
{kind=link}
Those of us who have been writing about medical misinformation, disinformation, and quackery are very familiar with a certain type of story or anecdote frequently presented by those who have lost faith in science-based medicine to argue for unproven and unscientific medical claims. One example is the person with a longstanding and often vague constellation of health symptoms that conventional medicine has not dealt with well and often cannot explain who becomes convinced that the cause is something like chronic Lyme disease, “adrenal fatigue” (as opposed to the real disease adrenal insufficiency), “electromagnetic sensitivity,” or any of the number of other fake diagnoses that quacks use to offer these patients hope when conventional medicine is struggling. Besides the inexplicable symptoms, a key component of these anecdotes is that “conventional” medical doctors are portrayed as, at best, ignoring their stories or, at worse, being dismissive of their symptoms and suffering, sometimes haughtily and even contemptuously so. (Worse, sometimes they are not exaggerating by much.) Before the pandemic, another common example of these sorts of stories consisted of parents—like Jenny McCarthy—who were utterly convinced that vaccines had been the cause of their child’s autism and treated even gentle attempts to persuade them that copious existing science does not support such a link angrily, as though doctors were denying their knowledge. Such stories, unsurprisingly, make for compelling human-interest stories and long before the pandemic sometimes tripped up journalists into giving too much credence to pseudoscientific diagnoses like CLD, vaccine-induced autism, and electromagnetic insufficiency, often based on the question, “What else could be causing these symptoms?”
Those of you who read the New York Times this weekend might sense where I’m going with this introduction, because featured prominently in the Sunday Times (but published on Friday) is an article by Apoorva Mandavilli that is being trumpeted by a number of antivaxxers as “vindication.” Entitled Thousands Believe Covid Vaccines Harmed Them. Is Anyone Listening? the story also sports the tagline, All vaccines have at least occasional side effects. But people who say they were injured by Covid vaccines believe their cases have been ignored. Of course, anyone who is familiar with Betteridge’s Law of Headlines knows that usually the answer to a question in the title of a news article is no, and, although this report doesn’t state a clear “no” as the answer to the question, it does clearly suggest that the answer is much closer to “no” than to “yes.”
Therein lies the first problem. This story is framed in the way that I’ve seen so many articles going back years and years about vaccine-induced autism, CLD, electromagnetic sensitivity,” and the like framed in the past: Primarily as a human-interest story about suffering people bravely trying to convince an uncaring establishment (be it medical or otherwise) of The Truth that no one wants to admit. In using this framing, Mandavilli and the NYT present stories and facts in a context designed to lead you to suspect that “They” are covering something up about COVID-19 vaccine injuries.
Before I go on, let me just emphasize that no one—and I mean no one—says that serious vaccine injuries don’t or can’t happen. Rather, science shows that, other than local reactions, fevers and chills, and other brief symptoms, severe adverse reactions to vaccines tend to be quite rare. Moreover, I have long said that those who suffer genuine vaccine injury should be recognized as having suffered such an injury and appropriately compensated. What Mandavilli’s article gets right is that, unlike the Vaccine Injury Compensation Program, which applies to all FDA-approved vaccines, vaccines like like the COVID-19 vaccines, which were not fully FDA-approved but instead received an emergency use authorization (EUA) are covered by the far stingier Countermeasures Injury Compensation Program. For the CICP, the burden of proof is much higher than it is for the VICP, where the level of proof is the same as it is for civil lawsuits (50% and a feather, as some put it) and the rules are set up to make it easier for complainants to access the system, to the point of the VICP will reimburse complainants for their legal costs and reasonable costs of bringing cases before the Vaccine Court the special court set up to hear such cases. Moreover, VICP only requires that such cases be heard first by the Vaccine Court; if a claim is denied, federal courts are still available.
As Mandavilli notes about the CICP, in contrast:
The federal government has long run the National Vaccine Injury Compensation Program, designed to compensate people who suffer injuries after vaccination. Established more than three decades ago, the program sets no limit on the amounts awarded to people found to have been harmed.
But Covid vaccines are not covered by that fund because Congress has not made them subject to the excise tax that pays for it. Some lawmakers have introduced bills to make the change.
Instead, claims regarding Covid vaccines go to the Countermeasures Injury Compensation Program. Intended for public health emergencies, this program has narrow criteria to pay out and sets a limit of $50,000, with stringent standards of proof.
It requires applicants to prove within a year of the injury that it was “the direct result” of getting the Covid vaccine, based on “compelling, reliable, valid, medical, and scientific evidence.”
The program had only four staff members at the beginning of the pandemic, and now has 35 people evaluating claims. Still, it has reviewed only a fraction of the 13,000 claims filed, and has paid out only a dozen.
Dr. Ilka Warshawsky, a 58-year-old pathologist, said she lost all hearing in her right ear after a Covid booster shot. But hearing loss is not a recognized side effect of Covid vaccination.
The compensation program for Covid vaccines sets a high bar for proof, she said, yet offers little information on how to meet it: “These adverse events can be debilitating and life-altering, and so it’s very upsetting that they’re not acknowledged or addressed.”
I doubt that there are any vaccine advocates who don’t agree that the CICP should be reformed and fully funded and that COVID-19 vaccine injuries should be treated like any other vaccine injury adjudicated under the VICP. Of course, as an aside, I can’t help but note that antivax lawyers have long hated the VICP and the Vaccine Court because, even though it’s a guaranteed payday for them, win or lose, in terms of hourly charges, these lawyers suing for “vaccine injury” want to play the lottery and risk not getting paid in hopes of getting a 30% contingency fee from multimillion dollar judgments. The reason I mention this is that antivaxxers might not be too thrilled if COVID-19 vaccine injury cases from before the vaccines were granted full FDA approval and were being administered under an EUA were shifted to the Vaccine Court. However, it would be much better for those who might have been injured by COVID-19 vaccines than the CICP. (Regular commenter and professor of law Dorit Reiss wrote about the CICP and its problems nearly three years ago at another blog, agreeing that, “Ideally, I would like to see COVID-19 vaccine liability moved to the routine compensation program.”)
Unfortunately, despite making some good points (another of which I will discuss later), the story frames the issue in such a way as to lead to an impression that those who might have suffered injury from COVID-19 vaccines are not being taken seriously. That impression permeates the framing of this article, which is bookended by the telling of a sad story.
Lead with the heart
Mandavilli’s story, as nearly all such stories seem to do, with a human interest story, an anecdote that in these sorts of stories is meant to put a human face on a problem and be representative of the problems being reported. In this case, it is a neuroscientist named Michelle Zimmerman, who suffered puzzling symptoms after receiving the Johnson & Johnson COVID-19 vaccine. Remember that the J&J vaccine was not based on the mRNA technology used for the Pfizer and Moderna vaccines that were administered to the vast majority of vaccinees, but, rather, was based on an adenoviral vector designed to express (make) the SARS-CoV-2 spike protein as the antigen:
Within minutes of getting the Johnson & Johnson Covid-19 vaccine, Michelle Zimmerman felt pain racing from her left arm up to her ear and down to her fingertips. Within days, she was unbearably sensitive to light and struggled to remember simple facts.
She was 37, with a Ph.D. in neuroscience, and until then could ride her bicycle 20 miles, teach a dance class and give a lecture on artificial intelligence, all in the same day. Now, more than three years later, she lives with her parents. Eventually diagnosed with brain damage, she cannot work, drive or even stand for long periods of time.
“When I let myself think about the devastation of what this has done to my life, and how much I’ve lost, sometimes it feels even too hard to comprehend,” said Dr. Zimmerman, who believes her injury is due to a contaminated vaccine batch.
The story is bookended with this followup on Dr. Zimmerman:
One of her therapists recently told her she might never be able to live independently again.
“That felt like a devastating blow,” Dr. Zimmerman said. “But I’m trying not to lose hope there will someday be a treatment and a way to cover it.”
In fairness, right after introducing Dr. Zimmerman, Mandavilla notes:
The Covid vaccines, a triumph of science and public health, are estimated to have prevented millions of hospitalizations and deaths. Yet even the best vaccines produce rare but serious side effects. And the Covid vaccines have been given to more than 270 million people in the United States, in nearly 677 million doses.
All of this is true, but when it is mentioned after an anecdote like that of Dr. Zimmerman, the framing comes across very much as, “Yes, but?”
Regardless, my heart goes out to Dr. Zimmerman and the others discussed in this story, as it does to all such patients suffering from a constellation of debilitating symptoms that her doctors can’t explain and have not been able to deal with well. I hope that she finds what is going on and a treatment that can get her as close as possible back to a normal life. As someone who late in life discovered physical fitness and, like her, can ride my bicycle over 20 miles, I just can’t imagine what it would be like to lose the ability to do that and so many other routine daily activities. That being said, this story suffers from just mentioning that she blames her symptoms on a contaminated batch of J&J vaccine without giving some context. I vaguely remembered a story about contaminated COVID-19 vaccines from early in the rollout, but didn’t remember any details. So I clicked on the link, which goes to a NYT story from three years ago entitled, The F.D.A. tells Johnson & Johnson that about 60 million doses made at a troubled plant cannot be used. What was the contamination? According to the story:
More than 100 million doses of Johnson & Johnson and at least 70 million doses of AstraZeneca were put on hold after Emergent discovered in March that its workers had contaminated a batch of Johnson & Johnson’s vaccine with a key ingredient used to produce AstraZeneca’s. Federal officials then ordered the plant to pause production, stripped Emergent of its responsibility to produce AstraZeneca’s vaccine and instructed Johnson & Johnson to assert direct control over the manufacturing of its vaccine there.
What was that “key ingredient”? The story didn’t say; so I tried to do some Googling. An article in Fierce Pharma wasn’t any more revealing, although it did make me wonder if any of the contaminated batches, whatever it was that they were contaminated with, ever made it out to be administered. The reason is that something described as a “key component” of the J&J vaccine and the AstraZeneca vaccine (another COVID-19 vaccine based on an adenoviral vector) were being manufactured in the same plant and somehow batches of the J&J vaccine had apparently been contaminated with this “key component” of the AstraZeneca vaccine. Since the two vaccines are very similar. Moreover, there were a number of investigations of the mixup at a subcontractor, Emergent BioSolutions, where the two vaccines were being manufactured, which showed that Emergent had had a history of red flags in terms of its quality control and manufacturing processes dating back to before it got the contracts to manufacture vaccines under the “Warp Speed” initiative, notably its role as a key supplier before the pandemic of anthrax vaccine for the Strategic National Stockpile. Moreover, from what I’ve read, it seems that what happened is that the contamination was actually of this key component of the J&J vaccine with that of the AstraZeneca vaccine.
I don’t want to dwell on this point other than to say first that it is incredibly unlikely that Dr. Zimmerman’s dose of J&J vaccine came from one of the contaminated batches given that the reporting I can find from the time indicates that the contamination was detected before the doses were shipped and that no doses of contaminated J&J vaccine ever reached the public. Second, even if Dr. Zimmerman did receive a contaminated dose it strains the imagination to come up with a mechanism by which such contamination would result in her constellation of medical symptoms, even if the cross contamination was the two adenoviral vectors making the spike protein, given that both were designed similarly. Finally, you would think that, instead of reporting only that Dr. Zimmerman thought her problems stemmed from a contaminated batch, Mandavilla would have mentioned some context and that apparently no contaminated batches ever reached the public. The story was more about an amount of that key ingredient, whatever it was, sufficient to manufacture many millions of doses of J&J vaccine having to be discarded and the sheer waste involved, rather than contaminated vaccine making it to the public.
As for Dr. Zimmerman, like a number of these patients, she has become a crusader, but much of what I found about her online didn’t help me understand much. For instance, this article didn’t really go into detail about her health problems but rather only mentions that it has been over 700 days since she had submitted her CICP claim and that she had no answers, nor did a BMJ Rapid Response by her help much either, other than that I basically agree that the CICP needs to do better. I also came across a long X/Twitter thread about the story in which Dr. Zimmerman describes some of the things she’s tried.
Here is a YouTube video of an interview that she did with Dr. Mobeen Syed, of whom I had never heard before. Perusing Dr. Syed’s social media, particularly his YouTube channel, led me to believe that he mixes useful, evidence-based tidbits with a lot of highly questionable medicine. Feel free to judge for yourself if you don’t believe me by perusing his YouTube channel. Suffice to say that I found a favorable interview with COVID-19 quack Dr. Paul Marik, founder of the crank or on his channel, among others, as well as a Substack linking to talks by him on COVID-19 vaccine “shedding” (which is not a thing). Moreover, the Substack algorithm seems to think that if I like Dr. Syed’s Substack I’ll like Substacks of the FLCCC Alliance and Dr. Pierre Kory. Overall, what I noticed was that his videos before the pandemic seem quite normal and reasonable, boring even, as lectures about medicine. After? Well, again, judge for yourself.
What saddened me is that in the interview, Dr. Zimmerman appears to have gone down the rabbit hole of thinking that she has mitochondrial injury and is undergoing tests for it. In fact, watching this video made me sad, because it’s clear that Dr. Zimmerman, in her desperation, is trying lots of different interventions, which range from the perhaps reasonable as a long shot to pure quackery, as you can see from these slides presented during the interview, which was published on May 12, 2023:
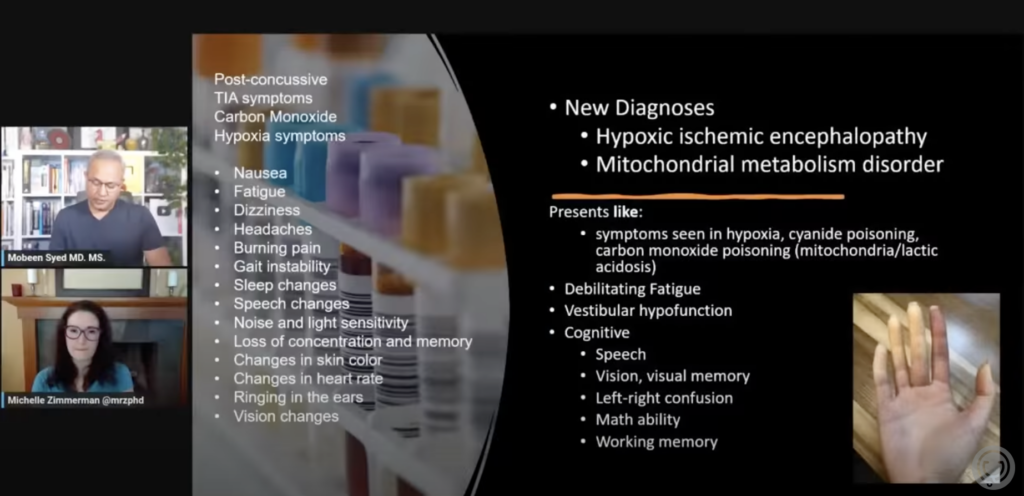
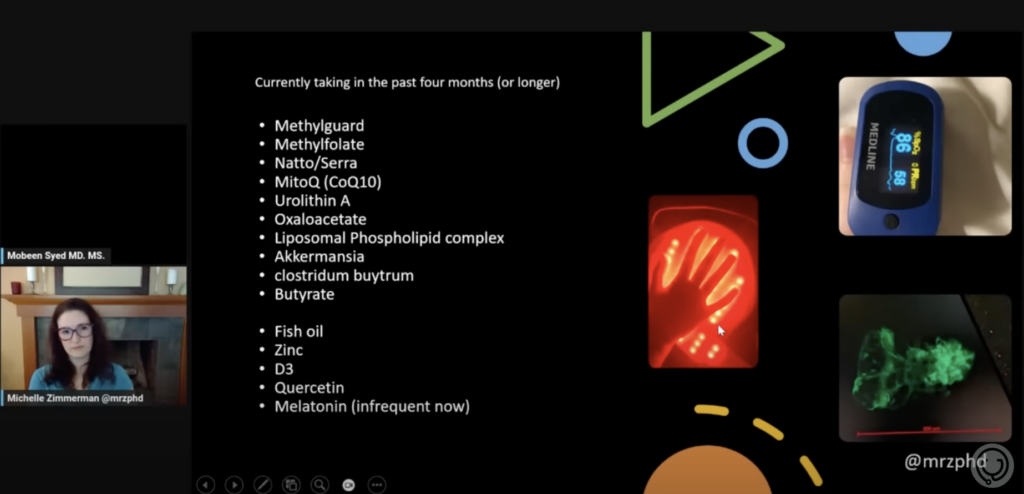
The treatments that she is undergoing are really where I feel for Dr. Zimmerman, who appears to have become the victim of at least some quacks:
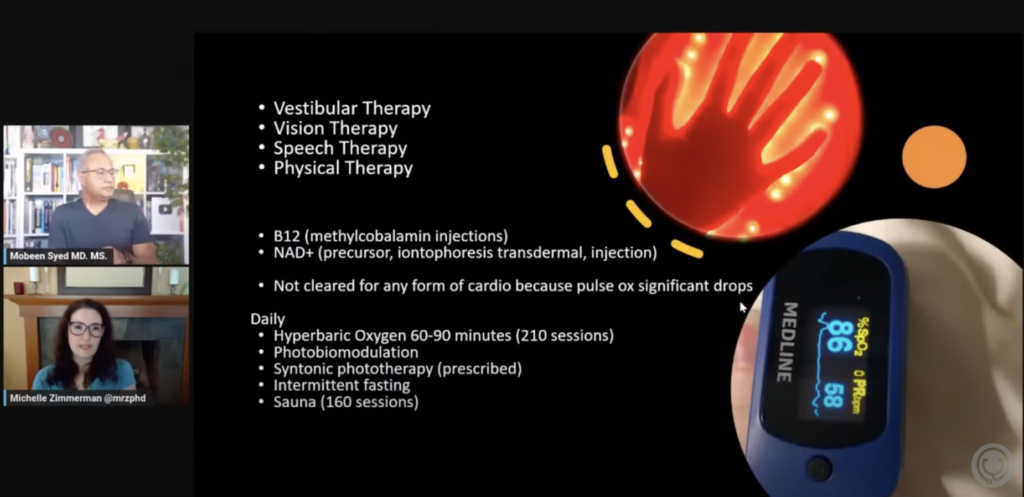
It leapt right out at me from the second slide that Dr. Zimmerman is using nattokinase and serrapeptase. I haven’t written about the latter but have noted that nattokinase has become a favorite quack treatment sold by COVID antivax quack Dr. Peter McCullough‘s The Wellness Company to treat “COVID vaccine injury,” the main difference being that, instead of serrapeptase, TWC’s formula includes another enzyme, bromelain.
As for some of the others, hyperbaric oxygen is a catch-all treatment that a lot of dubious health practitioners use to treat, well, basically everything. It generally has very few and very defined indications, such as in helping to heal hypoxic wounds, but most of its other uses are not evidence-based. Photobiomodulation is a form of laser treatment that might—the operative word being might—have some uses and benefits but has in generally been massively oversold, as noted by Jonathan Jarry, who describes it as a ” razzle-dazzle of cold lasers and red lights being used to treat just about anything,” and Paul Ingraham, who notes that such laser-based therapy is a “classic example of premature hype about a futuristic, ‘high-tech,’ unproven therapy: clinical practice races way ahead of the science, which barely exists, and all the hopes are pinned on vague and unfalsifiable biological plausibility, and research that is rife with fancy-sounding ‘mechanism masturbation’ — wishful and fanciful speculation about how it works rather than focusing on whether or not it actually does.” (Damn, Paul. I’m going to have to remember that term, “mechanism masturbation.”)
Unfortunately, the term appears to apply to some of the mechanisms mentioned in the interview, involving platelet activation, mitochondria, and various other measures. Dr. Zimmerman appears to have gone from researcher to researcher, including long COVID researchers like David Putrino, who has described microclots in patients with long COVID, in a desperate search to find what is causing her symptoms and how to alleviate them, citing a number of papers that might or might not have anything to do with each other and table after table of her lab results. For example, she shows an image from her blood from the Putrino lab showing microclots, but my reading of Putrino’s research leads me to think that he’s not about “vaccine injury”:
All of the long COVID patients Putrino has tested have had microclots and hyperactivated platelets, which is something he doesn’t commonly see in people who have never had COVID or who have fully recovered. It’s this high level of microclots in long COVID patients that Putrino thinks might be the biomarker. One of the questions that remains is, if they continue to see this pattern on a bigger scale, is targeting and getting rid of these microclots an effective treatment?
It is, however, true that Dr. Putrino is a co-author on one descriptive analysis reporting a “post-vaccination syndrome” after COVID-19 vaccination with the Moderna of Pfizer vaccine. Participants had joined the online Yale Listen to Immune, Symptom and Treatment Experiences Now (LISTEN) Study from May 2022 to July 2023:
The five most common symptoms were exercise intolerance (71%), excessive fatigue (69%), numbness (63%), brain fog (63%), and neuropathy (63%). In the week before survey completion, participants reported feeling unease (93%), fearfulness (82%), and overwhelmed by worries (81%), as well as feelings of helplessness (80%), anxiety (76%), depression (76%), hopelessness (72%), and worthlessness (49%) at least once. Participants reported a median of 20 (IQR: 13 to 30) interventions to treat their condition.
Concluding:
In this study, individuals who reported PVS after covid-19 vaccination had low health status, high symptom burden, and high psychosocial stress despite trying many treatments. There is a need for continued investigation to understand and treat this condition.
This study, of course, doesn’t apply to Dr. Zimmerman because it didn’t look at J&J vaccines. However, one always wonders if there’s something there, and I have no problem with more research being done. I realize that it’s possible that, should Dr. Zimmerman come across this post, she, like other patients whom I’ve discussed in the past, might take this as an attack on her. It is not. She is a victim here. Whether she is a victim of the vaccine or not, I have not been able to decide, but she is definitely a victim.
Other anecdotes
Mandavilli’s story is not just about Dr. Zimmerman, of course. It also tells the story of four other people, most healthcare professionals including, unsurprisingly, Dr. Gregory Poland, who has been in the news before for having developed “life-altering” tinnitus after the second dose of “an mRNA vaccine,” whom I also wrote about a year ago. In Mandavilla’s reporting, he experienced it after the first dose, which conflicts with this 2022 interview in MedPage Today. Another doctor, Dr. Buddy Creech, who ironically enough led several Covid vaccine trials at Vanderbilt University, reported tinnitus and racing heart for about a week after each shot, noting, “It’s very similar to what I experienced during acute Covid, back in March of 2020.”
His inclusion in the NYT report led me to update my PubMed search, as the studies available at the time had been conflicting, to determine if more recent work had found a link between the mRNA vaccines and tinnitus. One recent retrospective study found an elevated risk, as did another study, although another study found that over 20% of people who suffer from COVID-19 can develop tinnitus, while yet another found that, although a significant number of patients suffered sudden sensorineural hearing loss (of which tinnitus is one type) after vaccination, the incidence was “comparable to the general otology patient population” and still another found no correlation, although the latter was a single institution study. I was forced to conclude that we still don’t know if COVID-19 vaccines can cause the sudden onset of tinnitus and that it’s difficult to attribute causation because it is a common diagnosis and would be expected to occur within fairly close temporal association with vaccination during a mass vaccination campaign as huge as the COVID vaccine campaign was.
Also:
Shaun Barcavage, 54, a nurse practitioner in New York City who has worked on clinical trials for H.I.V. and Covid, said that ever since his first Covid shot, merely standing up sent his heart racing — a symptom suggestive of postural orthostatic tachycardia syndrome, a neurological disorder that some studies have linked to both Covid and, much less often, vaccination.
He also experienced stinging pain in his eyes, mouth and genitals, which has abated, and tinnitus, which has not.
“I can’t get the government to help me,” Mr. Barcavage said of his fruitless pleas to federal agencies and elected representatives. “I am told I’m not real. I’m told I’m rare. I’m told I’m coincidence.”
And:
Renee France, 49, a physical therapist in Seattle, developed Bell’s palsy — a form of facial paralysis, usually temporary — and a dramatic rash that neatly bisected her face. Bell’s palsy is a known side effect of other vaccines, and it has been linked to Covid vaccination in some studies.
But Dr. France said doctors were dismissive of any connection to the Covid vaccines. The rash, a bout of shingles, debilitated her for three weeks, so Dr. France reported it to federal databases twice.
“I thought for sure someone would reach out, but no one ever did,” she said.
I note that POTS has long been claimed to be a side effect of HPV vaccines, despite the lack of evidence. As for Bell’s palsy, the evidence is rather conflicting as well, with some studies possibly showing a slightly elevated risk after vaccination, while another finds no elevated risk after vaccination but a definite elevated risk after COVID-19. Again, the problem is that these conditions appear to be also associated with COVID-19.
Overall, Mandavilli interviewed 30 people over the course of a year who said they had been harmed by COVID-19 vaccines, noting that they “described a variety of symptoms following vaccination, some neurological, some autoimmune, some cardiovascular.” What stood out to me is that that is an incredibly small number given the billions of doses of COVID-19 vaccinations given worldwide and the hundreds of millions in the US alone. Indeed, even the “thousands” mentioned in the article would be a very tiny number compared to the number of people vaccinated. The problem, as I’ve always said, is the law of large numbers. When you vaccinate 270 million people, side effects with even a tiny chance of happening, will start to occur in large numbers. Moreover, never let it be said that I dismiss vaccine injuries; what I have a problem with is the framing of this article as an uncaring CDC and medical profession basically ignoring the concerns of these patients.
That being said, we do have to do better. Mandavilli reports that her 30 interviewees “had been turned away by physicians, told their symptoms were psychosomatic, or labeled anti-vaccine by family and friends — despite the fact that they supported vaccines.” I hope that no physician had labeled any of them “antivaccine,” but some lay public are indeed too fast to do that. That being said, I have little doubt that some doctors don’t handle dealing with odd symptom complexes well, particularly when there is little evidence to guide them with respect to cause or treatment.
Active versus passive surveillance
I again have to concede that not all of the reporting in this story is bad. For instance, in the article Mandavilli points out problems that really do hamper our ability to definitively recognize vaccine injury:
Federal officials and independent scientists face a number of challenges in identifying potential vaccine side effects.
The nation’s fragmented health care system complicates detection of very rare side effects, a process that depends on an analysis of huge amounts of data. That’s a difficult task when a patient may be tested for Covid at Walgreens, get vaccinated at CVS, go to a local clinic for minor ailments and seek care at a hospital for serious conditions. Each place may rely on different health record systems.
There is no central repository of vaccine recipients, nor of medical records, and no easy to way to pool these data. Reports to the largest federal database of so-called adverse events can be made by anyone, about anything. It’s not even clear what officials should be looking for.
“I mean, you’re not going to find ‘brain fog’ in the medical record or claims data, and so then you’re not going to find a signal” that it may be linked to vaccination, Dr. Woodcock said. If such a side effect is not acknowledged by federal officials, “it’s because it doesn’t have a good research definition,” she added. “It isn’t, like, malevolence on their part.”
Much of this is true.
On the other hand, although the Vaccine Adverse Events Reporting System (VAERS) features prominently in the article, as it does on all articles about vaccine injury, suspected or real, and Mandavilli points out (as above) that anyone can make a report about anything, nowhere in the article are other vaccine safety monitoring systems mentioned except in passing. For example, I was gobsmacked that nowhere in this article was there even a mention of the Vaccine Safety Datalink (VSD) or other vaccine safety reporting systems by name, although it was referred to:
Federal researchers also comb through databases that combine electronic health records and insurance claims on tens of millions of Americans. The scientists monitor the data for 23 conditions that may occur following Covid vaccination. Officials remain alert to others that may pop up, Dr. Daskalakis said.
Yes, the link above goes to a presentation from VSD data about COVID-19 vaccine safety, which is all well and good, but the percentage of people who click on most links is very small and those reading the article on a paper copy of the newspaper are not going to have even the option of getting that context. Overall, not naming the VSD when describing what it does and mentioning it almost in passing compared to VAERS leave the impression that VAERS is pretty much the be-all and end-all of vaccine safety monitoring in the US., which makes her comparison to other countries grate, at least to me, when I was reading this:
In some countries with centralized health care systems, officials have actively sought out reports of serious side effects of Covid vaccines and reached conclusions that U.S. health authorities have not.
In Hong Kong, the government analyzed centralized medical records of patients after vaccination and paid people to come forward with problems. The strategy identified “a lot of mild cases that other countries would not otherwise pick up,” said Ian Wong, a researcher at the University of Hong Kong who led the nation’s vaccine safety efforts.
That included the finding that in rare instances — about seven per million doses — the Pfizer-BioNTech vaccine triggered a bout of shingles serious enough to require hospitalization.
The European Medicines Agency has linked the Pfizer and Moderna vaccines to facial paralysis, tingling sensations and numbness. The E.M.A. also counts tinnitus as a side effect of the Johnson & Johnson vaccine, although the American health agencies do not. There are more than 17,000 reports of tinnitus following Covid vaccination in VAERS.
Are the two linked? It’s not clear. As many as one in four adults has some form of tinnitus. Stress, anxiety, grief and aging can lead to the condition, as can infections like Covid itself and the flu.
There is no test or scan for tinnitus, and scientists cannot easily study it because the inner ear is tiny, delicate and encased in bone, said Dr. Konstantina Stankovic, an otolaryngologist at Stanford University.
It is potentially a fair point that VSD is a smaller system than those of a lot of other countries because we do not have a centralized healthcare system or a centralized database of medical records or vaccinations. That might be why these countries found associations that the US did not. Also, Hong Kong paid people to come forward with their stories? I’d be worried that the offer of payment in and of itself could distort the reporting. It also doesn’t help that the context for the story isn’t really given in the story itself, but rather in a sidebar story, Covid Vaccine Side Effects: 4 Takeaways From Our Investigation. I’ll comment on each one.
- For most people, the benefits of Covid vaccines outweigh any risks. (Now she tells us.)
- Federal surveillance has found some side effects but may miss others. (Well, yes, but that’s why we examine data from all over the world. Each country’s system of vaccine safety monitoring has its strengths and weaknesses. And she cites VAERS as the largest but again, as though it were the be-all and end-all of vaccine safety monitoring. It’s also true that the Israelis beat us detecting the signal for myocarditis from the mRNA vaccines, but we found the signal for blood clots from the AstraZeneca vaccines in a timely fashion.)
- Proving vaccination led to an illness is complicated. (Yes, but the anecdotes sure do leave the impression that vaccination very likely caused the symptoms and conditions those interviewed are suffering from.)
- Understanding the full range of side effects may take years. (No one ever said otherwise, although, again, nearly all adverse events from vaccines manifest themselves within a few weeks of vaccination at most.)
Finally, let’s just say that antivaxxers have noticed this article and viewed it about the way you’d predict:
I could go on and on and on, but you get the idea from the sample above and this article featured on Robert F. Kennedy, Jr.’s antivax org Children’s Health Defense:

Let’s just say that antivaxxers know an article that is echoing their longstanding messages, and when that article appears in the NYT they are going to do their utmost to spin it as vindication. While it is the duty of news organizations to hold authority to account for its failures and point out where systems like our vaccine safety monitoring system need reform and improvement, which this article does, it’s also important not to make it too easy for enemies of public health and vaccination to use your reporting for their own purposes, which is what the NYT did here. Its poor framing based on an all-too-familiar (and tired) trope of people with mysterious diseases who believe they know what caused them being supposedly ignored and vilified by conventional medicine undermined what could have been an excellent story about the massive shortcomings of the CICP and problems with our current vaccine safety monitoring program.
Worse, framing like this does nothing to help those who are really suffering, like Dr. Zimmerman.
ADDENDUM: Dr. Vincent Iannelli has commented on the NYT article. He is a bit more harsh than I was, to the point that I wonder if I went too easy on Mandravilli and her editors at the NYT. On the other hand, I do note that Alex Berenson is not pleased with Mandravilli’s article, calling it a “gaslighting masterpiece.”