{kind=link}
A 3-D image of the ascorbic acid (vitamin C) molecule.
Somehow, I’ve a feeling we’re not in Kansas anymore—except that we are, as you will soon see.
Because I’m the resident cancer specialist on this blog, it usually falls on me to discuss the various bits of science, pseudoscience, and quackery that come up around the vast collection of diseases known collectively as “cancer.” I don’t mind, any more than my esteemed colleague Dr. Crislip minds discussing infectious diseases and, of course, vaccines, the most effective tool there is to prevent said infectious diseases. In any case, there are certain things that can happen during a week leading up to my Monday posting slot on SBM that are the equivalent of the Bat Signal. Call them the Cancer Signal, if you will. One of these happened last week, thus displacing that post I’ve been meaning to write on a particular topic once again. At this rate, I might just have to find a way to write an extra bonus post. But not this week.
In any case, this week’s Cancer Signal consisted of a series of articles and news reports with titles like:
- Vitamin C shows promise as cancer therapy (FOX News).
- Researchers establish benefits of high-dose vitamin C for ovarian cancer patients (Kansas University Medical Center press release).
- Vitamin C injections ease ovarian-cancer treatments (Nature).
- Vitamin C keeps cancer at bay, US research suggests (BBC).
- Vitamin C May Help Cancer Treatment, Study Finds (NBC News).
- IV Vitamin C Boosts Chemo’s Cancer-Fighting Power? (WebMD).
- Vitamin C as cancer treatment? High doses boost chemotherapy in study (LA Times).
These stories, to varying degrees, miss the point. Unfortunately, I confess that I wasn’t able to help at least one of them. A reporter happened to leave me a message Tuesday morning, which is my operating room day, and I didn’t have time to read the paper and to get back to her before her deadline. That paper, by the way, appeared in Science Translational Medicine from Jeanne Drisko and Qi Chen from, yes, Kansas University Medical Center, and indicates to me that STM‘s standards are slipping. But then, STM did publish a rather credulous paper by our old friend Ted Kaptchuk on placebos; so maybe I expect too much. Clearly STM appears to be looking for more papers on “complementary and alternative medicine” (CAM) or “integrative medicine.”
Be that as it may, a typical story describes the recently published research thusly:
People with ovarian cancer who receive high-dose vitamin C injections are less likely to report toxic side effects from chemotherapy than people who had chemotherapy alone, according to the results of a small clinical trial.
The study, published today in Science Translational Medicine1, was too small to assess whether the combination of chemotherapy and vitamin C combats cancer better than chemotherapy alone. But accompanying work in mice suggests that the two treatments could be complementary.
The results are the latest salvo in long-running controversy over the use of vitamin C against cancer. Early studies championed by Nobel-prizewinning chemist Linus Pauling in the 1970s suggested that vitamin C could help to fight tumours2. But larger clinical trials failed to substantiate those claims3, 4.
With the spin, from another typical story, being:
One potential hurdle is that pharmaceutical companies are unlikely to fund trials of intravenous vitamin C because there is no ability to patent natural products.
“Because vitamin C has no patent potential, its development will not be supported by pharmaceutical companies,” said lead researcher Qi Chen.
“We believe that the time has arrived for research agencies to vigorously support thoughtful and meticulous clinical trials with intravenous vitamin C.”
Yes, indeed. The same old tropes are there, from the claim that vitamin C has usefulness in treating cancer to the old ascorbate warriors’ lament that there’s no patent potential in vitamin C, which means that pharmaceutical companies don’t want to invest money into doing science and clinical trials on it because there’s no profit potential. Of course, I’ve written fairly extensively about vitamin C and cancer before, using it as an example of how even a two-time Nobel Prize winner like Linus Pauling could fall prey to bad science when he wandered outside of his area of expertise. Every so often these stories come up suggesting that Linus Pauling has somehow been vindicated and how vitamin C is the greatest thing for cancer patients since surgeons first discovered that some cancers could be cured by cutting them out. Inevitably, I have to throw cold water on such claims. No, Linus Pauling has not been vindicated, and, no, vitamin C for cancer is not all that great.
Also, no, contrary to what critics say, I’m not close-minded about vitamin C and cancer. Unlike so many “alternative” cancer treatments, it’s actually a chemical and, at the doses used by alternative cancer practitioners, a drug. There’s even a (very) weakly plausible mechanism by which it might work. However, in vitro, the concentrations required to provide even a whiff of a hint of antitumor activity are ridiculously high, and the same is true in animal models. Let’s just put it this way. Imagine a pharmaceutical company had developed a compound with properties identical to that of vitamin C and could thus own the complete patent on it as a drug. Given the ridiculously high concentrations and doses required in preclinical models to demonstrate a hint of antitumor activity, that pharmaceutical company would probably retire that compound before even the animal model stage because, as I like to put it, getting any useful anticancer activity out of it would be such a long run for a short slide. A good drug for cancer is, at the very minimum, active at low or reasonable concentrations against the cancer cells being targeted, and vitamin C fails miserably on that count. Worse, there are at least indications that in some cases vitamin C might interfere with chemotherapy.
Vitamin C in Kansas
So does this study change my opinion? Not really. It suggests there might be some utility for ascorbate (vitamin C) against ovarian cancer, but that ascorbate therapy for cancer still remains at best a long run for a very short slide right into the gloved ball of reality to be tagged for a third out. (OK, I’ll stop with the baseball analogies.)
The dubious reasoning begins right in the first paragraph, with the authors’ justification for “re-examining” ascorbate as a cancer therapy. Basically, they point out that the pharmacokinetics of oral ascorbate dosing is different from intravenous dosing, to the point where it is possible to obtain serum ascorbate concentrations of 10 mM (millimolar). To give those of you who aren’t chemists a rough comparison of just how high that concentration is, most cancer drugs have active concentrations in the nanomolar (nM) to micromolar (uM) range, in other words, a thousand-fold to a million-fold lower than 10 mM. For example, the IC50 (the concentration that leaves only 50% of cells alive) for paclitaxel is in the 2.5 to 7.5 nM nM range, depending upon the cell line, and 50 nM is considered a good, effective therapeutic concentration. You get the idea. You need a lot of ascorbate:
By contrast, when ascorbate is injected intravenously, tight control is bypassed and pharmacologic concentrations of ascorbate are established until excess ascorbate is excreted by kidney. Plasma concentrations greater than 10 mM are safely sustained in humans for ~4 hours (10–13). When patients have normal renal function and glucose-6-phosphate dehydrogenase (G6PD) activity, toxicity is minimal even with intravenous doses as high as 1.5 g/kg, equivalent to 105 g for a 70-kg person (2, 12). These data indicate that intravenous administration of pharmacologic ascorbate doses is safe and similar to drug administration. Therefore, the effect of ascorbate in cancer treatment is worth reexamining.
These are huge doses, consistent with previous experiments in mice with a xenograft from an ovarian cancer cell line (Ovcar5) in which 4 g/kg of ascorbate was administered twice daily for a total of 8 g/kg/day. The result was an inhibition of xenograft growth of around one-third after 30 days. Results for a pancreatic cancer cell line and a glioblastoma cell line were only marginally better.
The authors did several cell culture studies in which ovarian cancer cell lines were treated with ascorbate and various chemotherapeutic agents. The authors reported an IC50 of between 0.3 and 3.0 mM, which is still incredibly high for an anticancer drug. The authors blithely write that this is “easily achievable” with IV ascorbate. Maybe so, but given the quantities involved, if you’re going to use a drug that requires such high plasma concentrations to have activity, that activity had better be awesome. None of the activity shown in this paper can be characterized as being particularly impressive. Worse, the authors, despite testing several ovarian cancer cell lines, only tested one non-tumorigenic immortalized ovarian line, HIO-80, and, finding that the IC50 to kill HIO-80 cells was much higher than all but one of the other cell lines (SHIN3), proclaimed a high degree of specificity for cancer. Moreover, HIO-80 cells are hardly “normal.” They likely contain BRCA1 mutations. Finally, the authors only used one assay for proliferation, the MTT assay. This particular assay is very popular (I use it in my lab not infrequently) because it is faster and easier than counting viable cells and also allows for large experiments using 96-well plates. However, the MTT assay depends on the metabolism of cells to produce a dye that is detected. The amount of light absorbance due to the dye is assumed to be proportional to the number of viable cells. Usually, this assumption is reasonable accurate, but lots of things can interfere with this and render that assumption incorrect. For instance, one wonders if very high concentrations of ascorbate can interfere. I’d want to see a control demonstrating that the MTT results correspond to cell number.
In other words, if I were a reviewer for this paper, not so fast, I’d have said. I want to see the results for at least a couple of more non-tumorigenic cell lines and a control validating the MTT in the presence of so much ascorbate (even if just a reference) before I’ll let you conclude that the effects of ascorbate are highly specific for cancer over normal ovarian cells. At the very least, I wouldn’t have considered it unreasonable to ask for a couple more non-tumorigenic ovarian epithelial cell lines to be tested.
In any case, the authors also did some mechanistic studies, the results of which were consistent with the activity of ascorbate in cancer requiring the production of peroxide (H2O2), as H2O2 scavengers blocked the effect. They also did a series of experiments that indicated synergy between ascorbate and carboplatin, a common chemotherapy drug used in ovarian cancer. One area that, as a reviewer, I’d have gotten on the authors’ case was the series of xenograft experiments using ovarian cancer cell lines implanted under the skin of immunodeficient mice, specifically this part:
Two-tailed Student’s t test was performed for comparison of treated groups to control group in the cell and animal experiments, as well as for toxicity comparison between chemotherapy group and chemotherapy + ascorbate group.
No, no, no, no, no! This is some pretty basic stuff here. There are eight different experimental groups, and the authors didn’t control for multiple comparisons, as far as I am able to tell. Pair-wise two-tailed t-tests are not the correct statistical test for determining statistical significance in such a case; likely some form of ANOVA would be, given that the dataset consists of tumor weights and volumes of ascites, the latter being a common estimate of ovarian tumor burden in mouse models. Some form of ANOVA, likely factorial ANOVA, would have been the proper test, given that there are combinations of three drugs being used. Whatever the correct test is (and I’ll leave that to the statisticians out there), I know that Student’s t-test isn’t it, and that using Student’s t-test will often produce “false positives” that appear statistically significant but aren’t.
All of this, however, is the warm-up to the part of the study that got it noticed, namely the clinical trial. Without the clinical trial, this would have been yet another in vitro and animal study of high dose vitamin C that provokes a collective yawn throughout the scientific community. The clinical trial itself was a randomized prospective phase I/IIa clinical trial, which means that the trial was designed to combine an evaluation of toxicity with a pilot study to evaluate efficacy and safety. Its primary objective was to “determine the safety of high-dose intravenous ascorbate when combined with first-line chemotherapy paclitaxel and carboplatin in the treatment of advanced-stage ovarian cancer,” along with evaluation for toxicity. Consequently, the two groups were (1) standard carboplatin plus paclitaxel (Cp + Pax) and (2) carboplatin plus paclitaxel plus ascorbate (Cp + Pax + AA) according to this design:
Ascorbate dose for the Cp + Pax + AA arm was established via dose escalation initiated at 15 g per infusion titrated up to a therapeutic range of 75 or 100 g per infusion, with a target peak plasma concentration of 350 to 400 mg/dl (20 to 23 mM) (12, 13). The ascorbate infusion was given at a rate of 0.5 g/min, and 400 mg of magnesium chloride (Wellness Pharma) was supplemented into each infusion. Once the therapeutic dose was established, the Cp + Pax + AA group received ascorbate two times per week in conjunction with chemotherapy for 6 months, and injectable ascorbate was continued for another 6 months after chemotherapy completion.
In addition, the authors noted:
Two subjects voluntarily withdrew from the Cp + Pax arm before treatment commenced because they wanted intravenous vitamin C, and they were excluded from data analysis. Two subjects were removed from the Cp + Pax + AA arm because they were noncompliant with tobacco use, and one was removed from the Cp + Pax + AA arm after in vitro cytotoxic assays detected that her tumor cells were resistant to all chemotherapy. These three subjects received doses of chemotherapy and ascorbate, so their adverse events were counted, but they were excluded from the survival report (table S3). Double blinding was used at enrollment and randomization, but was not maintained during the treatment because no placebo control was used.
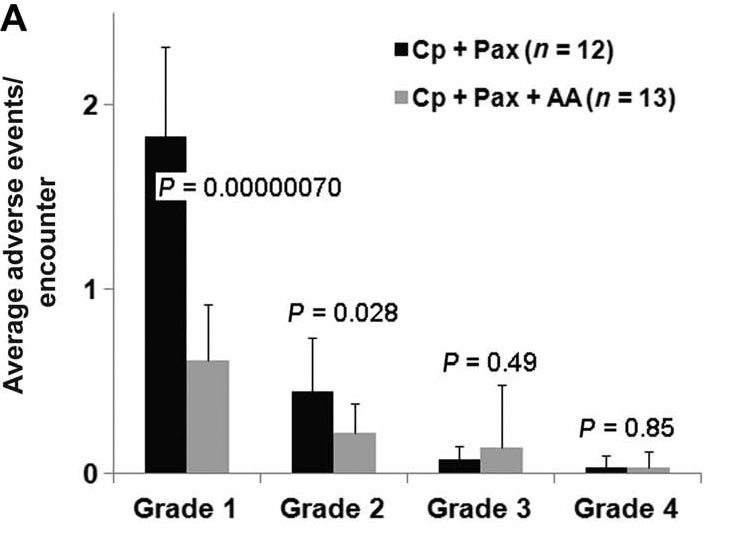
So what we have here is a small clinical trial with a 19% dropout rate that wasn’t even blinded. It reported zero difference in overall survival (both were, as one would expect for ovarian cancer at this stage, abysmal), and zero statistically significant difference in time to relapse/progression. In all fairness, there would have had to have been an enormous effect to produce a statistically significant effect on survival or progression in such a small study, but these are the two “hard” endpoints that would be least affected by the lack of blinding, although one notes that time to progression could be affected by lack of blinding when the definition depends on interpreting scans. It’s also hard not to note that the differences in toxicities are all in the mildest reported toxicities, grades 1 and 2 (out of a scale of 1 to 5, with a score of 1, which denotes mild toxicity that requires no intervention to 5, which is death). There were no statistically significant (or even close to statistically significant) differences in toxicities graded 3 or 4, which are the most troubling kind. Take a look at the graph:
Then, when the authors broke it down, this is what they found:
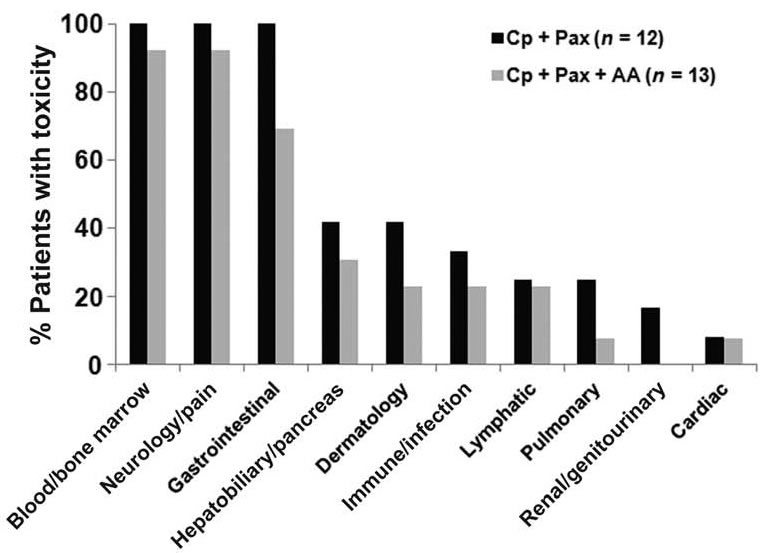
Notice the types of complaints with the biggest difference: gastrointestinal (which usually includes symptoms such as nausea, abdominal pain; dermatology, which usually includes itching and rashes of various types); pulmonary, which often includes symptoms of shortness of breath, cough, and the like, and renal/genitourinary, which is the only one that’s less objective. So, basically, what we have is a study that found no benefit in overall survival or time to progression (not unexpected for such a small study). More importantly, contrary to the way it was trumpeted to the press, the decrease in adverse events actually observed was limited to the least serious adverse events (grade 1 = minor, causing no limitation of activity, no intervention required; grade 2 = moderate, some limitation of activities, minimal intervention indicated) with the most potential to be subject to reporting bias, which in the context of a trial that is not blinded makes the difference reported probably meaningless. In other words, this was probably a negative study, a long run for a short slide, indeed. (Sorry, couldn’t resist.)
There’s no woo like Kansas woo
I thought it might be interesting to provide SBM readers with a bit of context about the institution from which this rather pointless study emerged. The reason that this particular study rose to the level that I thought I had to blog about it was not because a reporter contacted me about it. Rather, one of the key investigators on the study, Jeanne Drisko, recently appeared on a web chat, Can Alternative and Conventional Medicine Get Along?
This chat featured, in addition to Dr. Drisko, Dr. Josephine Briggs, the current director of the National Center for Complementary and Alternative Medicine (NCCAM) as well as an associate editor from Science Translational Medicine, Yevgeniya Nusinovich, M.D., Ph.D., who served as moderator. Dr. Jeanne Drisko’s titles include Director, KU Integrative Medicine and the Riordan Endowed Professor of Orthomolecular Medicine, and, consistent with her involvement in this study, KUMC offers its patients high dose vitamin C for cancer. The video itself was standard fair, discussed by a certain “friend,” where the Trial to Assess Chelation Therapy was incorrectly touted as a success warranting further study for chelation therapy for heart disease. However, what tweaked me to write this was Dr. Drisko’s mention at the end of her “hot off the presses” study of high dose vitamin C.
Personally, I found it instructive to take a look at the website for Dr. Drisko’s home department, the University of Kansas Medical Center Integrative Medicine Program. The first thing I noticed when I perused its website was this:
Nourishing the whole person — body, mind and spirit — and stimulating the body’s natural healing response, is our mission at KU Integrative Medicine. We combine the best therapies from conventional medicine with our integrative medicine approach, to form a comprehensive system of biomedical care.
From a patient’s very first visit with us, we attempt to uncover the underlying story that set the patient on their journey from wellness to disease. We listen. Based on our findings, we tailor a plan for each individual patient based on their lifestyle, their needs and their preferences. We consider the patient an integral part of the treatment team, and encourage patients to take control of their medical care.
Practitioners at KU Integrative Medicine include physicians, a naturopathic doctor, nurses, certified neurofeedback technicians and registered dietitians. We hope that you want to learn more about us, our services, and how we can help you forge a new path to healing and wellness.
Because Integrative Medicine attempts to dig deeper, very specialized lab work is often ordered. This also enables us to personalize your care and cater to your biochemical individuality.
Yes, it’s the same old tropes. KU claims to combine the “best of both worlds”. Unfortunately, whenever I hears that phrase, there’s another “best of both worlds” that I can’t help but think of, and it involves assimilation. Sadly, in this case the assimilation appears to involve science-based medicine being assimilated by quackery. After all, there’s a naturopath there, and naturopathy is nothing more than a cornucopia of pretty much every quackery imaginable under the sun, be it homeopathy, traditional Chinese medicine, “energy healing” modalities, and, of course “detoxification.”
However, it isn’t the fact that there’s a naturopath based at an academic medical center promising to “listen” and provide “individualized care.” That’s pretty much par for the course. In fact, it’s probably hard to find an “integrative medicine” program that doesn’t claim to “listen” and provide “personalized” or “individualized” care. Nor was I particularly surprised to see “healing foods” or neurofeedback. Nor was I even particularly surprised to see that KU offers detoxification. No, what caught my interest was the fact that KU offers “oral and intravenous vitamin and mineral therapies,” as in IV vitamin C being offered at a major academic medical center.
Orthomolecular medicine? Yes, Orthomolecular medicine, a form of quackery that posits that if the body needs some vitamins and minerals that more, more, more would be better. Indeed, it’s the quackery espoused by Linus Pauling that features, in particular, high dose vitamin C as one of its favored modalities. And guess what? The integrative medicine program at KU offers high dose intravenous vitamin C to its patients. It even has a FAQ about vitamin infusions on its site. What’s really scary, however, is this:
How do I know if the intravenous vitamin C therapy will work for my cancer?:
Each individual responds differently, and we can’t predict how different tumor types will react. A PET scan is usually a guidepost. If the PET is positive, the tumor usually responds to the vitamin C. If the PET is negative but there is active tumor present, the vitamin C is less effective in most cases. Vitamin C works best in the early stages of cancer when used in conjunction with chemotherapy or radiation. They will only consult patients who are also following along with a traditional oncologist.
It’s even said that there are “no contraindications to giving intravenous vitamin C with any chemotherapy when proper protocol is followed” and that the only chemotherapy that intravenous vitamin C doesn’t work with is methotrexate “because of urine pH requirements.” Upon what evidence is this based? Well, before it was minimal. One study examined on intravenous vitamin C. It was an in vitro and xenograft study (i.e., preclinical), and Dr. Drisko wasn’t even the corresponding author. Another study was a case series involving two patients. The third was a review article. None were particularly impressive. After this study, the evidence still remains unimpressive.
But that’s not all.
It turns out that Dr. Drisko has a rather dubious honor (dubious, at least to me; no doubt she doesn’t consider it so). I’m referring to her title of Chair of the Alliance for Natural Health USA. Yes, ANH-USA is one of the premier “health freedom” organizations in this country, “health freedom” in reality meaning advocating for freedom from pesky government regulation that might interfere with the selling of supplements. She’s also an advisory board member for the Institute for Functional Medicine. Functional medicine, a nebulously defined “specialty,” is pure pseudoscience, as has been described before. Perhaps the most famous practitioner of “functional medicine” is Dr. Mark Hyman, who promotes it under the title of “Ultrawellness.” In fact, the sad thing is this:
Dr Drisko teaches a fourth-year medical student elective in integrative medicine along with other teaching duties to 1st and 2nd year students, nursing students, and practicing physicians. A fellowship program in integrative medicine for primary care physicians began in 2008 under Dr Drisko’s leadership. She was nominated by the University of Kansas Medical Student Assembly to receive the Rainbow Award for Excellence in Teaching the Art of Medicine.
Dr Drisko serves the School of Medicine at KU Med by sitting on multiple committees, provides guidance for the State of Kansas on topics in integrative medicine, and participates at the national level on CAM initiatives. Dr Drisko is a member of the Kansas Cancer Research Institute and an advisory board member of the General Clinical Research Center at the University.
Meanwhile, the website for KUMC helpfully tells patients:
Will my insurance cover the costs of the vitamin C infusions?
They will not cover them in most cases. Alternative medicine doctors must use billing codes that are not usually accepted by insurance companies. And because vitamin C infusions are not FDA approved, insurance companies are not inclined to cover costs. Vitamin C infusions range in price from $125.00 to $160.00.
Good to know.
Yes, you read that right. An academic medical center is trying to facilitate patients going to alternative medicine practitioners who administer high dose vitamin C.
Depressingly, Dr. Drisko is intimately involved in the education of the next generation of doctors in Kansas and has started an “integrative medicine” program for primary care physicians, the better to “integrate” woo into real medicine. This latest highly unimpressive study being touted as evidence that high dose intravenous ascorbate/vitamin C therapy is anything other than a long run for a short slide (oops, there I go again!) is merely part of the campaign to insinuate quackademic medicine even more firmly into the mainstream than it has regrettably already succeeded in doing.