
{kind=link}
A long time ago, in—seemingly—a galaxy far, far away (or at least a time that now seems very far, far away indeed), I coined a term, the central conspiracy of the antivax movement. In brief, this conspiracy theory posited that vaccines are harmful, causing autism, autoimmune disorders, cancer, etc., and that “They”—the medical profession, the CDC, the FDA, state governments, and the federal government—know they are causing massive harm but are covering up evidence of that harm. The motivations for the “coverup” vary according to the weaver of the conspiracy theory and generally involve one of or a combination of motivations involving greed, ideology, and control, but the central conspiracy theory has long remained the same. Vaccines are evil; “They” know vaccines are evil; and “They” are covering up and/or actively suppressing the evidence uncovered by the brave maverick doctors and rag-tag vaccine “resistance” conclusively demonstrating that vaccines are evil. Now that longtime rabid antivax activist Robert F. Kennedy, Jr. is Secretary of Health and Human Services and thus in charge of all non-military federal medical, public health, and biomedical research programs, from Medicare/Medicaid, to the Centers for Disease Control and Prevention, to the Food and Drug Administration, to the Public Health Service, to the National Institutes of Health, we are seeing the “unbekoming”—I’ll explain shortly—ideas behind that conspiracy theory become policy under the banner of the “make America healthy again” (MAHA) movement, to the detriment of public health in the US and, more broadly, the world.
This central conspiracy theory of the antivax movement goes beyond just the antivax movement, of course. Its more general version, that there are “natural” cures to diseases that “They” don’t want you to know about, dates back generations and has long been a key feature of the various movements that have existed around alternative medicine, “health freedom,” New Age woo, and the like. Unsurprisingly, this sort of conspiratorial thinking now underlies much of RFK Jr.’s MAHA movement, but there is also an associated central delusion that now underlies the MAHA movement, after having long been a core feature of alternative medicine. Nowhere do I recall having seen it laid out more clearly than in a recent post on a Substack that I recently discovered. The Substack is entitled Lies Are Unbekoming. (I really hate that cutesy stylistically spelling of “Unbecoming.”) The post is entitled You Are Born Defective™: An Essay. (Yeah, whoever the pseudonymous writer of this Substack, who goes by the ‘nym “Unbekoming,” is, they’re clearly very full of themselves.) In this “essay,” Unbekoming claims that the main problem with medicine is that it views human beings as having been “born defective” and in need of correcting.
Unbekoming is clever, though. Here’s how the post is introduced:
This essay operates in two registers. When the medical system’s claims are being examined, the system’s own language is used — vitamin K deficiency, immune system, mutation, cholesterol threshold. This is the establishment being prosecuted in its own words, using its own evidence. When the position the essay actually holds is being stated — that the body is self-healing, self-regulating, and intelligent — the language shifts. The body’s lymphatic and cleansing network is not an “immune system” of warriors and defenders. The MTHFR polymorphism is not a “mutation.” Cholesterol is not a “danger” the body inflicts on itself. The dual register is the structure of the argument: the establishment’s framework is allowed to speak so its contradictions can be heard, and then the terrain framework names what is actually being observed.
There is a huge “tell” in this mass of pseudoprofound, pseudointellectual blather that reveals clearly where Unbekoming is really—if you’ll excuse the term—coming from, and that’s the use of the term “terrain framework.” I’ll discuss that in bit more detail later, but for the moment, “terrain theory” is the 19th century idea championed primarily by one of Louis Pasteur’s competitors, Antoine Béchamp, that it’s not the viruses, bacteria, etc. that are causing disease, but rather that disease is caused by the “terrain” being somehow “damaged” or otherwise hospitable to the outside invaders or causes of disease. It’s an idea that is not entirely untrue. After all, the elderly, the debilitated, those with immune systems that are not functioning properly, whether due to inherent disease or to chemotherapy, are more prone to infection. However, alternative medicine believers—and now MAHA stans—frequently vastly overplay this relationship to argue that the microbes don’t matter much, if at all.
Unbekoming starts with birth and the vision of a human baby that is, well, basically perfect, or nearly so.
Unbekoming: Birth, vitamin K, and vaccines
Unbekoming’s central straw man argument is that conventional science-based medicine views humans as “born defective,” and from that flows the second straw man that medicine must “correct” all these “defects.” To illustrate this, Unbekoming cites the example of the routinely recommended neonatal dose of vitamin K, portraying it in the most “unnatural” and “chemical” language possible, which I will quote in full, even though it’s long, so that you can see clearly what is being done, namely how Unbekoming claims to be “allowing” the “establishment’s framework” to “speak,” which is not actually what is happening here:
The baby is minutes old. The cord has been cut — too soon, but that is another story. The mother has not yet finished holding the child against her chest. A nurse approaches with a syringe.
The syringe contains 1mg of synthetic phytonadione suspended in polysorbate 80, propylene glycol, and a preservative system that has changed several times over the decades the injection has been administered.¹ The dose is roughly 20,000 times what the newborn would receive in a day of feeding on colostrum.² The baby is healthy by every visible measure — pink, breathing, alert, gripping a finger when one is offered.
The injection goes into the thigh muscle. The baby cries. The mother is told this is routine. She is rarely told what the injection is correcting.
What the injection is correcting, the medical system maintains, is a defect. The newborn, in the first days of life, produces clotting factors at levels lower than adult reference ranges. This lower level is called “physiologic deficiency”³ — a term whose internal contradiction passes without examination. The body is producing exactly what its own developmental program calls for, and this is described as a deficiency.
Within the first hour of life, the medical system has identified something wrong with the baby and acted to correct it. This is the first transaction. The baby has been told, on its first day, that the body it arrived with is inadequate.
Note the framing here. The infant is “healthy,” and the evil (and/or deluded) medical system is insisting on ripping it from its mother’s breast to inject it with unnecessary artificial chemicals to correct a what is portrayed as a nonexistent “defect.” (Never mind that babies aren’t ripped from their mother’s breast to be injected with vitamin K. The recommendation is simply that the newborn infant receive an intramuscular dose of vitamin K before leaving the hospital.) The neonatal vitamin K shot is then represented as the first of many “transactions” in which the medical profession portrays the body as inherently “defective” and offers a “correction,” or, as Unbekoming puts it:
There is a paradigm operating beneath modern medicine that is rarely stated as a paradigm, because to state it would be to expose it. The paradigm is that the human body, as it arrives, is defective. It produces too little of some substances and too much of others. Its immune capacities are insufficient. Its genetic code carries errors. Its measurements drift, with age, into pathological ranges. Each of these defects is the basis for a product or procedure that corrects it.
This passage literally made me chuckle out loud, given that this verbiage, minus the portrayal of ripping a baby from its mother’s arms to inject it with toxic chemicals, describes the very foundation of a branch of alternative medicine much favored by MAHA and practiced by MAHA bigwigs like former Surgeon General nominee Dr. Casey Means and Dr. Mark Hyman, namely functional medicine (FM). FM basically does what Unbekoming spends the Substack post accusing modern medicine of doing, but on massive doses of steroids. Basically, FM involves massive overtesting for diseases and conditions in the asymptomatic or “worried well,” with some FM panels involving hundreds of blood markers. Abnormalities in these panels of tests, often repeated at least once a year, are then “corrected” by selling supplements targeting every abnormality, whether clinically relevant to anything or not. Functional medicine, as I like to say, is based on reams of useless tests in one hand and a huge invoice in the other. Unsurprisingly, Unbekoming loves functional medicine to death.
How’s that for allowing Unbekoming’s own contradictions to be revealed by simply quoting what is written?
Vitamin K is an essential factor for one arm of the clotting system in mammals. As we have explained many times over the history of this blog when discussing vitamin K fear mongering by antivaxxers, the reason for the vitamin K injection is that neonates can be relatively deficient in vitamin K because it doesn’t easily cross the placenta and is relatively deficient in breast milk, which can leave infants relatively deficient until they start eating other foods at around six months of age. As Steve Novella noted six years ago, one dose of intramuscular vitamin K at birth “significantly reduces that risk (relative risk in that study was 0.19, with a number needed to treat of 74),” immediately increasing “vitamin K levels, with most of the vitamin being stored in the liver where it is slowly released over the next six months.” He also notes that the risks are minimal. In an earlier post, Steve noted that recent studies looking at infants who developed VKDB showed that most or all of them did not receive vitamin K prophylaxis. For a more in-depth discussion of why a routine neonatal dose of vitamin K is safe and effective, Dr. Clay Jones has you covered. Yes, these posts are several years old, but, seriously, the arguments made by people like Unbekoming against the routine vitamin K dose for neonates haven’t changed, nor has the evidence supporting this practice, other than more data showing it to be safe and effective.
Unbekoming does at least admit that the condition that the neonatal vitamin K injection is designed to prevent, namely Vitamin K Deficiency Bleeding (VKDB), is real; so there’s that. It’s even acknowledged that there are three subtypes of VKDB:
- Early onset VKDB (within 24 hours): Rare; usually associated with maternal medications (e.g., anticonvulsants, warfarin).
- “Classic VKDB” (days 2–7): The most common form without vitamin K prophylaxis; GI bleeding, umbilical bleeding, or post-circumcision bleeding.
- Late onset VKDB (weeks 2–12): The most dangerous form — intracranial hemorrhage occurs in 30–60% of cases and carries significant mortality and neurological morbidity. Exclusively breastfed infants are most at risk.
It’s even acknowledged that vitamin K prophylaxis eliminates the risk of late onset VKDB, which is cited as having an incidence of between one in 14,000 and one in 25,000 infants. (Hint: There are roughly 3.6 million births per year in the US, which, if you accept Unbekoming’s numbers, would translate into potentially 144-257 cases of late onset VKDB, a catastrophic condition, per year. There used to be a time when we thought that preventing hundreds of dead or severely neurologically injured infants was a good thing, but apparently not to MAHA’s way of thinking anymore. (RFK Jr. and HHS have backed away from routinely recommending neonatal vitamin K injections, and more parents are refusing the shots.)
But it’s all so “unnatural.” Unbekoming goes on and on about the excipients used for intramuscular vitamin K injections:
The injection is not vitamin K alone. It contains polysorbate 80, a surfactant shown in animal studies to alter blood-brain barrier permeability¹⁰; propylene glycol, which the FDA itself has warned about in neonates¹¹; and benzyl alcohol, which has been associated with “gasping syndrome” and infant deaths.¹² The product carries a black box warning — the FDA’s most serious — that reads “severe reactions, including fatalities, have occurred during and immediately after intravenous and intramuscular injection,” noting that “some patients have exhibited these severe reactions on first receiving phytonadione.”¹³ A 1992 study from the British Medical Journal reported an association between intramuscular vitamin K and childhood cancer.¹⁴ Subsequent studies disputed the finding. The dispute is unresolved. The injection continues.
First of all, phytomenadione is simply vitamin K1. Second, the dispute is not “unresolved.” Since the study mentioned, epidemiological studies have consistently failed to find an association between the birth dose of vitamin K and increased risk of any cancer. The purported “risk” at this time is purely hypothetical and therefore far outweighed by the benefits of the neonatal vitamin K injection.
As for polysorbate-80, unmentioned is that the animal studies cited used large doses of polysorbate-80, far above what a human infant receives in a vitamin K injection. (Indeed, the quantities of excipients like propylene glycol and polysorbate-80 in current vitamin K injectable formulations in the US are minuscule, making this attack just another variation of the “toxins” gambit beloved of antivaxxers.) Most were studies of polysorbate-80 in the diet, and most recent studies of polysorbate-80 and the blood-brain barrier that I could find involved using polysorbate-80 in lipid nanoparticles designed specifically to target the blood-brain barrier. Indeed, the study cited by Unbekoming to support the fear mongering about polysorbate-80 is a 1985 study in which levels of chemotherapeutic agents were measured in the brains of mice when dosed with and without polysorbate-80 included in the mice’s diet. Surely, if this were a major concern, they could have come up with a more relevant (and recent) study. At least, if I were trying to make the same argument, I’d find something less than four decades old that directly addressed the claim. Ditto benzyl alcohol, for which the reference cited comes from 1982 and looked at doses 100 times higher than what is in vitamin K shots, and even if parents are concerned about the presence of this chemical in the shots there is a preservative-free version of intramuscular vitamin K. Not that any of this stops Unbekoming from citing the litigation-driven antivax pseudo-“study” the Control Group as evidence for the dangers of vitamin K injection.
[NOTE ADDED AFTER PUBLICATION: Ironically, after I finished this post, I noticed that antivax physician Suzanne Humphries showed up on the website of the antivax org founded by RFK Jr. parroting basically the same claims about benzyl alcohol, the now disproven elevated risk of childhood cancer from the shot, and even the claim that the lower vitamin K levels in neonates is “by design” for a purpose. Yep. Unbekoming is parroting old antivax nonsense about vitamin K shots.]
Finally, Unbekoming asks what they must think to be a reasonable question: Why not just give the vitamin K orally in divided doses, as though it were pure ideology—”the hospital workflow is built around injection”—and grift that led the American Academy of Pediatrics to recommend one intramuscular dose of vitamin K1 in 1961 and reaffirm the recommendation in 2021. In reality, a single intramuscular dose provides protection for months. In contrast, oral regimens require multiple doses and have a higher failure rate, particularly for late-onset VKBD. If you listen to Unbekoming, though:
The newborn is not deficient. The newborn is producing vitamin K at the level the newborn’s developmental program calls for, in a body whose clotting system is calibrated to that level. The “deficiency” is defined against an adult reference range that has no biological relevance to a three-day-old infant. A genuine clinical bleeding risk exists in a small subset of infants with underlying pathology, and that risk is real and serious. The response is to inject every newborn, mask the signal that would have identified the at-risk subset, and accept the toxic burden of the carrier substances in exchange for protection against a condition most infants would never have developed.
The reason that the deficiency is defined the way it is is because at the lower level of vitamin K in neonates, the clotting system doesn’t work as well, and there actually is a risk of catastrophic bleeding. I also wonder what “signal” that would identify the “at-risk subset” is being “masked” by a universal neonatal vitamin K dose. What would that “signal” consist of? What action would Unbekoming recommend when an “at-risk” infant is identified? This is basically the same sort of MAHA appeal to “individualized” care that is, in reality, an excuse for undermining public health interventions.
Unsurprisingly, Unbekoming moves on to make the same sort of “appeal to perfect nature” to argue against the childhood vaccine schedule, portrayed this way:
The premise of the schedule is that the child’s lymphatic and cleansing network cannot adequately respond to childhood exposures without injected antigens, adjuvants, and excipients. Stated baldly, this is implausible. Children have been having childhoods for as long as there have been children. The lymphatic system, the fascial network, the mucosal surfaces, the liver, the kidneys — these are not new structures awaiting pharmaceutical activation. They are the body’s cleansing and adaptive architecture, refined across the entire arc of human existence.
“Implausible.” You keep using that word. I do not think it means what you think it means. Yes, children have been having childhoods as long as there have been children, and children have been dying of infectious diseases as long as there have been children. In the 19th century, huge numbers of children died of what are now vaccine-preventable infectious diseases, to the point where it was common for families to lose one, two, three, or even more of their children before they grew up. It’s a straw man to say that the child’s immune system “can’t” adequately respond to childhood exposures. The problem is that the immune system needs training. If it hasn’t seen an antigen before, it will not do as well dealing with that antigen as it will if it has seen it before. Vaccines do nothing more than prime the immune system by letting it see antigens of potentially dangerous disease-causing microbes in a safe manner that doesn’t cause disease, so that it “remembers” them when it encounters them for real.
The rest of Unbekoming’s section on vaccines consists of a lot of well-worn, common, and easily debunked antivax talking points, such as the “toxins” gambit, the “no saline placebo” gambit, the false claim that unvaccinated children are healthier than vaccinated children, and a truly brain-dead analogy:
The injection volumes themselves are worth pausing on. A two-month-old infant weighing roughly 5kg may receive, in a single visit, vaccines totalling around 2.5ml of injected material. Scaled to the body mass of a 70kg adult, the equivalent volume would be approximately 35ml — over two tablespoons of injected pharmaceutical product in a single visit.²⁹ No adult medical protocol approaches this density. The infant receives it in a body still building the structures the substances are delivered into.
Here’s a hint: Vaccines are not like standard pharmaceuticals. The doses do not scale linearly with weight; that’s not how the immune system works. Moreover, 35 ml is not a large fluid volume for an adult, just as 2.5 ml is not a large fluid volume for a two-month-old infant. Whether Unbekoming doesn’t know these—i.e., is just ignorant—or does know these things but knows that their audience doesn’t—i.e., is lying—I don’t know. Take your pick.
Either way, Unbekoming’s fallacy is the same for both vitamin K and vaccines:
Both pillars rest on the same proposition: the body is defective at baseline. The proposition is not stated this way in medical literature. It is implicit in the structure of every intervention. Each procedure, each prescription, each diagnostic threshold rests on the same foundation — that the body, as it arrives and as it ages, fails to meet a standard the medical system has the authority to set and the products to address.
There is another paradigm. It is older than germ theory. It survived the institutional capture of the early twentieth century only at the margins, in the work of Béchamp, Bernard, Tilden, Shelton, Price, and their inheritors. The paradigm holds that the body is a self-healing, self-regulating, intelligent organism. It maintains its own equilibrium. It does not make mistakes. It does not attack itself. It responds to insult — toxic, nutritional, electromagnetic, emotional — with intelligent processes aimed at restoring balance. Symptoms are not malfunctions; they are the body’s response to conditions that warrant a response. Disease arises from terrain conditions, not from baseline defects.
There it is, as expected, the appeal to terrain theory. While it’s true that terrain theory was a legitimate competitor to Pasteur’s germ theory of disease in the mid-19th century, the bottom line was that it lost the race. It was a hypothesis that seemed reasonable at the time, given what was known about medicine, but ultimately failed to be validated as science progressed, just like so many other hypotheses and theories over the history of medicine and science. Scientific evidence and experiments increasingly supported Pasteur and did not support Béchamp. Yes, it’s true that “terrain” contributes to one’s susceptibility to disease, but unfortunately people like Unbekoming seem to make like Bill Maher and claim that if one’s “terrain” is maintained through diet, exercise, and other “virtuous” behavior with respect to health practices, then they are not susceptible to disease and don’t need vaccines. Bob Costas had the perfect retort to such arguments: “Oh, come on, Superman!“
As for the body being “self-healing,” “self-regulating,” and “intelligent,” there is some truth to that, but, like quack-lovers everywhere, Unbekoming massively overstates the case. The body can “self-heal” and “self-regulate,” but there are definite limits, and the system doesn’t always work correctly (e.g., in the case of auto-immune diseases and cancer). As for “intelligence,” the brain produces intelligence, but the body’s homeostatic systems are more akin to algorithms than intelligence.
Naturally, all of this “reasoning” (if you can call it that) leads to the conspiracy theory that science-based medicine promotes vitamin K and vaccines for infants and children because it is creating “diseases” or “deficiencies” of the oh-so-perfec human body in order to profit, which, again, is truly rich given how much quacks and, more recently, MAHA have promoted supplements for nonexistent diseases:
This paradigm has no product line. It generates no patents. It cannot be billed. A body that needs only to be supported — through clean food, clean water, low toxic burden, low stress, sunlight, movement, sleep — produces no revenue. The medical system as currently structured cannot operate on this paradigm. It requires the other.
Oh, you sweet summer child! (Either that, you know damned well that a body that “needs only to be supported” can be monetized by selling it products that allegedly help it with “clean food, clean water, low toxic burden, low stress, sunlight, movement, sleep.”)
Into the adult world
I’m not going to spend as much time on the two adult examples that Unbekoming uses to try to make the same “argument” (such as it is), specifically methylenetetrahydrofolate reductase (MTHFR) mutations (referred to as “defective” genome) and statin treatment for hypercholesterolemia (referred to as “the defective adult”). Once again, I chuckled out loud when I saw that Unbekoming was going to “go there” when it comes to MTHFR mutations, given that testing for such mutations has become such a cottage industry among quacks, MAHA-aligned and otherwise, that eight years ago genetics experts at the Cleveland Clinic called out all the dubious tests for MTHFR mutations being marketed. Most of the time genetic testing for MTHFR mutations.
Just to remind readers, folic acid is not metabolically active itself. It must first be converted to dihydrofolate (DHF) and then to tetrahydrofolate (THF) through enzymatic reduction, a reaction that is catalyzed by the enzyme DHF reductase (DHFR). After that, THF can be converted to the biologically active l-methylfolate by the enzyme methylenetetrahydrofolate reductase (MTHFR). This key conversion is necessary to provide l-methylfolate for the one-carbon transfer reactions needed for purine and pyrimidine synthesis during DNA and RNA assembly, for DNA methylation, and to regulate homocysteine metabolism. Thus, MTHFR is the critical enzyme for almost all biologic processes that involve the metabolism of folate and methionine.
Here’s a diagram illustrating its role:
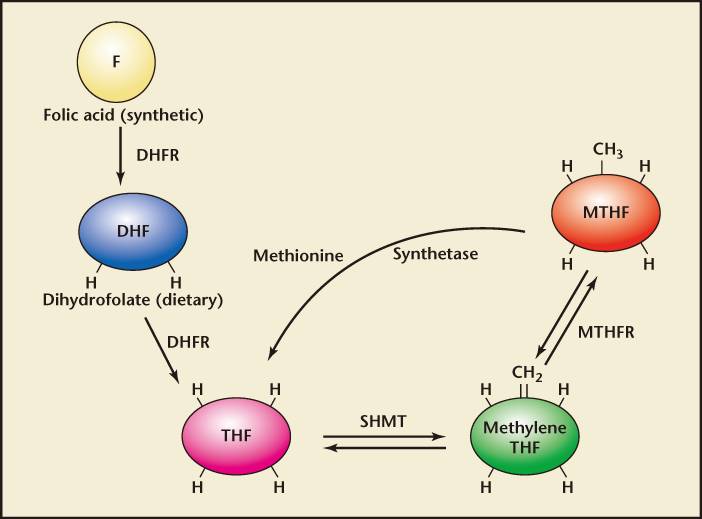
To be honest, I almost think that Unbekoming might be calling out the quacks here, because, seriously, most science-based medical professionals aren’t going to be routinely ordering MTHFR mutation testing for patients, certainly not for patients complaining of “fatigue,” but a whole lot of MAHA-aligned quacks, particularly functional medicine quacks and naturopath quacks, will. I wanted to assume that, but in reality this whole example serves mainly as an excuse to attack folic acid supplementation as “artificial” and “toxic,” a “chemical” that wasn’t synthesized until 1943. Meanwhile, two common variants, C677T and A1298C, are portrayed as totally “natural” and harmless because approximately 40% of the population carry them.
In reality, this is all a pretext for nothing more than attacking the addition of folic acid to foods—referred to, tellingly, as being “added through industrial fortification”—and the recommendation that people who are pregnant or who plan on becoming pregnant supplement with folic acid. I’m not going to go into gory detail on this topic, because, unsurprisingly, it’s a lot more nuanced than Unbekoming portrays it:
A patient is told they carry the mutation. They are told it predisposes them to cardiovascular disease, pregnancy complications, neural tube defects, depression, autoimmune conditions, and detoxification impairment. They are told they must supplement with methylated folate — 5-MTHF — for life, because they cannot adequately process folic acid.³¹
Yes, the most dreaded pregnancy-related consequence of folate deficiency is neural tube defects in the developing fetus, which is why folic acid supplementation has been routinely recommended during pregnancy. Interestingly, the reference cited doesn’t actually say this. It’s all about folate metabolism and how supplementation with folic acid prevents all the bad things that can happen with folate deficiency, such as birth defects and other adverse pregnancy and health outcomes. What does it say about L-methyfolate?
Not much:
Although folic acid supplementation to supraphysiologic levels has demonstrated many of the benefits to pregnant women and fetuses noted above, the potential risk of high-dose folate supplementation must also be considered. First, folate supplementation can mask vitamin B12 deficiency (pernicious anemia) and care must be taken with susceptible individuals to avoid missing this diagnosis. Also, concerns have been raised about the potentially untoward effects of unmetabolized synthetic folic acid with regard to cancer, depression, and cognitive impairment. 52 With all these concerns, early data suggest supplementation with l-methylfolate rather than folic acid may mitigate these risks.53
See what I mean? (Note that L-methylfolate and 5-MTHF are the same substance.) All this review says is that using 5-MTHF instead of folic acid might mitigate potential effects of unmetabolized folic acid and that “newer research in this area has focused on supplementation with l-methylfolate rather than folic acid as a means of preventing folate-related pathology,” not that the standard recommendation is that if you have an MTHFR variant that interferes with folate metabolism you will definitely need to take 5-MTHF for the rest of your life. Of course, this review is from 2011—Unbekoming seems incapable of citing newer literature—and so I looked up some newer literature. As of November 2024, the American College of Medical Genetics, for instance, recommends against routine screening for MTHFR polymorphisms/mutations and that “women of childbearing age should take the standard dose of folic acid supplementation to reduce the risk of neural tube defects as per the general population guidelines.” As for the general population, it recommends that “MTHFR positive individuals may decide to take vitamin B and folic acid supplements. Although safe (toxicity is rare), evidence is lacking on whether such supplements reduce the risks associated with hyperhomocysteinemia or MTHFR genotype status.”
That sure doesn’t sound like how Unbekoming is portraying modern medicine and how it deals with MTHFR mutations. What Unbekoming describes sounds a lot more like how functional medicine quacks and naturopaths deal with MTHFR variants. Be that as it may, Unbekoming concludes here:
The genome is not defective. The diet is. The defect-claim has been moved from the food supply, where it belongs, to the patient’s DNA, where it absolves the food supply and creates a permanent customer for the supplement industry. The genome, which existed long before the synthetic compound it is being declared inadequate to process, is now held responsible for the inadequacy of the synthetic compound.
The funny thing is, the medical consensus with respect to MTHFR variants seems to be similar: that these are not “defects” and that, unless you’re trying to become pregnant, you probably don’t need to do anything other than eat a good diet with green, leafy vegetables. If you are trying to become pregnant, supplement with folic acid to prevent neural tube defects and other defects in your baby.
The next example, “the defective adult,” is basically your standard anti-statin nonsense. Pretty much everything written by Unbekoming is nonsense of the sort I once wrote extensively about when COVID quack Pierre Kory started to embrace statin denial; so I won’t go into much detail regarding the claims, although I do love a claim like this:
In 1984, the cholesterol threshold for treatment in adults was 240 mg/dL.³⁴ In 1993, it dropped to 200 mg/dL. In 2001, the threshold for high-risk patients dropped to 100 mg/dL. In 2004, it dropped again to 70 mg/dL for very high-risk patients. The 2004 update was authored by a panel of nine members, eight of whom had financial ties to statin manufacturers.³⁵ Each threshold reduction expanded the eligible patient population by tens of millions. Statin prescriptions in the United States exceeded 200 million annually by the 2010s, generating revenue in the tens of billions.³⁶
Yes, and blood pressure thresholds for the diagnosis of hypertension have dropped through the decades as well. It’s what happens as more epidemiological and clinical evidence accumulates and guideline organizations realize that there is a benefit to intervening at lower values, which Unbekoming misrepresents by discussing a hypothetical patient with elevated cholesterol who was prescribed a statin:
The doctor does not mention that the threshold he now fails was lowered by a committee in which eight of nine members held financial ties to the manufacturers of the drug he has just been prescribed.
Here we go with the conspiracy theories again.
This leads Unbekoming to repeat what is, after the previous three examples, a now-familiar refrain adapted for cholesterol and statins:
Cholesterol is not dangerous. It is required. The body manufactures it in the quantities the body requires. When measurements are taken and compared to thresholds, the thresholds are being moved to expand the patient population, not to track a biological change. The “high cholesterol” of a healthy adult is the cholesterol level a healthy adult produces. Treating it with a drug that interrupts a biosynthetic pathway producing multiple essential compounds is not correction of a defect. It is induction of a deficiency.
Again, it never occurs to Unbekoming that the body might actually malfunction, that it might make too much of a substance and that too much of that substance might actually cause health problems. Given this framework, I have to wonder why the article didn’t mention type 2 diabetes, with the argument that impaired glucose metabolism is normal for the person with type 2 diabetes and that metformin and GLP-1-based drugs are all a big scam to induce a glucose deficiency.
What ties them all together? According to Unbekoming:
The four pillars share an architecture. A measurement is taken or a category is named, a threshold is set or a defect is claimed, a product is offered. The threshold is positioned as biology; the product is positioned as correction.
In each case, the body is held to a standard the body did not set. The newborn is measured against an adult reference range with no biological relevance. The child is measured against an immune theory that requires injected substances to function. The adult is measured against a synthetic compound invented in 1943. The aging adult is measured against a threshold lowered by a committee paid by the manufacturer.
In each case, the actual cause of the symptoms or risks the intervention claims to address is foreclosed. The newborn’s bleeding risk, where it exists, is from underlying pathology that the universal injection masks. The child’s chronic disease load is from the toxic burden of the schedule itself, alongside diet and environment. The adult’s MTHFR symptoms are from a diet built around fortified processed food. The adult’s cardiovascular risk is from inflammation driven by diet, stress, toxic exposure, and metabolic dysregulation — not from cholesterol levels the body itself maintains.
In each case, the patient becomes a customer for life. The newborn injection initiates the relationship. The schedule extends it. The MTHFR diagnosis cements it. The statin completes it. From the first hour to the last, the body has been a revenue stream, and the defect-claim has been the mechanism by which the revenue stream was constructed.
There it is, the central delusion of MAHA, that the body is this all-knowing, (nearly) all-powerful self-healing machine and that the only thing that prevents it from healing itself of virtually anything are the “toxic load” of chemicals and pharmaceuticals that the medical profession nefariously hooks you on by declaring your body to be less than perfect, full of “deficiencies” that must be corrected for the rest of your life. Given that viewpoint, it should not surprise anyone that Unbekoming is a virus denier, basically claiming that viruses don’t really exist in posts such as What Is Ebola? and What Is Hepatitis C? Amusingly, Unbekoming argues that Ebola doesn’t really exist, that it is really arsenic poisoning, much as antivaxxers did for the polio virus in the past, and “poisoning” due to other industrial toxins related to mining. (Everything old is new again.) Meanwhile, hepatitis C isn’t due to a virus, but just “toxins” that are “poisoning” the liver. (Everything old is new again.)
As Unbekoming shows us, the central delusion of MAHA now (and a lot of alternative medicine in the past that has now glommed onto MAHA) is that the body is basically perfectly functional, even when it’s not. The lower level of vitamin K in the neonatal bloodstream is exactly as nature intended, and the neonatal birth dose is an abomination that “masks” those who are truly “at risk” for VKDB at the cost of exposing all babies to supposedly horrific “toxins.” Your immune system is already exactly as nature intended it to be, and vaccines only interfere with that perfection, again at the cost of exposing the body to horrific “toxins.” Your genome is also exactly as nature intended it to be, and food alone is enough to prevent neural tube defects if you happen to have an MTHFR variant that leaves you deficient in folate. If you have elevated cholesterol, it’s just as nature intended and not at all harmful, even though medical research tells us that there is increasing risk of cardiovascular disease with elevated levels of LDL and cholesterol.
This delusion leads to a single answer to nearly all medical problems related to chronic disease. A medically virtuous diet and lifestyle will fix everything and prevent all diseases—I only exaggerate slightly—and you don’t need pharmaceuticals or vaccines. Would that this were true, but unfortunately we live in the real world. Our bodies are not perfect. Far from it. Most of us will need medical care at some point in our lives, often at many points. The central delusion of MAHA is to deny this essential reality.