{kind=link}

Patient discussing treatment options with a pharmacist.
I’m a health professional, but sometimes a patient as well. And like most patients, I generally don’t want health decisions being made without my input. Yes, I want the best medical information, and the advice of medical professionals, but ultimately I want to make my own decisions about my care. That’s the norm in health care today, but relatively new in the history of medicine.
Medical paternalism, where patient preferences are secondary (or even ignored), is disappearing. Even informed consent, where patients are given information on risks and benefits, doesn’t adequately describe the drive towards a two-way exchange, with an empowered, engaged patient. Today the goal is shared decision making, which describes a mutual decision that is informed by a health professional’s medical knowledge and advice, but also incorporates a patient’s own preferences and wishes. Truly shared decision-making includes an explicit consideration of a treatment’s expected benefits and potential harms, yet reflects patient values.
Screening is a textbook example of why shared decision-making should be our goal. Given the benefits of a disease screening program may be modest, and not without harms, understanding and incorporating individual preference is essential. Some may value the small but incremental benefits of screening, and choose to be screened despite the risks of false positives, investigations, and possible overtreatment. Given the exact same circumstances, another individual may opt to forgo screening, making a different, yet equally acceptable decision. While there are some health interventions for which the benefits are unequivocal, and others for which the harms are just as clear, most health treatments (and interventions like screening) have both benefits and potential harms that must be carefully assessed within the context of patient preferences. Research published earlier this year has identified a significant barrier to truly effective shared decision-making and risk assessment: Across a wide range of interventions, we routinely overestimate the benefits of health treatments, and underestimate their risks.
There’s extensive research to show that patients want to be engaged and informed in health-care decision-making. Critical to this approach is an honest consideration of the scientific evidence. One of the important benefits of this blog has been to highlight the risks of poor health decisions when treatment considerations fail to consider plausibility, and instead rely on other forms of evidence. High-quality scientific evidence is the best tool we have to evaluate new treatments and determine their risks and benefits. However, that evidence must be informed by a consideration of basic scientific principles, and the overall scientific evidence established on a topic. For example, there is no persuasive evidence that alternative medicine treatments like acupuncture or homeopathy give any objective medical benefits. Yes, you can find individual clinical trials that may be statistically significant. But the totality of the evidence, when considered in the context of what we know to be a fact in fields like physics, biochemistry and other disciplines, makes it far more likely that positive effects seen in any single trial are due to bias, poor design, or statistical noise. Homeopathy and acupuncture have “effects” that, when closely scrutinized, are indistinguishable from placebo. Yet it’s unlikely that a potential recipient will have this fact disclosed to them by a provider. And without this information, consumers really can’t make a truly informed decision – and shared decision-making is effectively impossible.
It’s not just alternative medicine where effective shared decision-making can be difficult. Health professionals can also be at fault. As a pharmacy student I was taught to help patients make better self-care decisions, such as how to choose an appropriate cough and cold medication. I have probably assessed and recommended products to hundreds of patients over the years. I admit to facing some considerable cognitive dissonance later in my career, when I took a much closer and skeptical look at the science and determined that there’s little evidence to support the use of many of the ingredients in cough and cold products. Moreover, these products were best avoided in children, where the limited evidence that did exist suggested that the harms probably outweighed any expected benefits.
Opiates are another example where health professionals have created expectations of benefit without balancing the risks of harms. Over-prescribing climbed for years, based on inappropriate assumptions of benefit and risk. Today we are faced with a significant public health issue, with tremendous harms to patients.
If health professionals, whether they be pharmacists, physicians or surgeons, are overly optimistic about the treatments they are recommending, then their recommendations may contribute to overtreatment, or in the case of screening, overdiagnosis. And that can also compromise the goal of effective shared decision-making.
Ask your pharmacist if nothing is right for you. (HT @leachkathleen)
A patient’s own expectations can change treatment decisions, too. If patients believe a treatment or health intervention is beneficial, they are more likely to seek it out. This is well documented, from those that seek antibiotics for viral infections, or those that “ask their doctor” about the latest prescription drug (or homeopathic nostrum) that’s widely advertised and may not be as effective (or as safe) as advertised. And as has been well documented at this blog, the infamous Dr. Oz effect that creates an overnight demand for the latest “miracle” is regrettably not based in anything that resembles good science or medicine.
What appears to be the first paper to systematically examine patient assumptions and expectations has now been published. It lays out a significant challenge to optimal health-care decision-making.
The study, by Tammy C. Hoffmann and Chris Del Mar, was published earlier this year in JAMA Internal Medicine. It is a systematic review of other studies that have assessed patient expectations of benefits and/or harms of any treatment, test or screening test. They cast a very wide net in searching for evidence. They included studies where participants were asked to estimate the expected benefits/harms of a treatment, test, or screen. There had to be some form of quantification of the benefit in the questions asked.
For each identified study, the authors calculated the proportion that estimated accurately, and those that over/underestimated. The results were striking and consistent.
Of over 15,000 studies assessed, only 36 papers were eligible for inclusion. Study dates ranged from 1994 through 2013. Sixteen studies looked at treatments, and 20 looked at tests or screening.
Expectations of benefit
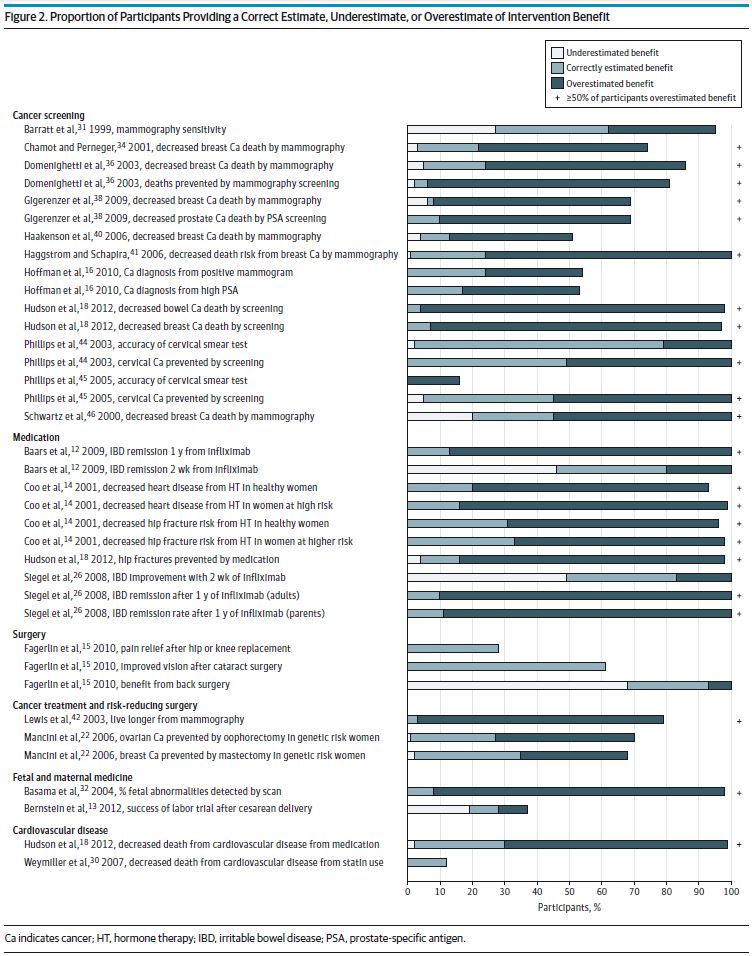
Figure 2 – patient expectations regarding intervention benefits (click to embiggen)
Of the 32 studies that assessed expectations about benefits, the authors compared the study outcomes with the “correct” estimates of benefit. The majority of participants overestimated benefits for treatments and interventions like cancer screening, the efficacy of infliximab for inflammatory bowel disease, and for cancer surgery. Only two studies found accurate estimates of risk, in studies of the expected benefits of cataract surgery and cervical test smear accuracy. In only one trial did participants underestimate benefit: surgery for low back pain (see figure 2, above).
Expectations of harm

Figure 3 – Patient expectations regarding treatment harms (click to embiggen)
In the 11 studies that examined expectations of harms, at least 50% of participants underestimated harms for 10 of 15 outcomes studied. These harms included the negative consequences of cancer screening, the side effects of different medications, and complications from surgery (see figure 3, above). Correct estimates of harm were noted for only two interventions: glasses after cataract surgery, and miscarriage risk from amniocentesis. Harm was overestimated for only one outcome, that of breast cancer risk due to hormone therapy.
Despite the diversity of studies included in this review, the overall findings are persuasive. In general, patients tend to overestimate benefits and underestimate the harms of treatments. This is an important signal to advocates of science-based medicine, suggesting that our continued advocacy in areas like the regulation of homeopathy are important. But beyond getting the science right, we need to work to find better strategies and tools to inform decision-making. Decision aids have been identified as one tool that may support both shared decision-making and an accurate assessment of risks and benefits. The Choosing Wisely campaign is another approach, designed to support dialogue between patients and providers with the goal of minimizing the use of low-value treatments and interventions.
Conclusion
Health care providers and patients alike want the best care. Treatment decisions need to be informed by accurate, science-based information. Health professionals need to not only be aware of the benefits and harms of the treatments that they recommend, they need to disclose them in an accurate and candid way. They also need to recognize that their own biases, positive or negative, may be inflating patient expectations about benefits and risks. There’s much more that can and must be done to improve how we collaboratively make health decisions.
Reference
Hoffmann TC, Del Mar C. “Patients’ Expectations of the Benefits and Harms of Treatments, Screening, and Tests: A Systematic Review .” JAMA Intern Med. 2015;175(2):274-286. doi:10.1001/jamainternmed.2014.6016. PMID 25531451.
Pharmacy photo from flickr user Si Morgan used under a CC licence.