients well-cared for day and night for months at a time. There were people whose sole job was to bring dead bodies to the overflowing morgue. I can’t imagine how they managed to do this every day. Our hospital director kept everyone calm with his cool demeanor during daily briefings, even when he was informing us that a dozen more critically ill patients were on their way. The administration and countless others toiled behind the scenes to ensure the hospital was properly staffed and we had the PPE we needed. I’m certain we saved many lives, though we all wish we could have done more.
The countless brave people who worked on COVID-19 units have every right to feel legitimately proud of their work.
Extraordinary claims require extraordinary evidence, part 2
Of course, doctors aren’t perfect, and sometimes we need to hear tough feedback, even during a pandemic in which we are “healthcare heroes”. Dr. Ioannidis’s meta-analysis of hydroxychloroquine trials is an example of such feedback, even if it doesn’t support his claim that the medication killed 100,000 people globally as it says nothing about how many people received the medication. I’m glad that I refused to give this, or other unproven therapies, to my COVID-19 patients outside of a clinical trial. In fact, the only demand I, a neurologist treating a respiratory virus, made upon agreeing to take over a COVID-19 team was that none of my patients would receive unproven medications. Understandably though, many desperate doctors wanted to do something for their patients even if it lacked evidence, a defensible strategy only for those patients who were certainly going to die otherwise. Unfortunately, it is certain that some of these “heroic” efforts seriously harmed and even killed some patients. Evidence-based criticisms must be welcomed in the spirit of preventing similar errors in the future.
In contrast, criticisms without evidence, and especially those that are contrary to the evidence, must be exposed and rejected. This applies to Dr. Ioannidis’s charges that doctors killed many patients through inappropriate intubations and then filled out their death certificates incorrectly. Not only is there no evidence that doctors were “just going crazy” intubating patients, leading to their demise, in fact, a meta-analysis of 12 studies found “The synthesized evidence of almost 9000 patients suggests that timing of intubation may have no effect on mortality and morbidity of critically ill patients with COVID-19”. This suggests that early intubation of critically ill COVID-19 patients may not be necessary, but it doesn’t kill them. This meta-analysis was published after Dr. Ioannidis made his accusation, but all 12 studies it reviewed were published beforehand. Not only is there no evidence that doctors “subconsciously or unconsciously” preferred to list COVID-19 on death certificates, in fact, death certificates have proven to be very reliable this pandemic, as I discuss below. Again, extraordinary claims require extraordinary evidence. This is especially true for an influential scientist with a large megaphone making substantial allegations in public against frontline doctors in the middle of a pandemic.
COVID-19 deaths are not drastically inflated: Studies of death certificates
Christopher Hitchens famously said, “What can be asserted without evidence can also be dismissed without evidence”. It would be perfectly legitimate to dismiss many of Dr. Ioannidis’s statements on these grounds alone. However, I will present two refutations to the claim that SARS-CoV-2 is an incidental infection in many COVID-19 deaths – studies of death certificates and common sense. Let’s start with studies of death certificates.
Studies of death certificates confirm the unsurprising news that most people who are said to have died of COVID-19 actually died of COVID-19. According to the CDC:
Among death certificates from calendar year 2020 listing COVID-19 and at least one other co-occurring diagnosis, the documentation is consistent with these deaths being attributable to COVID-19. Specifically, in 97% of 357,133 death certificates with COVID-19 and at least one other diagnosis, the documented chain-of-event and significant contributing conditions were consistent with those reported in clinical and epidemiologic studies to occur among patients with severe COVID-19–associated outcomes. Only 5.5% of death certificates had COVID-19 without any other conditions listed.
It’s good that the CDC was willing to investigate death certificates to ensure their accuracy, even if QAnon supporters misinterpreted the results. It’s good that 97% of death certificates of COVID-19 victims are “consistent with these deaths being attributable to COVID-19”. Dr. Ioannidis said, “We know that death certificates often are pretty inaccurate”. If he has evidence that death certificates have often been filled out inaccurately this pandemic, I have been unable to find it. Until he provides it, during this pandemic at least, we know that that death certificates often are pretty accurate.
COVID-19 deaths are not drastically inflated: Common sense
Now let’s look at the common sense refutation. Last year during the surge in New York City, every hospital in the city was overflowing with COVID-19 patients. Children’s hospitals cared for adult patients. Ambulances came from all over the country, and their sirens wailed constantly throughout the strangely quiet city streets. Field hospitals were set up in several places and a massive naval hospital, the USNS Comfort arrived, though it only treated 182 patients due to strict admission criteria. Every day, dozens of the sickest patients were transferred to Bellevue Hospital, where I worked, from other city hospitals that were overwhelmed with COVID-19 cases. Though we came very close, Bellevue never totally ran out of space, as many people died every day. Every fifteen minutes the overhead pager would summon the “airway team” to a different room. I would often arrive in the morning to learn that half of the people I left the evening before had died or been transferred to the ICU overnight.
The ICU itself was an eerie place. This is where I started out working, though truthfully I was only marginally more helpful than a medical student. Our incredible facilities staff managed to install ventilation in every room in a very short amount of time. IV poles were placed outside the rooms to minimize exposure to staff. Almost all the patients were Black or Hispanic. Some were Asian. Very few were White. Guards from the Department of Corrections kept watch over dying inmates. There were always two patients in a room meant for one. There were just bodies of motionless people, intubated, sedated, and alone. Some lived. Some died. I would occasionally gaze out a window to glimpse the abandoned, crumbling Renwick Smallpox Hospital on Roosevelt Island, reminding myself that humanity had defeated viruses before.
Overall, I saw more people die in a few weeks than I had in the past decade, if not my entire career. One of the first was a man who worked as a carpenter at Bellevue for several decades, though he retired before I arrived. As the city morgues became overwhelmed, massive, refrigerated trucks were parked behind my hospital to store the bodies. Overall, 135 such trucks were used in New York City. Even that was not enough. According to news reports, “Shelves were placed in the trailers, doubling their capacity, as funeral directors ran out of storage room. Cemeteries and crematories could not handle the load”. One hospital used a forklift to move all the dead bodies. Finding space to bury the bodies was difficult, a problem faced by many countries. As one nurse, Eileen Diaz, said, “It was just complete chaos. It was like a medical war zone”.
I saw plenty of middle-aged people die and several younger people die. The youngest person I saw die was only 23 years old. He was able to breathe, but was completely obtunded, unable to speak or move. Several days before his death, I made him suffer by placing a nasogastric tube so he could be fed. We didn’t know he would die, and of course he needed nutrition. I still think about that a lot. I wonder what kind of person he was and what his future might have held. His aunt said that he was a loner, and it makes me sad that few people might have mourned his passing. He wasn’t in touch with his mother who had substance abuse issues, I was told. I promised myself to remember his name and I think about him from time to time. I’ve often wondered if I should call his aunt to see how she is doing and tell her that I still remember her nephew. She was an EMT and knew she gave him the virus. I hope she doesn’t blame herself.
While most victims had chronic, underlying conditions, it’s ludicrous to expect a large percentage of them would have died “immediately” or “perhaps in a few days or in a few weeks or a few months” had they not contracted COVID-19, as Dr. Ioannidis suggested. The virus was not an “innocent bystander” for these patients. They were not “already dying from something else” when we just happened “to find a PCR positive test for SARS-CoV-2 in a nasal swab”. The virus did not just give a “final kick” to people who were days or weeks away from dying of other causes.
When Dr. Ioannidis said that “you’re not even sure that SARS-CoV-2 really did contribute to their death substantially”, he could only have been referring to the fortunate people who experienced COVID-19 exclusively as an online event. Clinicians who spent substantial time working with hospitalized COVID-19 patients were all pretty sure what killed our patients – it was the virus. He also said, “It’s very hard to say how many of these people would have died anyhow and how much is the direct contribution of the virus”. He’s wrong. It was very easy to say how many of our patients would have “died anyhow”. Virtually none of them would have “died anyhow”. It was also very easy to say “how much is the direct contribution of the virus”. The virus was directly responsible for killing our patients. He also wrong when he said, “the number of person-years lost, how many years of life are being lost, is much less than even what the number of deaths would suggest”. Doctors who actually work with COVID-19 patients know many victims have their lives shorted by several decades. If you doubt this, ask one of these doctors. They will all say the same thing.
Research supports what they will tell you. One study from April 2021 calculated the virus had stolen 3.9 million years of life away from Americans, and the average COVID-19 victim lost over 9 years of life. Another study from October 2020 calculated that the virus had stolen 2.5 million years of potential life in the US. Just under half of these years were taken from people younger than 65 years. As the paper’s author Dr. Stephen J. Elledge said, “COVID-19 has wiped out millions of years of productive, active, and happy existence”. They were not all 95-year-olds with advanced cancer only days away from dying when they happened to test positive for SARS-CoV-2. In the words of Dr. Utibe Essien, “These are everyday people who are dying. They’re losing time with their kids, their grandkids, their opportunities to build their futures”.
Deaths spiked not just in hospitals, but in homes as well. According to news reports, “About 120 morgue workers and soldiers from the U.S. Army, the National Guard and the Air National Guard are working in shifts around the clock, driving rented vans around the city to pick up the bodies of as many as 280 people a day who have died at home and have probably not been part of the official death count”. According to the New York City Fire Department, “In the first five days of April, 1,125 people were pronounced dead in their homes or on the street in New York City, more than eight times the deaths recorded during the same period in 2019”. While not all of these were COVID-19 victims, many certainly were. None of them died because of doctors “just going crazy” intubating them. Quite possibly some could have lived had they made it to the hospital.

Bellevue Hospital should be proud of discharging nearly 2,000 COVID-19 patients
Indeed, many more patients were discharged home, thanks in part to the care they received. The condition of these survivors varied widely. Some left without symptoms and were seemingly back to normal. Some left in the middle of their disease course, as they had somewhere to go or simply didn’t want to be in the hospital. We tried desperately to make them stay, especially if they were homeless, but we couldn’t force them to do anything. I wonder how many of these patients were willing and able to isolate themselves. Some older patients had been extremely delirious, paranoid and hallucinating. Many did not speak English and it was a struggle to communicate with them. It must have been terrifying when we approached with our faces hidden by masks and goggles. Many survivors had been intubated and bedbound for months. They survived but were quite debilitated, barely able to move after experiencing prolonged immobility. With the focus on deaths, these survivors often get overlooked. I wonder how they are doing now.
While the surge in New York City was earlier and perhaps more intense than elsewhere, our experience wasn’t particularly unique. When the refrigerated trucks left New York, they were needed in other states. Children’s hospitals elsewhere opened their doors to adults. We all remember headlines such as “Coronavirus Kills 70 Veterans at Massachusetts Care Home”. Spain had to convert an ice rink into a morgue, and coffins piled up in Italian churches. In India, “Hundreds of corpses have been found floating in the (Ganges) river or buried in the sand of its banks”. Scenes of innumerable funeral pyres there are unforgettable. In Ecuador, bodies were simply left in the street. Variations of these scenes played out all over the world.
With this in mind, we can now revisit Dr. Ioannidis’s claim that “it’s very likely that many of them would have died anyhow, if not immediately within a very short period of time, because of these other causes of death that they had”. There are not normally refrigerated trucks behind my hospital to store dead bodies – indeed they are gone now. Pediatricians don’t normally treat seniors, and gynecologists don’t normally treat men. Medical schools don’t normally graduate students early to work on overflowing hospital wards. The overhead “airway team” pager doesn’t normally go off dozens of times per day at my hospital. Dozens of people don’t normally die in a single nursing home in the span of several days. The military is not normally needed to retrieve dead bodies from homes. It’s not normally a challenge to find space to bury dead bodies. Skating rinks in Spain and rivers in India are not normally full of dead bodies. Bodies aren’t normally left in the streets of Ecuador. Something abnormal happened. There’s only one conclusion; it’s very likely almost none of them would have died anyhow, if not immediately within a very short period of time, because of these other causes of death that they had.
Challenging questions arise
These horrific scenes raise challenging questions for some people. Having established that many more people died than usual, one must blame either the virus or the methods used to control it. If the virus was often just an “innocent bystander”, or if a meaningful number of people died “because of the disruption induced by lockdown,” then:
- Why did the deaths peak just three short weeks after the lockdown started in New York City?
- What was the exact mechanism of death for all these people?
- Why did the deceased all have nearly identical symptoms, radiographs, and lab values?
- Why did they die in such a similar manner?
- Why did people who were able to isolate rarely die?
- Why did the deaths decline precipitously as the lockdown dragged on, instead of rising further in New York City?
- Why did the deaths come in waves, as with previous pandemics?
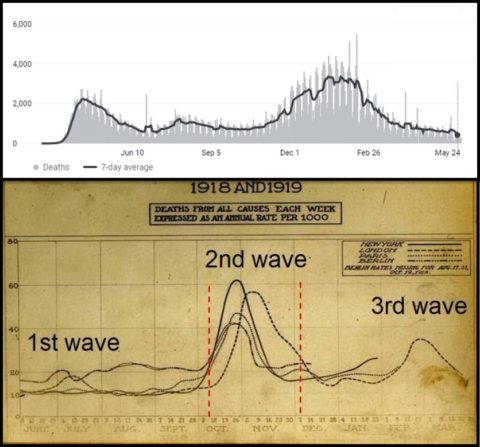
The COVID-19 and 1918 death waves. It’s almost as if a virus caused all these deaths
- Why have deaths fallen so dramatically, though primarily in vaccinated people or in areas with very high vaccine uptake?
- Why were places like New Zealand, which had “7 weeks of what was essentially a national stay-at-home order” spared these horrific scenes?
- If New York City had locked down in 2019 as part of a bizarre experiment, does anyone really think these nightmarish scenes of death would have occurred in a just three weeks? If so, what exactly would kill all these people in such a short period of time?
COVID-19 deaths might be underestimated
We’ll never know the true death toll of COVID-19. Importantly, undercounting deaths is likely a much more significant problem than overcounting deaths, even for the US. Undercounting was particularly a problem early in the pandemic when healthcare systems were overwhelmed, large numbers of people died at home, and testing was scarce or nonexistent. Doctors may have been reluctant to attribute deaths to COVID-19 under these circumstances. As one funeral home director said about the death certificates of likely COVID-19 victims, “I’ve seen it many times where the doctors will just leave it off. They’re exhausted, they’re busy, and they have a funeral director hounding them”. Looking at excess deaths compared to years past may give a better estimation of the true toll of COVID-19.
Undercounting deaths still remains a significant problem in much of the world. As Dr. Gideon Meyerowitz-Katz wrote,
We probably aren’t overcounting deaths on a global scale by very much. While there are almost certainly some deaths that are being inappropriately counted as being caused by Covid-19 that were really due to something else, the number is probably enormously outweighed by undercounting. It’s plausible that the true global toll of Covid-19 is 10% lower than we think, but it’s quite likely to be 50% higher or more. Given the data from some developing nations, it’s entirely possible that there are millions of uncounted Covid-19 deaths.
Scientists who express evidence-based views on COVID-19 should be heard, not demonized
Much has been written during this pandemic about whether or not nasty words directed toward Dr. Ioannidis have silenced important debate. Surely, some of the threats he says he and his family have received are horrifically inappropriate. We should all condemn this unequivocally.
But debating public policy requires some semblance of shared facts. You couldn’t debate me on the best way to capture the Loch Ness monster, since I reject the creature’s existence in the first place. Creating unwarranted doubt around basic facts similarly precludes meaningful debate about COVID-19. How can contentious issues such as masks, vaccines, and school closures be reasonably discussed when many people are falsely convinced the COVID-19 death toll is greatly inflated? They can’t.
Indeed, anti-mask protesters have harassed public officials and hapless store employees. Anti-vaxxers have shut down vaccination sites and even destroyed vaccines. Many public health officials have resigned after relentless harassment campaigns and threats. Dr. Anthony Fauci and his family need bodyguards for their protection. Though the widespread acceptance of COVID-19 myths has silenced debate much more than any mean tweet directed towards Dr. Ioannidis, many of those who vigorously opposed the supposed “silencing” of Dr. Ioannidis are themselves strangely silent about all of this.
Dr. Ioannidis has said how much he deplores this. I completely believe him. It also would all have happened if he had not said a word. Highly influential leaders of the anti-vaccine movement, such as Dr. Kelly Brogan have also cast doubt on the accuracy of death certificates and the overall toll of COVID-19. In one video she said:
There are other theories about what’s going on that have nothing to do with a virus spreading. That literally suggests, there is potentially no such thing as a coronavirus. There is a tremendous lack of vigilance around the declaration of cause of death in hospitals… ‘Cardiorespiratory collapse’ was the phrase I was encouraged and taught to put on a death certificate if we didn’t immediately know the cause of death.
She additionally posited that fear was killing people, not a virus. As a germ-theory denier, Dr. Brogan doesn’t believe viruses cause disease at all. She said the pandemic was part of a psychological operation to “link our passports with our vaccination records and the restriction of travel being the new normal” to establish “totalitarian governmental control not unlike the divide-and-conquer dehumanization agendas that preceded the Holocaust”. I am not making this up, the way she is making up how she was taught to improperly fill out death certificates. This article is quite a read. Dr. Brogan and other members of the so-called “Disinformation Dozen” have greatly undermined the response to COVID-19 by convincing large numbers of people the virus isn’t dangerous.
As with Mel Q, it is remarkable to realize there’s a fundamental agreement between Drs. Ioannidis and Brogan about core issues this pandemic. They both feel the virus’s toll “is much less than even what the number of deaths would suggest”, as Drs. Ioannidis put it, and death certificates that say otherwise cannot be trusted. As critic Eliza Wells said about one of these two doctors, in order to believe their “claim that numbers are vastly exaggerated you would have to accept that medical health professionals around the world are misreporting the number of deaths attributable to COVID-19. You would also have to believe that they are incompetent, manipulated or lying — perhaps all three”. Was Ms. Wells referring to Dr. Ioannidis or Dr. Brogan when she wrote this passage? It quite reasonably could be either of them, though the answer is Dr. Brogan. Notably, I was unable to find any examples of Dr. Brogan blaming doctors for killing their patients as a result of their “not knowing how to use mechanical ventilation”.
Twitter COVID-contrarians
Misinformation also abounds on Twitter, where Dr. Ioannidis does not have an account. There is a predictable group of COVID-contrarians who garner attention and followers through their “controversial hot takes”. They reflexively oppose the scientific consensus in predictable, trite ways. Being unique matters more to them than being right, it often seems. Their followers call them “brave” and “independent”. It must be very gratifying. I don’t get that feedback on Twitter. Several contrarians declared the pandemic over in the US several months ago. They then inexplicably continue to tweet and write about an event they feel has ended. Some contrarians will say they are 100% pro-vaccine and then provide specious arguments for why they feel adolescents should not be vaccinated. Others push outright vaccine misinformation. The border between these two isn’t always clear.
Twitter has banned the accounts of some of the worst offenders, though many others remain. To the contrarians, Dr. Ioannidis is a brave truth-teller who is rarely if ever wrong. Dr. Ioannidis’s mathematically implausible claims (discussed below) are spun as someone who just thinks “differently” about trade-offs. Despite the extensive quotations I’ve shared, contrarians will likely deny he ever minimized the virus. The fact that he called the virus a “serious problem” will likely be used to excuse everything else he said. They will claim that he was “just asking questions,” a rhetorical trick known as JAQing off. They’ll point to others who overestimated COVID-19, which of course, has no relevance to Dr. Ioannidis’s underestimation of the disease.
This essay will likely upset contrarians, though my criticisms of Dr. Ioannidis are much milder than those he causally lobbed against doctors who treated patients during the deluge of the first wave. Hopefully my criticisms have the advantage of being backed by evidence. Contrarians will say I’m guilty of “tribal politics” and “groupthink,” which are schoolyard taunts, not actual arguments. They will likely substitute tone-policing for meaningful argument. Predictably someone reading this article will latch on to a phrase they feel is inappropriate or they will complain about the overall “nasty tone”, rather than deal with the substance of my criticisms. Notably, few of these contrarians actually worked with COVID-19 patients. Most are utterly divorced from the consequences of their words. It all seems to be a game to them, a way to build their brand.
“The evidence we had early in the pandemic was utterly unreliable”
Sadly, it’s not a game. There are real-world consequences when influential scientists minimize the pandemic, undermining the credibility of doctors and public health officials without compelling evidence. To better understand this, let’s examine Dr. Ioannidis’s appearance on a Fox News program hosted by right-wing firebrand Mark Levin from April 20th, 2020.
At the start of the interview, Dr. Ioannidis tells Mr. Levin that, “the evidence we had early in the pandemic was utterly unreliable”. Mathematical models of 2.5 million Americans dying, are called “completely off, it is just an astronomical error”. I am not certain, but can only imagine this was a reference to epidemiologist Neil Ferguson whose model predicted COVID-19 would kill 2.2 million Americans. Importantly, this number applied only “in the (unlikely) absence of any control measures or spontaneous changes in individual behaviour”, something Dr. Ioannidis did not mention. By CDC estimates, about 34% of the US has had COVID-19 and about 600,000 people have died. It’s entirely plausible that close to 2 million Americans would have died had the virus been allowed to rip throughout the population unchecked, completely overwhelming medical systems. In retrospect, Professor Ferguson’s model doesn’t seem like an “astronomical error” to me.
Having told the viewer to distrust everything they’ve heard about COVID-19 so far, Dr. Ioannidis then claimed to have newer and better data. This data was incredibly good news. It was what we all wanted to hear: COVID-19 isn’t that bad. According to Dr. Ioannidis, the risk of dying from COVID-19 is high for elderly people, especially those in nursing homes, and for those with serious underlying diseases, but “most of the population has minimal risk, in the range of dying while you’re driving from home to work and back”. He said the infection fatality rate is “probably in the range of 1 in a 1,000”. Mr. Levin repeats the good news by saying, “You say one in a thousand. You’re saying well under 1%, is that one-tenth of 1% of the population that actually has the virus will pass away as a result of the virus, or in connection to the virus”. Dr. Ioannidis responds in a now familiar way by saying “This is as open question…99% of people (in Italy) who die with this virus have other reasons as well to die”.
Sadly, more than 1 in a 1,000 people who contract COVID-19 will die from it. In fact, by some estimates, the 1 in a 1,000-fatality rate is accurate only for 25-year-olds. Given the current death toll in the US, a fatality rate of 1 in 1,000 would require 600 million total infections, though only 328 million people live here.
Elsewhere, Dr. Ioannidis claimed that “For people younger than 45, the infection fatality rate is almost 0%”. In fact, approximately 25,000 Americans younger than age 45-years have died of COVID-19 thus far. This includes at least 452 children, perhaps more. One study, spanning the first 5 months of the pandemic, found 11,899 more Americans ages 25-44 years died than expected, with 4,535 (38%) of the deaths due to COVID-19. Many of the other excess deaths were likely due to “an insufficient amount of COVID-19 detection and reporting in this age group”. The death toll for children and young people has been worse outside the US. As a healthy 45-year-old, I did not consider my pre-vaccine risk of dying from COVID-19 to be “almost 0%”.
In yet another interview he said, “For someone who is less than 65 and has no underlying diseases, the risk is completely negligible…it seems that these deaths are extremely exceptional”. Different people have different definitions of a risk that is “completely negligible”. To me, my risk of being swallowed by a whale is “completely negligible”. In contrast, healthy people younger than 65 die of COVID-19 every day. The fact that these tragedies make up a relatively small percentage of the total COVID-19 deaths can obscure the fact that the total number is not trivial, especially considering the number of years of life lost when a young person dies. Younger people have been especially affected in less resource-rich parts of the world. According to Dr. Carissa F. Etienne, “In Brazil, mortality rates have doubled among those younger than 39, quadrupled among those in their 40s and tripled for those in their 50s between December 2020 and March 2021”. Young, healthy people also suffered greatly during India’s still-ongoing wave.
Dr. Ioannidis also said on Fox News that “the vast majority” of people “don’t even realize that they have been infected, they are asymptomatic, they have no symptoms, or they have very mild symptoms that they would not even bother to do anything about”. In fact, one meta-analysis found that only 16% of cases are asymptomatic. Another found that only 20% of cases are asymptomatic. Moreover, studies of asymptomatic individuals found that about 80% of them eventually develop symptoms. Many are best labeled as pre-symptomatic. Clearly, the vast majority of people feel sick and do realize they have been infected.
10 Million infections people in a city with 8.3 million people?
I recognize most of the statements I have quoted are from relatively early in the pandemic, though several are from well after the pandemic’s first wave. As late as June 27th, 2020 Dr. Ioannidis claimed that deaths in the US and Europe were “more likely to be overcounted” and warning that “we need to be careful to dissociate deaths from COVID-19 versus deaths that happened because of the disruption induced by lockdown”. I also recognize it is not entirely fair to judge comments from the spring of 2020 with knowledge from the spring of 2021, as some now retroactively judge doctors who worked during the pandemic’s first wave. However, even at the time he made them, many of Dr. Ioannidis’s claims were mathematically implausible or downright impossible. New York City had already recorded over 10,000 COVID-19 deaths the week before he gave the Fox News interview, though Dr. Ioannidis likely did not accept this number as is included 3,700 people who presumably died of the virus without having been tested for it. If 10,000 people had already died and if only 1 in a 1,000 people died overall, as he claimed, this would require 10 million New Yorkers to have been infected, when only 8.3 million people live there.
Even excluding the 3,700 deaths who weren’t tested for the virus, a death rate of 1 in a 1,000 requires 75% of New York City to have been infected by mid-April 2020. Dr. Ioannidis’s may very well have thought this many New Yorkers had been infected given his belief that the vast majority of people have no or minimal symptoms. Currently, over 33,330 people have died in New York City from COVID-19. Dr. Ioannidis’s death rate of 1 in a 1,000 requires 33 million infections in New York City, which is four times its population and equal to the populations of New York State, Massachusetts, and New Jersey combined. This is not an isolated incident. Several times during the pandemic Dr. Ioannidis has calculated fatality rates that require more people to be infected in a given area than actually live in that area, assuming one accepts the death tolls as accurate of course.
What “really caused” 2.6 million COVID-19 deaths?
Dr. Ioannidis was not the only smart person to underestimate COVID-19 initially. There is no shame in having done this. There was a lot we didn’t know early in the pandemic, and many statements from that time look awful a year later. I, for example, tweeted out a study in March 2020 casting doubt on the benefits of masks. Though my “audience” is a fraction that of Dr. Ioannidis, this was a mistake, one of many I’ve made. I acknowledged my mistake, which wasn’t hard to do. Many others have since acknowledged their errors, and I admire them for this. Infectious-disease expert Dr. Paul Offit, for example, predicted on March 2nd, 2020 that COVID-19 would cause less than “one-tenth of the damage that influenza causes every year in the United States”. He later acknowledged his error saying, “If you’re going to be wrong, be wrong in front of millions of people. Make a complete ass of yourself”.
While Dr. Ioannidis readily admits error on behalf of frontline doctors, he has not returned to Fox News, or anywhere else, to correct these early statements as far as I know. The only time I have seen him admit error is when he revisited a prediction of his “that COVID-19 will result in fewer than 40,000 deaths this season in the USA”. However, even in this article, from August 25th, 2020, he cited “additional contributing reasons” as to why his prediction was off. According to Dr. Ioannidis, the real problem was how COVID-19 deaths came to be counted. Note the use of scare quotes in his explanation below:
When I made that tentative quote, I had not considered the impact of the new case definition of COVID-19 and of COVID-19 becoming a notifiable disease despite being aware of the Italian experience where almost all counted “COVID-19 deaths” also had other concomitant causes of death/comorbidities. “COVID-19 death” now includes not only “deaths by COVID-19″ and” deaths with COVID-19″, but even deaths “without COVID-19 documented”.
To be fair, more recently Dr. Ioannidis appears to have quietly, but dramatically, shifted his position and now seemingly accepts that millions of people have actually died from the virus, but with some key caveats. In a talk from March 2021, he listed the following reasons as “what really caused” 2.6 million COVID-19 deaths:
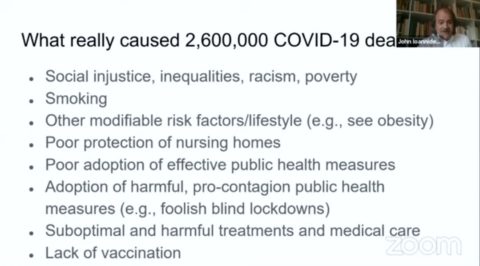
What “really caused” 2.6 million COVID-19 deaths
From doctors to politicians who supported “foolish blind lockdowns” to nursing home directors to COVID-19 victims themselves, Dr. Ioannidis clearly feels there’s a lot of blame to go around. Almost everyone is to blame it seems, except influential scientists who repeatedly minimized a deadly virus on widely watched outlets such as Fox News.
“THE U.S. DID NOT SURPASS 200,000 COVID-19 DEATHS”
However, influential scientists minimizing a deadly virus in public forums likely had an effect, one that makes previously perplexing behavior quite understandable. Anti-mask protesters really believed warnings about COVID-19 were “completely off, just an astronomical error”. Those who harassed public health officials really believed the chance of dying was “completely negligible” or “almost 0%” for everyone but grandma. Those who mocked social distancing guidelines really believed the “vast majority” of people “don’t even realize that they have been infected”. Anti-vaxxers really believe “death certificates often are pretty inaccurate”. And why wouldn’t they really believe these things? They heard it all from a highly-respected scientist, from a highly-respected university, who spoke with great conviction as he told them just what they wanted to hear. Indeed, Dr. Ioannidis’s interviewer on Fox News, Mr. Levin, would later promote Mel G’s conspiracy that COVID-19 deaths are inflated by tweeting, “THE U.S. DID NOT SURPASS 200,000 COVID-19 DEATHS”. This is how debate is silenced.
Unfortunately, false beliefs travel around the world with the click of a button, and the US has become a main exporter of these myths. According to one survey:
Among the most widely believed Covid conspiracies is that the death rate of the virus, which according to the Johns Hopkins University tracker has so far killed nearly 1.1 million people worldwide, has been “deliberately and greatly exaggerated”. Nearly 60% of respondents in Nigeria said this was definitely or probably true, along with more than 40% in Greece, South Africa, Poland and Mexico. About 38% of Americans, 36% of Hungarians, 30% of Italians and 28% of Germans felt the same.
The widespread acceptance of this belief will likely be a huge barrier to controlling the virus. To again quote Dr. David Oliver, “Every time we see or hear such mistruths we need to combat them and call them out. They are used to play down the seriousness and consequences of covid-19 and undermine health protection efforts”. I agree.
What exactly did the virus do to all these people?
Dr. Ioannidis said, “at some point we need to go back and check very carefully and try to understand what exactly did the virus do to all these people”. We can begin doing that now. Around the world, the virus has killed nearly 4 million people, likely many millions more, and sickened many hundreds of millions of people. In the US, the virus has killed 600,000 people, hospitalized 5.6 million, and sickened over 100 million more according to CDC estimates. Along with the Civil War and the 1918 epidemic, COVID-19 is one of the top three greatest mass casualty events in American history. Some survivors have been severely debilitated. We will be learning about the potential long-term consequences of COVID-19 for years. It’s not over yet.
Though access is still a problem for some people, overall, the vaccine roll-out in the US greatly exceeded my expectations. I never imagined that very safe and very effective vaccines would be freely and widely available for almost every American over 12-years-old well before the summer. Yet, many people have resisted. Many states have resorted to offering all sorts of incentives to convince people to get vaccinated. In 24 states, 40% or less of the population is fully vaccinated. I suspect Fox News is very popular in these states. Predictably, COVID-19 continues to sicken people in these areas. According to a New York Times database, in parts of Tennessee, “where only 20 percent of people are fully vaccinated, there has been an almost 700 percent increase in hospitalizations for Covid-19 over the past two weeks”.
Doctors and scientists have an obligation to choose their words very carefully when engaging with the public about a deadly virus and to openly correct the errors we all will inevitably make. It bears repeating; there are real-world consequences of promoting the idea that many people died with the virus, not from the virus. When an American dies of COVID-19 today – and hundreds are still dying daily – it is probable the decedent passed up an opportunity to be vaccinated.
Perhaps this person heard the threat from COVID-19 was greatly exaggerated. Perhaps this person was told doctors falsely hyped the threat or even killed patients through their “crazy,” inappropriate intubations. As such, these doctors couldn’t be trusted when they suggested vaccination or warned against quack cures. I hear versions of this frequently with my patients. Astonishingly, according to one article about an overwhelmed hospital in Canada, staff “are routinely hearing from sick and unvaccinated patients who believe the pandemic is a hoax — some remaining defiant even on the brink of death”. What is the source of these beliefs, for which people are willing to sacrifice their lives? Likely the source is people like Ted Nugent, Mel Q, and Dr. Kelly Brogan.
All of this makes me sadder than you can possibly imagine.