
{kind=link}

“Ebola virus particles” by Thomas W. Geisbert, Boston University School of Medicine – PLoS Pathogens, November 2008 doi:10.1371/journal.ppat.1000225. Licensed under CC BY 2.5 via Wikimedia Commons.
Without a doubt the big medical story of the last week or so has been the ongoing outbreak of Ebola virus disease in West Africa, the most deadly in history thus far. Indeed, as of this writing, according to a table of known Ebola outbreaks since 1976 at Wikipedia, in Guinea, Sierra Leone, and Liberia, the three nations affected thus far, there have been 1,440 cases and 826 deaths. Worse, the World Health Organization (WHO) is reporting that it is spreading faster in Africa than efforts to control it. In particular, late last week it was announced that two Americans who had been infected with Ebola were going to be flown back to the US, specifically to Emory University, for treatment, a development that ramped up the fear and misinformation about Ebola virus to even greater heights than it had already attained, which, unfortunately, were already pretty high. Indeed, the ever-reliably-histrionic Mike Adams of NaturalNews.com wrote a typically hysterical article “Infected Ebola patient being flown to Atlanta: Are health authorities risking a U.S. outbreak?” On Saturday, we learned that Dr. Kent Brantly, an aide worker for Samaritan’s Purse, a Christian charity run by Franklin Graham, son of the well-known preacher, Billy Graham, who had been evacuated from Liberia aboard a private air ambulance, had arrived in Georgia.
This latest development inspired medical “experts,” such as Donald Trump, to stoke fear based on the arrival of two infected Americans in the US. For instance, last Friday, after it was first announced that the Ebola-infected Americans would be flown back to the US, Trump tweeted:
Stop the EBOLA patients from entering the U.S. Treat them, at the highest level, over there. THE UNITED STATES HAS ENOUGH PROBLEMS!
— Donald J. Trump (@realDonaldTrump) August 1, 2014
One is tempted to add that ignorant Twitter tirades by billionaires with far more money than sense are also one of the “enough problems” that the US has. After all, besides having embraced conspiracy theories like “birtherism,” Trump has been a raving antivaccinist since at least 2007. So, right there, you know that Trump’s knowledge of medicine is—shall we say?—lacking, to put it kindly. None of that stopped him from following up with more fear mongering:
The U.S. cannot allow EBOLA infected people back. People that go to far away places to help out are great-but must suffer the consequences!
— Donald J. Trump (@realDonaldTrump) August 2, 2014
And:
The U.S. must immediately stop all flights from EBOLA infected countries or the plague will start and spread inside our "borders." Act fast!
— Donald J. Trump (@realDonaldTrump) August 2, 2014
And:
The fact that we are taking the Ebola patients, while others from the area are fleeing to the United States, is absolutely CRAZY-Stupid pols
— Donald J. Trump (@realDonaldTrump) August 2, 2014
Trump also re-Tweeted a bunch of equally overheated Tweets about the topic, and meanwhile WorldNetDaily is stoking fears of illegal immigrants massing at our southern border to bring in Ebola and other diseases, bolstered by Dave Hodges and the president of the American Association of Physicians and Surgeons (remember the AAPS?), Dr. Jane Orient, who are claiming that “100,000 West Africans are in Central America, have been taught to speak Spanish and are coming across our Southern border” carrying Ebola, naturally. These claims are based on anonymous and unverifiable “sources.” All of this is why now seems an opportune time to discuss the Ebola outbreak from a science-based perspective and whether or not bringing back these two Ebola patients is such a huge mistake that, if Mike Adams and Donald Trump (and several others) are to be believed, will endanger this country with the possibility of an Ebola epidemic. The time is all the more appropriate, given that, as they all too frequently do, quacks are promoting their remedies as cures for Ebola. So what is the situation, really?
What is Ebola virus disease?
The disease caused by Ebola virus belongs to a class of diseases known as viral hemorrhagic fevers. It’s a diverse group of diseases caused by Ebola virus that range in severity from relatively mild to exceedingly deadly, but all share in common the tendency of being complicated by disseminated intravascular coagulation (DIC), which eats up clotting factors and results in an increased susceptibility to bleeding. Other hemorrhagic fevers include dengue, yellow fever, Marburg virus, Lass fever, and more. There are five classes of viruses, all RNA viruses, that can cause hemorrhagic fever; of these, the Ebola virus belongs to the family Filoviridae, because the viruses form filaments, as you can see from the photo of an Ebola virus at the beginning of this post, and uses negative-sense single-stranded RNA as its genetic material, which is used both to produce more viral protein and to produce an antisense template to produce more viral RNA. The virus was discovered in 1976 and has caused sporadic outbreaks since then. It’s diagnosed by a combination of history (particularly of travel to areas where the disease is found) and clinical history, but definitive diagnosis is made using either enzyme-linked immunoassay (ELISA) for viral proteins or reverse transcriptase polymerase chain reaction (RT-PCR) for the viral RNA.
There are five subtypes of Ebola virus:
- Ebola-Zaire
- Ebola-Sudan
- Ebola-Ivory Coast
- Ebola-Bundibugyo
- Ebola-Reston
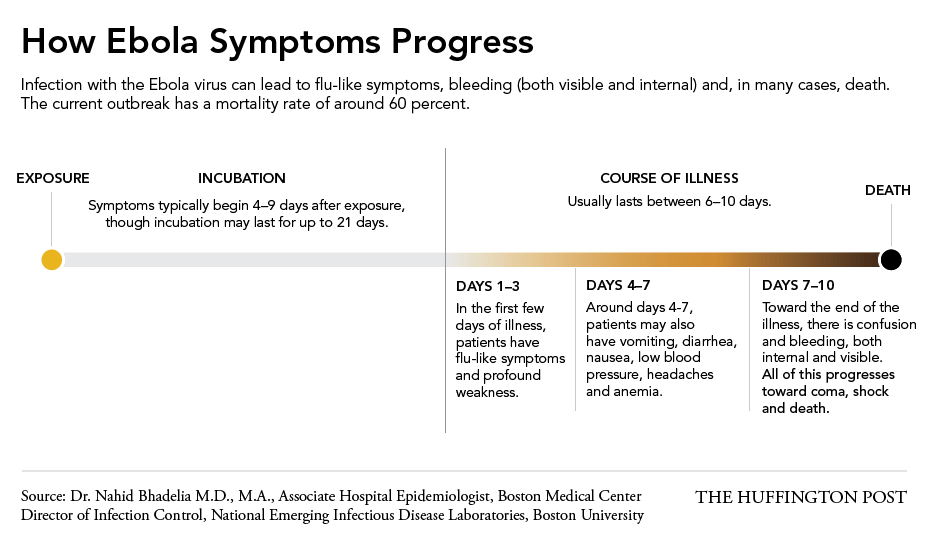
Ebola-Reston, which is found in the Philippines, doesn’t cause human disease, but all the others, which are found in Africa, do. Of these, the Zaire strain of Ebola is the most deadly, with a greater than 90% case fatality rate. It is the most feared of all the strains of Ebola virus, and quite rightly so. However, it should be remembered that the figure of 90% fatality is the case fatality rate with essentially no treatment. With modern medical care, the case fatality rate, even for Ebola-Zaire is more like 56%, which is still quite bad. In this specific outbreak, thus far the case fatality rate is around 57%.
After infection, symptoms usually begin within 5-10 days. Early signs and symptoms are very much like influenza or other flu-like illnesses and include fever and chills, headache, joint and muscle aches, and weakness. With progression, additional symptoms can include a maculopapular rash, cough, nausea and vomiting, and abdominal pain. The bleeding that gives hemorrhagic fevers their name can, in the case of Ebola disease, manifest itself many ways, including bleeding from the eyes, hematemesis (vomiting blood), hemoptysis (coughing up blood), melena (dark blood in the stool from upper GI bleeding), hematochezia (red blood in the stool), bleeding from orifices (such as ears, mouth, and nose), and internal bleeding. As the disease progresses, multiple organ failure can occur, contributing to death:
{kind=link}
Those who survive can suffer long-term complications, such as hepatitis, fatigue, headaches, and testicular inflammation.
Worse, Ebola is a master of evading the immune system:
The Ebola virus is also a master of evading the body’s natural defenses: It blocks the signaling to cells called neutrophils, which are white blood cells that are in charge of raising the alarm for the immune system to come and attack. In fact, Ebola will infect immune cells and travel in those cells to other parts of the body — including the liver, kidney, spleen and brain.
Each time one of the cells is infected with the Ebola virus and bursts, spilling out its contents, the damage and presence of the virus particles activates molecules called cytokines. In a healthy body, these cytokines are responsible for provoking an inflammatory response so that the body knows it’s being attacked. But in the case of an Ebola patient, “it’s such an overwhelming release [of cytokines], that’s what’s causing the flu-like symptoms” that are the first sign of Ebola, Bhadelia said.
Yes, Ebola is a very, very bad disease. Worse, there’s not much that even modern science-based medicine can do to treat the virus specifically. Basically, the treatment consists of supportive care: Fluid resuscitation to prevent dehydration, transfusion as needed to replace blood loss; treat the DIC with clotting factor replacement, and respiratory and cardiovascular support if needed. It’s true that there are experimental drugs that has shown promise in preclinical models, and the search for an Ebola vaccine has been put on the fast track, but as of now there is no approved treatment or vaccine for Ebola.
So should we be bringing victims to the US for treatment?
Treat in Africa or treat in the US?
So are the concerns of Donald Trump and Mike Adams justified? One of the two Americans infected with Ebola (Dr. Kent Brantly) is already here. The second, Nancy Writebol, will leave Africa tomorrow. In considering whether bringing these patients back home is so dangerous that it shouldn’t have been done, it’s important to consider two things: how Ebola is transmitted and existing isolation protocols.
Ebola virus, although contagious, is not nearly as contagious as, for example, influenza or measles, both of which are easily spread through the air. Ebola, by comparison, is transmitted through contact with body fluids (blood, saliva, semen, vomit, urine, or feces) in much the same way HIV or hepatitis B is. Although transmission through aerosol has been demonstrated in the laboratory between pigs and primates, it has never been conclusively demonstrated to happen from human to human and the evidence is fairly compelling that it does not. True, the virus, from what I’ve found in my research, persists on surfaces for days, and only 1-10 virus particles are needed to initiate infection. Most people acquire the virus through contact with the blood or bodily fluids of the infected (as in blood from an infected person coming into contact with the mucus membranes of the mouth or eye or with an open cut) or through nosocomial transmission (accidental needle sticks with a syringe containing infected blood, for instance). In Africa, given how poor the countries suffering outbreaks tend to be, the nosocomial route is prominent, because of reuse and improper sterilization of syringes, needles, or other medical equipment contaminated with these fluids. Also in Africa, a common means of acquiring the virus is preparing the bodies of the dead for funerals.
Dr. Bruce Ribner, one of the doctors who will be caring for Ebola patients described the situation nicely:
Ebola isn’t “some mystical pathogen (with) some bizarre mode of transmission,” the doctor noted, adding that it is transmitted similarly to illnesses like SARS or HIV.
So, if patients are brought to the US (as one has already been as of this writing), it’s not as though American hospitals don’t have considerable experience with universal blood and bodily fluid precautions, and it’s not as though they don’t properly sterilize instruments and equipment between uses. In other words, there’s nothing unique about Ebola virus in terms of transmission. No one’s saying the risk is zero, but it’s incredibly low, the blatherings and bloviations of ignorant gasbags like Donald Trump on Twitter notwithstanding. One also notes that the CDC has stocks of the virus, which it studies, which means that Ebola virus is already on US soil (in various universities, an Army facility, and the CDC) and Canadian soil, along with patient blood samples from Africans infected with the various forms of Ebola. As a real infectious disease expert, Tara Smith, pointed out, not only is Ebola already in the US, but US health officials have already dealt with cases and small outbreaks of related hemorrhagic fevers, such as Lassa fever and Marburg.
Moreover, Emory University is better equipped than most hospitals to deal with such patients:
Emory University Hospital, which is slated to care for the patients, has a specially designed wing separate from the rest of the hospital that was created to treat people infected by bioterrorism attacks or pandemics.
But Dr. William Schaffner, an infectious disease specialist and professor of preventive medicine at Vanderbilt University, says almost any American hospital is equipped to take care of an Ebola patient without endangering staff or the public.
Infectious patients are put in an isolation room, and health workers have to put on protective gear before entering the room. They remove the gear when leaving. It is put in red infectious disease waste bags, which are burned.
Even though Ebola isn’t spread through the air, the CDC says that patients probably will be put in negative-pressure rooms that isolate air so it can’t circulate through the building. Those are typically used with patients with active tuberculosis, which is airborne.
It’s also noted that it isn’t the precautions that might fail, but the humans doing the precautions, as Schaffner noted that they were “busy” or “because familiarity breeds if not contempt then casualness.” This was learned in Toronto dealing with the SARS outbreak when hospital workers dealing with SARS patients became infected. Posting monitors outside the patients’ rooms to make sure personnel followed the precautions eliminated any further cases. Emory did the same thing when patients with suspected Middle East Respiratory Syndrome (MERS) were admitted, and, given the level of fear over Ebola virus, you can be quite sure that anal sphincters will be even tighter this time. Moreover, given that, as far as has been ascertained, Ebola does not spread through the air as SARS and MERS do, the likelihood of nosocomial transmission to a health care worker is minimal, particularly given that any staff in contact with Ebola victims will almost certainly be carefully monitored for any signs of viral infection and rapidly quarantined if they exhibit them. Again, the likelihood of an outbreak in the US due to these patients is not zero, but it’s very close.
So, when faced with Americans infected with Ebola virus in Third World hospitals lacking the resources to provide optimal treatment, the options are to send sufficient medical equipment and staff there to take care of them in Africa or to bring the patients back. By far, the most efficient and economical solution is to bring the patients back to the US, and the risk is minimal. However, fear of contagion remains a powerful force, as noted by Dr. Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota:
Osterholm said he’s been getting calls from editors and reporters in the United States asking why the sick patients are being brought here. “Their reaction to the virus on the fear and panic side is no different than what you see in Africa,” Osterholm says.
“We’re being critical of the West African population for not understanding,” Osterholm says. “I’m thinking, ‘Oh my God, the U.S. senior media doesn’t get it.'”
Or a conspiracy-minded billionaire with bad hair.
It also helps to put Ebola in perspective. Since 1976, Ebola has infected fewer than 5,000 people and killed fewer than 3,000. That’s in Africa, where over 1 billion people live. By contrast, poor, “boring” measles still kills 122,000 people every year and killed over 2 million a year in 1980, before widespread vaccination campaigns. According to the WHO, in 2012, malaria caused an estimated 627,000 deaths, mostly among African children. Also according to the WHO, since the beginning of the AIDS epidemic (which dates back almost as far as the discovery of the Ebola virus), HIV has infected over 75 million and killed 36 million, with approximately 35 million currently living with the infection. None of this means that we shouldn’t take Ebola seriously or that much larger outbreaks couldn’t happen. Nor does noting this difference minimize the deaths of people infected with the disease. We should note from these observations and others, however, that Ebola is unlikely to reach such numbers because it is simply not infectious enough and Ebola outbreaks tend to “burn themselves out” because, unlike HIV or measles (which are also transmissible human-to-human), Ebola virus disease is so rapidly fatal.
In other words, Ebola is a horrible disease, but because it’s so horrible it’s unlikely to kill as many people as diseases we already know about. And it’s not nearly as dramatic as people think. Tara Smith interviewed representatives of Doctors Without Borders several years ago, and this is what one physician, Armand Sprecher, told her:
As for the disease, it is not as bloody and dramatic as in the movies or books. The patients mostly look sick and weak. If there is blood, it is not a lot, usually in the vomit or diarrhea, occasionally from the gums or nose. The transmission is rather ordinary, just contact with infected body fluids. It does not occur because of mere proximity or via an airborne route (as in Outbreak if I recall correctly). The outbreak control organizations in the movies have no problem implementing their solutions once these have been found. In reality, we know what needs to be done, the problem is getting it to happen. This is why community relations are such an issue, where they are not such a problem in the movies.
“Getting it done” is much easier in the US and other developed nations than it is in Africa.
Enter the quacks
Unfortunately, there is no effective treatment for Ebola virus disease yet. All doctors can do right now is to isolate the patient to prevent others from being infected and to support the patient’s physiology with fluids, antibiotics for secondary infections, and blood products to combat the DIC until the patient either manages to clear the infection or dies. There are experimental drugs being tested against Ebola. (David Kroll has nicely summarized the current state of research and development of Ebola drugs, and there is an antibody-based treatment being tested.) Also, there is no vaccine, although efforts to develop one have been fast tracked. The problem in human testing of such a virus, of course, is that Ebola outbreaks are sporadic and difficult to predict. By the time human tests are ready, this latest outbreak could be over, and scientists would have to wait for the next one to test the vaccine. Worse, the economics of developing effective treatments or vaccines against Ebola are prohibitive.
Not surprisingly (or maybe surprisingly, I don’t know), antivaccine activists are already afraid of an Ebola vaccine, even though one hasn’t been approved yet and is unlikely to be for quite some time:

I actually agree with the last commenter. If you’re a nurse and antivaccine, you’re in the wrong career. Please, for the good of your patients, change careers. Seriously, how can you be a nurse and be antivaccine? In any case, resisting the vaccination of healthcare personnel against Ebola is a problem for the future, after such a vaccine has been developed. Meanwhile, in Africa itself, faith healing is being promoted by at least one Nigerian pastor, Ituah Ighodalo, as a means of curing Ebola, including laying on hands, which is a great way to infect oneself with the virus if those hands happen to come into contact with any bodily fluids of the sick and then happen to touch a mucus membrane.
Here in the “developed” world, we have similar claims being made, for instance, in this article entitled Can Gingko and Turmeric Help Stop Ebola? I could have saved them the trouble and said “almost certainly not,” but the author of this article insists on all sorts of handwaving about JAK-STAT signaling p38 MAP kinase and the effect of Gingko and Tumeric on these pathways. It might be worth a detailed deconstruction elsewhere. For now, let’s just say it’s “speculative,” to put it kindly. The editors of Inside Surgery should really know better. Or maybe not. I saw another article on Inside Surgery entitled Can Rife Therapy Help Stop Ebola Disease? Then I saw that the editor of Inside Surgery, L. “Skip” Marcucci, MD, has completed “a fellowship in Integrative Medicine at the University of Arizona” and that he’s also “a formally trained medical acupuncturist.” Well, OK, then. That explains a lot. It also rather saddens me to see an article on a website called Inside Surgery that is not too different from this article by Mike Adams about “natural” cures for Ebola (one of which is based on traditional Chinese medicine).
And that doesn’t even count this amazing bit of pseudoscientific nonsense from Robert F. Cathcart III, MD, who touts himself as an allergist and practitioner of orthomolecular medicine. If you know anything about orthomolecular medicine, you know what’s coming next. Yes, according to Cathcart:
Note that the 2005 epidemic in Angola which was first referred to as an Ebola like virus has now been called the Marburg Virus. It does not make a difference from the point of view of treatment with massive doses of intravenous sodium ascorbate. Both diseases kill by way of free radicals which can be neutralized by massive doses of sodium ascorbate intravenously.
[…]
It does not take a genius to figure out that with the increased bowel tolerance to oral ascorbic acid somewhat proportional to the toxicity of the disease that the most serious infectious diseases would rapidly exhaust all the bodies vitamin C, acute induced scurvy, and cause bleeding all over the body and finally free radical deaths.
That’s right. Cathcart claims that Ebola kills by “free radicals,” which exhaust the body’s supply of vitamin C and induce scurvy, resulting in bleeding. Never mind that Cathcart’s view of the pathophysiology of Ebola virus disease and reality are related only by coincidence, and not even very much then.
As if claims for all sorts of herbal and vitamin treatments for Ebola virus disease weren’t bad enough, there are Kelly and Nate Bailey, the makers of dōTERRA® Essential Oils, who say right on their website:
The reason doctors can’t do anything for viruses is because viruses live inside of your cell’s walls, and medicine particles can’t penetrate those walls. Essential oils, however, have super tiny particles and a makeup that allows them to pass through with no problem! They go in, kill the virus while also stopping the viral cells from duplicating, and all the while boost the immune system so the body can continue to fight for itself. We’ve found that we can kill viral infections in 12-48 hours, depending on how quickly we start using oils.
One notes that doctors can do something for certain viruses, just not this particular virus—yet, hopefully. None of this stops them from playing the martyr from the inevitable charges of quackery that will fly:
Again, I expect an outlash from the western medicine community, and those indignant that I would write about using essential oils against such a ruthless virus. I’m okay with that, because my mission since beginning to share about essential oils is to provide hope where there is none, and to empower people to not let life and illnesses happen to them, but rather arm themselves with the tools to do something.
That’s nice. Actually the “outrage” comes about because the Baileys are peddling quackery that will not help patients with Ebola and capitalizing on the fear of Ebola inspired by the current outbreak to sell essential oils through what sure looks like a multilevel marketing system. They are, however, as nothing compared to what practitioners of The One Quackery To Rule Them All, homeopathy, are doing. Yes, homeopaths are claiming they can cure Ebola.
Given the symptoms of Ebola virus disease, here’s what two homeopaths have proposed as a homeopathic remedy for Ebola:
Dr. Gail Derin studied the symptoms of Ebola Zaire, the most deadly of the three that can infect human beings. Dr. Vickie Menear, M.D. and homeopath, found that the remedy that most closely fit the symptoms of the 1914 “flu” virus, Crolatus horridus, also fits the Ebola virus nearly 95% symptom-wise! Thanks go to these doctors for coming up with the following remedies:
1. Crolatus horridus (rattlesnake venom) 2. Bothrops (yellow viper) 3. Lachesis (bushmaster snake) 4. Phosphorus 5. Merc. cor.
If you are not in the U.S., you must locate your closed homeopathic practitioner and ask him or her to order these remedies for you from Hahnemann Pharmacy, (510) 327-3003 (Albany, California, a suburb of Oakland). If your country’s laws allow you to call a homeopathic pharmacy directly, do so. In any case be sure to find a homeopathic practitioner you can work with. Do not try to take care of yourself without the further education and experience that a homeopath can give you.
You know what they call an Ebola victim foolish enough to rely on these five homeopathic remedies to treat his disease, whether administered by a “real” homeopath or not? Almost certainly dead, that’s what! (Well, at least with a 90% certainty, given that homeopathy is the equivalent of no treatment.) Unfortunately, Derin and Menear are not the only homeopaths recommending this nonsense. Homeopathy has been proposed by clueless homeopaths as a valid means of combatting bioterrorism, chief among the bioterrorism agents being Ebola. For instance, homeopath Joetta Calabrese has suggested:
In the case of Ebola, no conventional treatment or vaccine is available. Fortunately for us, homeopathy has great renown for its healing ability in epidemics.
No. Really. No, it doesn’t, except among homeopaths. Among those health care practitioners rooted in science, not so much. Calabrese proposes a variant of Derin and Menear’s delusional treatment:
If a person is infected, the remedies most commonly used would be the following. One dose every hour, but as the severity of the symptoms decrease, frequency is reduced. If no improvement is seen after 6 doses, a new remedy ought to be considered.
Crotalus horridus 30C – Is to be considered for when there is difficulty swallowing due to spasms and constriction of the throat, dark purplish blood, edema with purplish, mottled skin.
Bothrops 30C – Is the remedy to think of when nervous trembling, difficulty articulating speech, sluggishness, swollen puffy face, black vomiting are present
Lachesis mutus 30C ,– when there’s delirium with trembling and confusion, hemorrhaging in any area, consider this remedy. Often, the person cannot bear tight or constricting clothing or bandages and feels better from heat and worse on the left side.
Mercurius corrosivus 30C, – For copious bleeding, better when lying on the back with the knees bent up, delirium, headache with burning cheeks, photophobia, black swollen lip, metallic, bitter or salt taste in mouth.
Secale cornutum 30c,– For thin, slow, painless oozing dark hemorrhage with offensive odor, cold skin and tingling in the limbs. The individual wants to be uncovered and feels WORSE from motion.
Echinacea 30C – For when there’s sepsis or blood poisoning, fetid smelling discharges and enlarged lymph nodes.
Homeopathy is an ideal medical stratagem for survivalists, homesteaders and anyone wanting to be self-reliant in any situation.
I thought this might be a joke, but it’s not. All you have to do is to peruse the rest of Calabrese’s website to realize that she actually believes these things. Calabrese also pimps her forthcoming book, The Survivalist Guide to Homeopathy. In any event, all of these remedies, being 30C dilutions, are nothing more than water, likely soaked into sugar pills. I still can’t figure out why homeopaths take their water, press it into sugar pills, and then let them dry out. Why not just administer the water with a bit of salt? In that case, it might at least have a chance to contribute to the rehydration of a vomiting and bleeding patient.
Of course, these recommendations aren’t just the delusional ravings of pseudoscience-believing homeopaths? (Well, actually, they are.) Homeopaths try to show there’s “science” behind them. For example, there’s even a paper in the British Journal of Homeopathy (OK, so it’s not actually science) entitled “Sicarus (Six-Eyed Crab Spider): A homeopathic treatment for Ebola haemorrhagic fever and disseminated intravascular coagulation?” Shockingly, I found this ridiculous paper hosted on a personal page on the Indiana University website. In any case, it’s not just Ebola. Homeopaths are deluded enough to think that they can treat potential bioterrorism agents such as anthrax (Anthracinum and Arsenicum album), smallpox (Variolinum, Malandrinum, Sarsparilla, Thuja, Baptisia (Pestinum and Crotalus horridus for hemorrhagic plague; Lachesis, Arsenicum album for bubonic plague; Phosophorus for pneumonic plague), and Botulism (Botulinum and Gelsemium, Arsenicum album, Belladonna Alternate).
Meanwhile, on Twitter, the homeopathy supporters were out in force, and the WHO tweeted:
There is no evidence base that #homeopathy can cure #Ebola. Severely ill patients require intensive supportive care http://t.co/itpATExjBk
— WHO (@WHO) July 31, 2014
It’s sad and also evidence of how loudly homeopaths have been making the claim that homeopathy can cure Ebola virus disease that the WHO felt obligated to state this simple fact. Not surprisingly, the WHO got responses like:
@Skepticat_UK @WHO Applied Research in Evidence-based Homeopathy for 29 medical conditions http://t.co/7SK8Gc26g3
— EvidenceBased Hpathy (@DrNancyMalik) July 31, 2014
And:
WHO on Ebola "No specific treatment is available" and no comments about #homeopathy pro or con. http://t.co/hzDvGhEtzD
— Laurie J. Willberg (@LaurieJWillberg) August 1, 2014
This response from Laurie J. Wilberg, who was told that the burden of proof is not on homeopathy critics, says it all:
#homeopathy @BrownBagPantry The burden of proof concept is a legal one: the accuser needs to prove their case, as in malpractise.
— Laurie J. Willberg (@LaurieJWillberg) August 2, 2014
Once again, homeopaths get a basic concept of science and medicine wrong. Science is not the legal system. It is thus not up to skeptics to prove that homeopathy doesn’t work. It’s up to homeopaths to prove it does. Indeed, it’s tempting to propose that a homeopath infect himself with the blood of an Ebola victim, wait until the flu-like symptoms start, and then cure himself with homeopathy. I say “tempting” because I won’t really propose it. Some homeopath might actually try it. So if you’re a homeopath reading this, please don’t do something like that. And, if you’re in Africa (or anywhere else) and are unfortunate enough to be infected, please, please, please, please, don’t rely on homeopathy or other quackery for your treatment. If you want to quadruple your chances of surviving (10% chance of survival to over a 40% chance), don’t do it. Seek the best science-based medical care you can find.
Conclusions
This is the largest Ebola virus disease outbreak recorded thus far. Because Ebola virus (particularly the Zaire strain) produces such a nasty disease that kills more than 50% of those infected, even when optimal medical care is available, and over 90% of the untreated, it’s natural that fear and misinformation are running rampant, be they peddled by faith healers, homeopaths, or rich old guys with bad hair and an overinflated opinion of their own knowledge. It’s important for us to remember here in the US that the likelihood of an outbreak due to bringing back two patients with Ebola virus disease is incredibly small, and that conditions here in the US and other developed nations are such that it is unlikely that such an outbreak, even in the unlikely event that it happened, would spread very far, given the differences in medical care, availability of resources, and differences in funeral practices. That’s not to say we shouldn’t be vigilant, but there is really nothing particularly unusual about Ebola virus other than the rapid onset and severity of the disease it causes.
As for Africa, the problem is, as is usually the case in poor and less developed countries, resources. Doctors Without Borders/Médecins Sans Frontières are stepping up efforts to bring real medical care to the victims in Africa, constructing a clinic that looks like this:
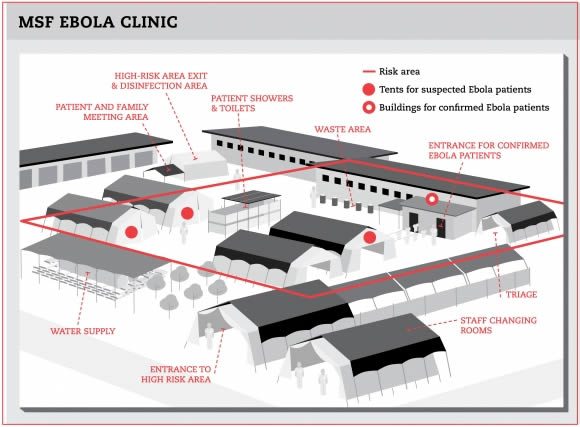
But:
Already stretched beyond capacity in Guinea and Sierra Leone, MSF is able to provide only limited technical support to the Liberian Ministry of Health. MSF has set up an Ebola treatment center in Foya, in Lofa county in northern Liberia, where cases have been increasing since the end of May. After the initial set up, MSF handed over the management of the center to nongovernmental organization Samaritan’s Purse on July 8.
WHO is also contributing, as is Samaritan’s Purse. If there’s one thing that’s sure, more resources and more effort on the part of developed nations will be required to bring these outbreaks under control and save as many lives as possible. If there’s another thing that’s sure, it will require science-based medicine, not quackery like homeopathy, to succeed.