
{kind=link}
I’m getting tired of writing about ivermectin as a “miracle cure” for COVID-19, just as in 2020 I got tired of writing about hydroxychloroquine as a miracle cure for COVID-19. Oddly enough, as high-quality evidence accumulated that hydroxychloroquine doesn’t work, it faded in importance such that by early 2021 it was no longer the preferred wonder drug among COVID-19 conspiracy theorists. Ivermectin rose to replace it, or, as Scott and I like to say, ivermectin became the new hydroxychloroquine.
As high-quality evidence accumulates that ivermectin doesn’t work, I keep wondering what will be the new ivermectin, but, for some reason, ivermectin seems to have “legs”. So far, it’s withstanding a far greater assault in terms of evidence and even demonstration of probable fraud in the largest randomized controlled clinical trials cited to support its use to treat COVID-19. Moreover, as has long been the case with quackery like acupuncture, as the evidence from RCTs show it not to be any better than placebo, similarly as negative RCTs accumulate and serious deficiencies and probable outright fraud invalidating the positive RCTs, advocates are increasingly citing lower quality observational studies as “proof” that ivermectin “works” against COVID-19. It’s reminding me very much of a much older topic that we’ve been writing about since the founding of this blog, acupuncture, so much so that I’m beginning to think that ivermectin is the acupuncture of COVID-19 treatments.
Because of this, I find myself saying, “Once more unto the breach.” The reason is that ivermectin advocates are back and they’re flogging two more studies as evidence that ivermectin is the cheap, highly effective, nontoxic treatment for COVID-19 that “they” don’t want you to know about, for example:
I’ll get to those studies in a moment. In the meantime, legislative efforts to bypass science and professional recommendations continue apace, as touted here on TrialSiteNews, one of the largest antivaccine and medical conspiracy theory websites out there right now:
The New Hampshire’s state House approved a bill making ivermectin available by a medical prescribers’ “standing order,” meaning pharmacists will be able to dispense the medication without individual prescriptions.
Narrowly approved
The Republican dominated House in Concord voted 183-159 to approve the bill.
Republicans had argued that the drug is already over the counter in several countries and had been used specifically for COVID-19.
According to the legislation, a pharmacist would be able to fill a request for the drug under a “standing order“.
Meanwhile, Jeffery Tucker, who founded the libertarian “free market” think tank, the Brownstone Institute as the “spiritual child of the Great Barrington Declaration” (which advocated in essence a do-nothing let ‘er rip” strategy for the COVID-19 plus a poorly defined strategy of “focused protection” for those vulnerable to severe disease or death) gloats that New Hampshire voted for “pharmaceutical freedom“:
The New Hampshire House of Representatives has voted to make Ivermectin available at any pharmacy that wants to distribute this drug even without a prescription. It will likely pass the Senate and become law.
It’s a hugely positive breakthrough for medical and pharmaceutical freedom. It’s only tragic that this was not the situation two years ago. The doctors the world over who have rallied behind this treatment believe that many lives might have been saved. If one state in the Northeast had at least made the option available, outcomes might have been very different.
The Epoch Times reports that “Similar bills are pending legislative approval in Oklahoma, Missouri, Indiana, Arizona, and Alaska.”
Magnificent! What’s key here is the concept of human choice.
The irony is very bitter: the vaccine mandates have been universal and people have lost careers for refusing or been rejected for participation in public life. People were forced to get shots of doubtful efficacy in most cases that many people did not want or because they did not see the need and feared their side effects.
Meanwhile, a drug they would have chosen to take was denied to them, again by force, and physicians who believed they were saving lives had their licenses taken away for using their professional discretion.
For a good part of last year, many people in the world could freely buy Ivermectin, a generic drug that at least 8 quality studies have shown to be an effective treatment for Covid-19. It has long been part of the alternative treatment protocol for Covid since it was first tried in early 2020, but never recommended by the FDA, CDC, or NIH. At some point, the CDC was tweeting denunciations of it, somehow with the implication that this treatment was distracting from the main push of vaccine fanaticism.
I quote Mr. Tucker because it’s important to remind you before I discuss the studies of how the promotion of ivermectin has so easily become part of the COVID-19 disinformation machine plus a much older phenomenon. That older phenomenon is one of which long-time readers are very aware, specifically how quacks and antivaxxers have long argued that people should be allowed to “choose” their quackery (or “choose” not to vaccinate their children), portraying such “choice” as “health freedom” while portraying those trying to hold medicine to a scientific standard of being, in essence, fascists and authoritarians trying to keep the “people” from the “cures”. There’s also a conspiracy theory at the heart of such appeals, namely that “they” are “covering up the evidence” and “they” don’t want you to know the “truth”. Such appeals have been very effective over the last decade, as I’ve pointed out that the main reason that the politics of vaccine resistance have shifted very much rightward is because of a longstanding campaign by antivaxxers to rebrand their antivaccine views as “health freedom” and “parental choice”, even co-opting the women’s health slogan “my body, my choice” in a highly cynical way.
That’s why it’s important to look at the whole conspiratorial package behind “COVID-19 resistance”, and not just the individual parts, such as antivaccine pseudoscience or resistance to masks and other nonpharmaceutical interventions (NPIs) to mitigate the spread of COVID=19. Indeed, Tucker explicitly makes this case for me. First, he mocks a CDC cartoon about how to identify health misinformation:
You are welcome to peruse the entire document, the main message of which is that the government is always correct, always knows the most science at the time, while front-line doctors with experience are very likely quacks, crazies, or ruthless profiteers.
Sometimes it seems like the people who produce such propaganda are forever attempting to live in the world of the movie Contagion, where every alternative treatment is a scam promoted by a corrupt “blogger” and where the CDC knows all. This cartoon is a smear in every way.
I perused the document. It’s actually quite reasonable and mild, perhaps even too much so. It warns people to look out for professional-looking websites that feature quote-mined quotes, cherry-picked statistics, deceptively edited videos, old images being recirculated as though they were recent, and misleading diagrams. It identifies several types of misinformation creators and spreaders, such as the disinformer, the casual sharer, the believer, the mischief maker, and others. It suggests the CDC as one of several sources to fact check claims against, urging people, “If you’re not sure, don’t share!” All of this is very reasonable; so I wonder why Tucker reacts so violently against this message and uses a straw man huge enough that, if set afire, it could be seen from space to mischaracterize the message. Actually, no I don’t.
Unsurprisingly, though, Tucker pivots to cry “Freedumb!”:
This battle is much larger than the legal status of Ivermectin. That’s just one symbol. What’s really at stake here is the idea of medical freedom itself. And freedom is a precondition for scientific inquiry and the search for the truth. It is also essential for public health. This is one of many lessons of the disastrously botched pandemic.
The decisions of the New Hampshire legislature to enshrine that freedom into law in this one instance represent a mighty tribute to the principle and a repudiation of the use of force in disease management.
That’s exactly what I’ve been saying, except that, unlike Tucker, I realize that ivermectin doesn’t work and vaccines do, while also understanding that denialists like him might portray what they are doing as a “medical freedom” and a “search for the truth,” but what they are really doing is spreading misinformation that doesn’t really much care for what is “true” or not, as long as it decreases the power of government.
On to ivermectin. Again.
Observational studies a-go-go
If there’s one principle that should help you to identify when a medical claim is probably nonsense, it’s that you should look at the quality of evidence cited by the proponents of that medical claim. That’s why I mentioned acupuncture. Here at SBM, we’ve long pointed out how, as higher quality evidence from randomized controlled clinical trials of acupuncture that use proper blinding and better controls (i.e., sham acupuncture needles, acupuncture at the “wrong” sites that aren’t acupuncture points, actual double blinding to experimental group), it’s become increasingly obvious that acupuncture is nothing more than a theatrical placebo with no therapeutic effects, acupuncture advocates have shifted to preferring “pragmatic” trials. As Steve Novella pointed out so long ago, such studies are nothing more than the “rebranding” of unblinded trials. Early in the process of investigating a new treatment, unblinded studies can be justified as hypothesis-generating studies, but they are generally not considered the final word. Similarly, nonrandomized observational studies can be justified for a similar reason, in order to test whether larger randomized studies are justifiable.
It’s true that so-called “pragmatic” studies are also unblinded, but their purpose is different. They are not so much hypothesis generating as “real world” testing. As I’ve pointed out, such studies are “putting the cart before the horse“. The reason is that pragmatic trials do have a specific use in medicine. They are designed to test the “real world efficacy” of an intervention outside the highly controlled auspices of controlled randomized clinical trials (RCTs). The assumption is thus that the medical treatment being tested has already been demonstrated to be efficacious in RCTs and that the pragmatic trial is going to see how much less efficacious the treatment is when, as always happens when a new treatment is released “into the wild”, so to speak, it’s applied to a larger, less defined population with less rigor in methodology and follow-up.
The situation with ivermectin is similar in that ivermectin advocates prefer lower-quality clinical evidence than RCTs, because, as has been discussed here a number of times, all the high quality RCTs for ivermectin to treat COVID-19 have been resoundingly negative thus far, and the positive RCTs cited have all been found to contain, at best, serious flaws that invalidate their results, or to have been likely outright fraudulent. It turns out that all the dubious meta-analyses promoted by ivermectin advocates also become negative if these studies are left out (as they should have been, given their poor quality). In brief, all the higher-quality RCTs that tested whether ivermectin works are, as is the case of the higher quality RCTs of acupuncture for pretty much any indication, negative. There’s a definite rule of thumb at work here for the two. The higher quality the study, the more likely it is to be negative. Just as acupuncture advocates cite low quality unblinded studies that might have been acceptable early in the process of investigation, ivermectin advocates now cite lower quality studies that aren’t RCTs, and that’s exactly what Kim Iversen cites above.
Two observational studies that show…nothing
So let’s take a look at the two studies that Ms. Iversen touted in the Tweet that I quoted above. I’ll remind you of them by citing the Tweets again:
The first cited study comes from Cureus and is titled “Ivermectin Prophylaxis Used for COVID-19: A Citywide, Prospective, Observational Study of 223,128 Subjects Using Propensity Score Matching“. Most of the investigators are from Brazil, but one name stands out: Pierre Kory, MD of Front Line COVID-19 Critical Care Alliance (FLCCC). I’m not sure why it’s making the rounds now, given that it was first published two months ago, but such is life on social media. Either that, or it’s been making the rounds since then, but I just never noticed. I suspect that part of the reason is that it started out as a preprint that made the rounds even earlier. Indeed, in January, the FLCCC was flogging it thusly:
Results of the world’s largest study of ivermectin in COVID have just been posted. Meticulously collected data from hundreds of thousands of patients find massive reductions in hospitalization & death. “Controversy” over. Join us tomorrow for discussion with study investigators https://t.co/BQt9fia44I
— Pierre Kory, MD MPA (@PierreKory) January 5, 2022
You might well recall that the FLCCC is a group of doctors who are not at all “frontline” doctors treating COVID-10 but, as I’ve suggested, are prolific spreaders of COVID-19 misinformation, including antivaccine misinformation and the promotion of ivermectin as a cure-all for COVID-19. Last fall, they were even caught running a telehealth prescription mill selling ivermectin and hydroxychloroquine prescriptions to anyone who had the cash.
But what about the study itself? You can see how it might impress someone like Ms. Iversen, given that it involved looking at 223,128 subjects. However, quantity doesn’t always trump quality, and one notes right away that this study is not a randomized controlled clinical trial, but rather an observational study:
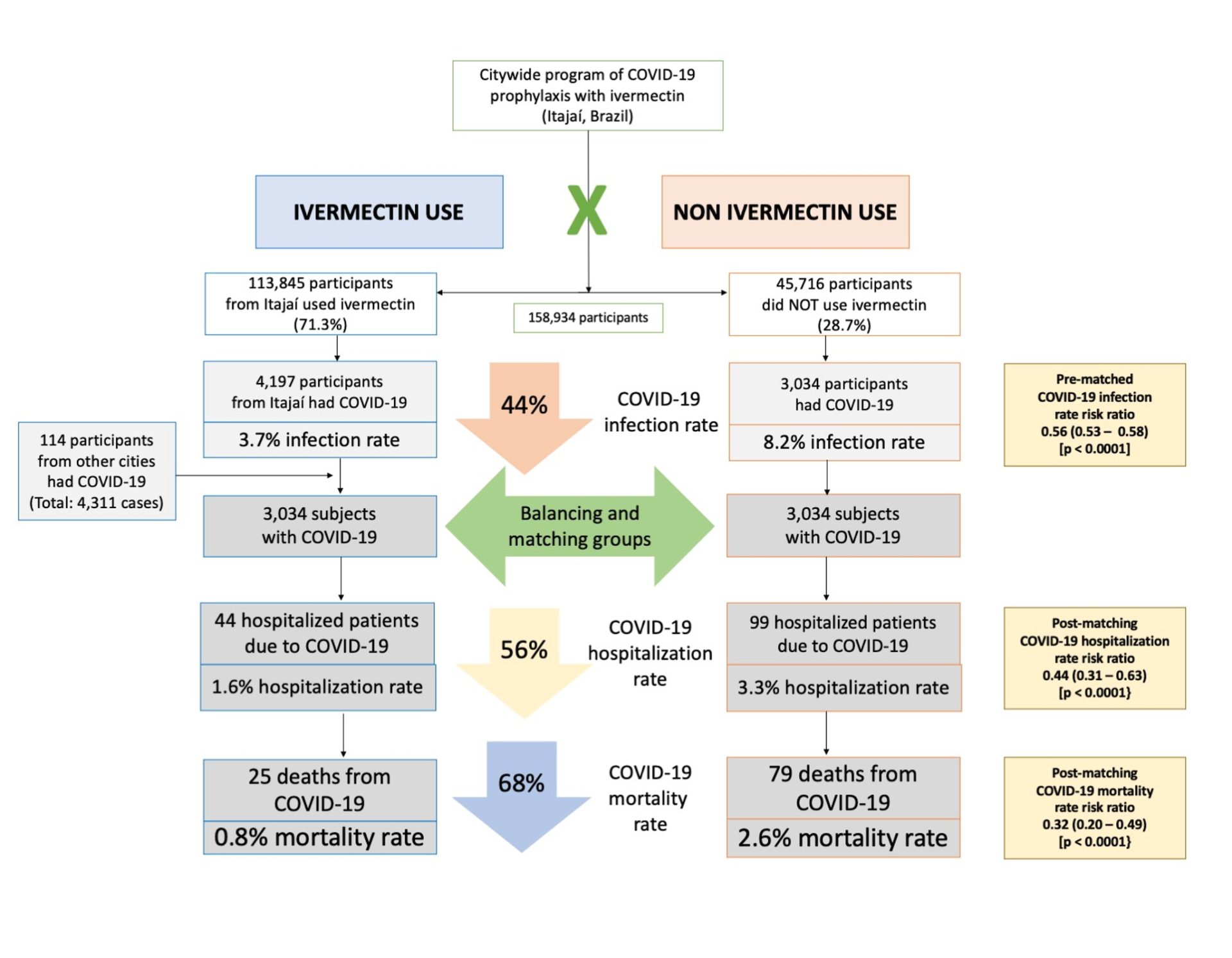
We analyzed data from a prospective, observational study of the citywide COVID-19 prevention with ivermectin program, which was conducted between July 2020 and December 2020 in Itajaí, Brazil. Study design, institutional review board approval, and analysis of registry data occurred after completion of the program. The program consisted of inviting the entire population of Itajaí to a medical visit to enroll in the program and to compile baseline, personal, demographic, and medical information. In the absence of contraindications, ivermectin was offered as an optional treatment to be taken for two consecutive days every 15 days at a dose of 0.2 mg/kg/day. In cases where a participating citizen of Itajaí became ill with COVID-19, they were recommended not to use ivermectin or any other medication in early outpatient treatment. Clinical outcomes of infection, hospitalization, and death were automatically reported and entered into the registry in real time. Study analysis consisted of comparing ivermectin users with non-users using cohorts of infected patients propensity score-matched by age, sex, and comorbidities. COVID-19 infection and mortality rates were analyzed with and without the use of propensity score matching (PSM).
Reading the paper, I honestly was a bit confused. Reading the abstract and the methods, it came across to me that ivermectin was offered as prophylaxis to everyone but if anyone became sick with COVID-19 it was not recommended, and, yes, that appears to be what was done:
Patients who presented signs or the diagnosis of COVID-19 before July 7, 2020, were excluded from the sample. Other exclusion criteria were contraindications to ivermectin and subjects below 18 years of age. The dose and frequency of ivermectin treatment was 0.2 mg/kg/day; i.e., giving one 6 mg tablet for every 30 kg for two consecutive days every 15 days.
During the study, subjects who were diagnosed with COVID-19 underwent a specific medical visit to assess COVID-19 clinical manifestations and severity. All subjects were recommended not to use ivermectin, nitazoxanide, hydroxychloroquine, spironolactone, or any other drug claimed to be effective against COVID-19. The city did not provide or support any specific pharmacological outpatient treatment for subjects infected with COVID-19.
This is, to say the least, a rather strange design. First, of all, when this study first started, people were asking the same question as I was: Why on earth would you recommend that patients take two doses, separated by a day, every two weeks?
Odd protocol or not, let’s see what the authors claim to have found:
Summarized thusly:
Of the 223,128 citizens of Itajaí considered for the study, a total of 159,561 subjects were included in the analysis: 113,845 (71.3%) regular ivermectin users and 45,716 (23.3%) non-users. Of these, 4,311 ivermectin users were infected, among which 4,197 were from the city of Itajaí (3.7% infection rate), and 3,034 non-users (from Itajaí) were infected (6.6% infection rate), with a 44% reduction in COVID-19 infection rate (risk ratio [RR], 0.56; 95% confidence interval (95% CI), 0.53-0.58; p < 0.0001). Using PSM, two cohorts of 3,034 subjects suffering from COVID-19 infection were compared. The regular use of ivermectin led to a 68% reduction in COVID-19 mortality (25 [0.8%] versus 79 [2.6%] among ivermectin non-users; RR, 0.32; 95% CI, 0.20-0.49; p < 0.0001). When adjusted for residual variables, reduction in mortality rate was 70% (RR, 0.30; 95% CI, 0.19-0.46; p < 0.0001). There was a 56% reduction in hospitalization rate (44 versus 99 hospitalizations among ivermectin users and non-users, respectively; RR, 0.44; 95% CI, 0.31-0.63; p < 0.0001). After adjustment for residual variables, reduction in hospitalization rate was 67% (RR, 0.33; 95% CI, 023-0.66; p < 0.0001).
Leading to the conclusion:
In this large PSM study, regular use of ivermectin as a prophylactic agent was associated with significantly reduced COVID-19 infection, hospitalization, and mortality rates.
If you believe this study, then, everyone should be taking ivermectin, two doses separated by a day, every two weeks. But should we believe it? There are a number of reasons not to, not the least of which is Kyle Sheldrick’s analysis:
And:
And:
In other words, data being presented…changed. Also, as pointed out by Sheldrick, the analysis claimed is pretty much impossible and hidden behind “data available upon request”:
In other words, not only is this study not a randomized clinical trial, which is how you really determine if a drug treatment works, either to treat or prevent a disease, but it has a lot of…issues. These are issues similar to some of the randomized trials. It’s not clear to me whether this is sloppiness or potentially outright fraud; it could be either. However, this is not a good study. It does appear very impressive, though, to people like Ms. Iversen. I also rather doubt that it was truly a prospective study. Rather, it appears to be a retrospective study masquerading as a prospective study:
This was a prospective, observational study. Although study design, institutional review board (IRB) approval, and data analysis occurred after completion of the voluntary prophylaxis program, all data were collected prospectively in real time with mandated reporting to the registry of all events as they occurred during the citywide governmental COVID-19 prevention with ivermectin program, from July 2020 to December 2020, developed in the city of Itajaí, in the state of Santa Catarina, Brazil. Demographic and clinical data were reported from medical records of patients followed in a large outpatient setting (a provisional outpatient clinic set in the Convention Center of Itajaí) and several secondary outpatient settings, as part of the universal health system (Sistema Único de Saúde [SUS]).
Why is this important? In retrospective studies, one looks at an existing dataset; i.e., patients in the past. In a prospective study, one sets up and looks at patients as they present and collects the data as it happens. Given that, retrospective studies tend to be more bias-prone. What we appear to have here is a prospective data collection for residents of Itajaí onto which was later grafted a retrospective study. Here’s a hint: Just because the data were collected prospectively, you can’t call your study prospective if you designed it after data collection had been completed.
Similarly, the claim that there was a dose-response, I love how Sheldrick described how a massive apparent decrease in mortality could be observed even if ivermectin did nothing. I quote him here because he describes it better and more succinctly than I ever could:
On to the next study.
This study is titled “ Treatment with Ivermectin Is Associated with Decreased Mortality in COVID-19 Patients: Analysis of a National Federated Database“. Not giving me confidence in their abilities, the investigators are plastic surgeons and urologists at the University of Miami. Nothing against University of Miami, but rather plastic surgeons and urologists are generally not the ones who have the correct skills to do a study like this. In any event, this study is also being promoted by FLCCC. Amusingly, one of the authors, a medical student, pushed back:
Hi Dr. Peterson, first author of the paper, I think the information and data is being crudely misrepresented and misinterpreted. This is an abstract (NOT PEER REVIEWED) from a conference I presented at. We did not submit the manuscript for a reason, weak evidence.
— Iakov Efimenko (@AesBrah) March 8, 2022
And he’s right! I didn’t notice that at first, namely that it’s published in a supplement of the International Journal of Infectious Diseases dedicated to publishing Abstracts from the Eighth International Meeting on Emerging Diseases and Surveillance, IMED 2021, November 4-6, 2021. That’s why there’s just an abstract with no full article. I’ll give the student, Iakov Efimenko, credit for being honest. What I won’t do is to spare his mentors. Students can be forgiven for this bad a study, particularly when they learn from the mistake, mentors less so.
Basically, this is an example of confounding by indication. In a retrospective database review, the authors compared patients who received remdesivir for COVID-19 to those who received ivermectin. Can anyone see the problem? It should be obvious, and the name of the confounding should tell you: Patients who receive remdesivir receive it intravenously and are pretty much all hospitalized, while those who receive ivermectin take it as outpatients. As a result, it would be expected that the remdesivir patients would do worse; they’re all hospitalized, and the study didn’t correct for that!
Or:
World's worst study. Remdesivir has to be used as inpatient therapy so patients are already hospitalized vs an oral drug that you can take at any stage of the disease. Worthless data from the bright minds of the department of Plastic Surgery.
— B&B (@Bladeandbarrel) March 3, 2022
Personally, after perusing this thread, I’m less harsh, at least on the students:
The methods are weird.
They found 1.7 million people w/ COVID. Out of this group they identified 1,072 who received ivermectin (not exactly widely used) & 40k who received remdesivir
The groups were very dissimilar: IVM was 10 yrs younger. They don’t report any comorbidities
3/ pic.twitter.com/RI2n1orRcI— Nick Mark MD (@nickmmark) March 3, 2022
The authors are interesting…
The first two are medical students, the 3rd is a plastic surgery resident.
(Nothing wrong with this, though it is weird for the MS not to be affiliated w/ SOM)The fifth & sixth authors are plastic surgeons. Neither has expertise in ID or COVID
5/ pic.twitter.com/wIu7SL1hrI— Nick Mark MD (@nickmmark) March 3, 2022
All of this makes me wonder – did the authors all even read/approve this abstract?
Did the peer reviewers think it was odd that plastic surgeons were doing research on ivermectin for COVID?
7/— Nick Mark MD (@nickmmark) March 3, 2022
As Dr. Mark must know, peer review of abstracts for meetings is pretty perfunctory. Usually most of them are approved for at least a poster presentation. Also, these days, it seems that all specialties seem to view themselves as qualified to do COVID-19 research. I have, after all, seen orthopedic surgeons, ophthalmologists, and all manner of specialties without special expertise in infectious diseases doing COVID-19 research.
In any event, this, too, is not a good study, even as a preliminary hypothesis-generating paper, given the obvious confounders based on indication, hospitalization, and age. It is, however, an excellent case study in the creation of COVID-19 misinformation in real time:
Notice the part where the author woke up to find that his conference abstract had been shared thousands and thousands of times on social media. Notice also how YouTube’s accursed algorithm “suggests” a couple of the very videos by ivermectin-pushing influencers that were mentioned in this video as falsely portraying this abstract as slam-dunk evidence that ivermectin works against COVID-19. It had even been included in the “meta-analysis” at IVMmeta, an anonymous pro-ivermectin site that claims to be doing a “real time meta-analysis” of ivermectin studies.
Ivermectin: The acupuncture of COVID-19
Coming out last week were stories about yet another negative RCT for ivermectin versus COVID-19, for example, this one in The Wall Street Journal, “Ivermectin Didn’t Reduce Covid-19 Hospitalizations in Largest Trial to Date“:
The latest trial, of nearly 1,400 Covid-19 patients at risk of severe disease, is the largest to show that those who received ivermectin as a treatment didn’t fare better than those who received a placebo.
“There was no indication that ivermectin is clinically useful,” said Edward Mills, one of the study’s lead researchers and a professor of health sciences at Canada’s McMaster University in Hamilton, Ontario. Dr. Mills on Friday plans to present the findings, which have been accepted for publication in a major peer-reviewed medical journal, at a public forum sponsored by the National Institutes of Health.
And:
The researchers prescribed half of the patients a course of ivermectin pills for three days. The other half received a placebo. They tracked whether the patients were hospitalized within 28 days. The researchers also looked at whether patients on ivermectin cleared the virus from their bodies faster than those who received a placebo, whether their symptoms resolved sooner, whether they were in the hospital or on ventilators for less time and whether there was any difference in the death rates for the two groups.
But, but, but…, I can hear some of you saying. This study hasn’t been published yet! You’re just citing a newspaper article! True enough. That’s exactly why I only mention this study—and only very briefly, at that—because it is yet another RCT that has failed to find a therapeutic effect for ivermectin versus COVID-19. (If it were the only RCT, I would have waited for it to be published in the peer-reviewed literature before discussing it.) There are a number of other such RCTs, and, again, all the high quality RCTs are negative, including another recent RCT, which was also negative.
Add to that the extreme biological implausibility behind the hypothesis that ivermectin can treat COVID-19. While it is true that ivermectin demonstrates antiviral activity against SARS-CoV-2 in cell culture, the concentrations required are much higher than what can be achieved in the human body. These observations alone meant that it was always highly unlikely that this repurposed anthelminthic drug (used to treat roundworm infestation-based diseases) would ever show activity against COVID-19 in humans at nontoxic (or even toxic) doses. As I described the last time I wrote about ivermectin a few months ago, the pharmacokinetics and pharmacodynamics always meant that the drug probably wouldn’t work in humans, and ivermectin is not “Pfizermectin,” as is claimed in a common conspiracy theory based on the fact that Pfizer’s new COVID-19 drug Paxlovid is a protease inhibitor and ivermectin also demonstrates protease inhibitor activity in cell culture.
The bottom line is that there is now an increasing body of high quality evidence demonstrating that there is no detectable therapeutic effect due to ivermectin against COVID-19. So what are activists doing? Like acupuncture advocates, they’ve stopped looking at high quality RCTs, which are pretty much all negative, and turned their attention to poorer quality studies. Just as acupuncture advocates turned their attention to touting unblinded studies and pragmatic studies, so too are ivermectin advocates now touting retrospective analyses, which can be hypothesis-generating in the absence of an RCT but are, from my perspective, close to pointless in the context of a situation in which several negative RCTs exist. They’re even doing the same thing as acupuncture advocates; i.e., lobbying state legislators for laws that permit their treatment even in the absence of high quality evidence for it, all in the name of “health freedom”.
Truly, ivermectin has become the acupuncture of COVID-19.