
{kind=link}
If there’s one reliable characteristic of physicians who go all-in on antivaccine beliefs, it’s that, after they have come to identify vaccines as The One True Source of All Chronic Disease (or just a bunch of toxic sludge causing “vaccine injury”), it is almost inevitable that they come up with quackery to treat what they view as vaccine-induced chronic disease or injury. Back in the “old days,” I used to write about what was called “autism biomed,” because the primary antivaccine claim 15 years ago was that childhood vaccines cause autism. Basically, “autism biomed” was—and remains—a blanket term used by believers in the vaccine-autism conspiracy theory to describe a rather large collection of quackery that included chelation therapy, various “detox” regimens, “metabolic” treatments, and more, none of which had one iota of evidence to support them as treatments for autism spectrum disorders. Use of the term “biomed” was meant to imply that these were legitimate “biomedical” treatments for “vaccine-induced autism,” when in reality they consisted mainly of a motley collection of “detox” quackery, often bolstered by “functional medicine” and various alternative medicine treatments like naturopathy and homeopathy. This brings me to Dr. Peter McCullough and his “Base Spike Detox,” which uses enzymes like nattokinase and bromelain to “detox” the spike protein from both COVID-19 and COVID-19 vaccines. As it turns out, Dr. McCullough’s protocol is just a variant of an earlier protocol that I first learned about earlier this year, Signature Series Spike Support Formula sold by The Wellness Company and promoted by Dr. McCullough, a video of whom is featured on the product page, but had never gotten around to writing about on this blog.
Here are the ingredients of the supplement, which is advertised to let you “get back to that pre-COVID feeling”:
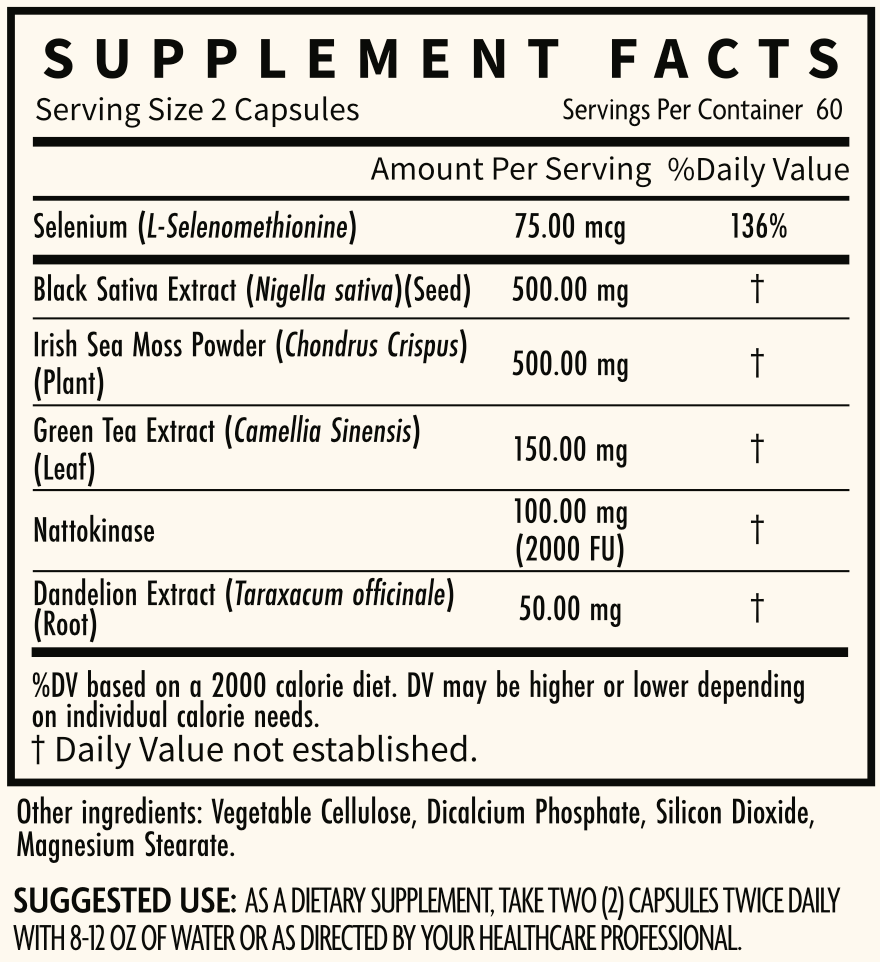
Note the Quack Miranda Warning. What I want to know is: Why all the other herbs?
As for the claims:
Spike Support Formula contains all natural, non-GMO, scientifically-supported ingredients:
Nattokinase has been researched to dissolve spike proteins and blood clots.
Dandelion root may prevent spike protein from binding to your cells.
Selenium to help reduce stress, aiding in helping the body repair itself and recover.
Black sativa extract may facilitate cellular repair.
Green tea extract provides added defenses at the cellular level through scavenging for free radicals.
Irish sea moss is mineral-rich and could help rebuild damaged tissue and muscle.
Leaving aside the nattokinase for a moment, you can see that most of the claims for the herbs and extracts are all fairly generic; i.e., “rebuild damaged tissue”; “facilitate cellular repair”; or “help reduce stress.” We’ll look at the other claims in a moment, such as that nattokinase dissolves spike protein and dandelion root “may prevent spike protein from binding to your cells.”
Obviously, Dr. McCullough is far from the first example of COVID-19 antivax docs making a pivot towards unproven treatments. One prominent example that comes to mind is America’s Frontline Doctors, a group that first made a name for itself resisting “lockdowns,” masking, and public health interventions for COVID-19 but then later pivoted to a highly profitable grift running a telehealth prescription mill for ivermectin. Ivermectin, of course, was billed the inexpensive highly effective treatment for COVID=19 that “They” don’t want you to know about. In addition, although I have been unable to figure out who first came up with the idea of using nattokinase to “dissolve spike protein,” I do know that this particular detox formulation appears to have been the “brainchild” (and I do use the word “brain” very loosely here) of Jen VanDeWater, who’s a pharmacist selling something called “Dr. Jen VanDeWater’s Spike Recovery Formula,” which is billed as the “gold standard” in combatting “shedding” and fending off the “deadly spike protein”:
These are the basics for the claims about nattokinase as a treatment for COVID-19, long COVID, and COVID-19 “vaccine injury.”
Dr. McCullough, however, is a bit different in that he’s promoting his nostrums not just to treat COVID-19 and long COVID, but to “detox” people from the dreaded spike protein used as the antigen in COVID-19 vaccines. The key ingredient in the Spike Support Formula is nattokinase, which is a proteolytic enzyme (an enzyme that cleaves proteins at specific sites), and now apparently Dr. McCullough has added another proteolytic enzyme, bromelain, to the mix:
I have found in my clinical practice that most multiply infected and or COVID-19 vaccine injected patients with post-COVID-19 symptoms respond slowly after three months or more of “Base Spike Detox” which contains:
- Nattokinase 2000 FU (100 mg) twice a day
- Bromelain 500 mg daily
- nano Curcumin 500 mg twice a day
So what are nattokinase and bromelain, and why does Dr. McCullough promote them as treatments to “detox” you from spike protein, whether it comes from COVID-19 or the dreaded and much more evil (apparently) spike protein that the mRNA vaccines induce your cells to make in minute quantities? Let’s find out.
Nattokinase
I was unfamiliar with nattokinase before, but several months ago I had bookmarked a post by Dr. Paul Alexander that basically laid out the entire “rationale”—again, if you can call it that—for using nattokinase to “detox” from the dreaded spike protein. First, he says that you need to “detox” the spike protein, particularly if you’ve had the vaccine:
Spike protein (due to the COVID vaccine or virus) is becoming increasingly concerning and people are begging for solutions. They are scared and in many instances distraught as to the spike circulating within them. As a result, a spike detoxifier is needed. This detoxifier can potentially help manage the amount of spike protein in your body (especially spike induced by the Pfizer and Moderna gene platform).
Seeing a claim like this leads me to point out some things. First, the amount of spike protein that gets into the bloodstream as a result of the mRNA COVID-19 vaccines made by Pfizer and Moderna is infinitesimally small, definitely smaller than the amount of spike protein one gets from an—oh, you know—actually infection with SARS-CoV-2, the coronavirus that causes COVID-19. Second—and I know I’m repeating myself from above, but bear with me—antivaxxers have been recommending “detoxification” to treat “vaccine injury” or “vaccine toxicity” since long before I ever first took notice of the antivaccine movement which was well over two decades ago. Nattokinase, as you will see, is just the latest wrinkle in this old narrative.
Unsurprisingly, instead of blaming the virus for long COVID, Alexander blames—you guessed it!—the vaccine:
This is a particularly important consideration given the massive reporting of symptoms post recovery from virus infection or taking the COVID mRNA-DNA gene injection (Pfizer and Moderna). I am referring to what is called ‘LONG-COVID’ and you may have heard this term or similar. The advancing ‘maturing’ science is focusing on clarifying this condition yet it is clear just by looking around us in our own personal daily lives (ourselves, our family members, our friends, or our work colleagues as well as just strangers who shared their struggles), that this COVID gene injection or the virus leaves many with symptoms and often debilitating crippling one. This is no laughing matter and some (many) people are very damaged by the gene injection vaccine (as well as the virus).
At least Dr. Alexander sort of acknowledges that the virus might actually cause long COVID. Of course, he frames it by saying “some (many) people” were damaged by the “gene injection” vaccine “as well as the virus.” His readers know what he really means, namely that he’s claiming that the vaccine is the primary cause of what is being labeled “long COVID.” Lest you fail to get that message, he rapidly pivots to claim:
The reality is that the COVID gene injections (so called vaccines) induces the very toxic dangerous part of the COVID virus that causes severe and often fatal disease sequelae, this being the spike protein, as part of the immune response. The spike protein and especially the S1 sub-unit of the spike protein is highly pathological and is more than likely involved in the often crippling post-vaccination syndrome e.g. LONG COVID. The spike protein is devastatingly toxic (references here, here, here).
I can’t help but note that the first article uses a mouse model to study acute lung injury from COVID-19 involving artificially high doses of spike protein. The second article is by Stephanie Seneff, a naturopath, and Peter McCullough. (‘Nuff said.) The third article is about the incidence of acute allergic reactions to COVID-19 vaccines, and I note that pretty much all vaccines can cause rare allergic reactions, making COVID vaccines nothing unique on that score. None of these articles, other than the mouse model, demonstrates that the spike protein is a “toxin” that causes long COVID, and even the mouse model is of limited utility in that the dose used (400 µg/kg) is huge compared to anything a vaccine could cause and arguably even more than infection can cause. Also, the recombinant spike protein was administered not intramuscularly or intravenously, but intratracheal, meaning that the investigators squirted saline containing it into the tracheas of the mice. Anyway, cherry picking and misrepresenting studies is how dishonest antivaxxers roll.
So what does nattokinase supposedly do? Actually, maybe it’s more appropriate to ask: How does nattokinase supposedly “dissolve” the dreaded spike protein, which to antivaxxers is so much more horrible if it comes from the toxin-laden vaccines rather than naturally from the disease?
According to Alexander:
Recent literature has shown nattokinase to be effective in degrading the spike protein associated with COVID-19 [3]. It has long been known to reduce the risk of clot formation and improve circulation [3].
Before I started looking into what nattokinase is even supposed to do, let me just briefly note that the first thing I always wonder about when I see an enzyme being touted as a treatment for anything is how a protein—an enzyme—can work when taken orally. In general, proteins are rapidly broken down in the stomach and proximal small intestine by a number of other very efficient enzymes that chew up the peptide chain. It is true that there are a few exceptions, but they tend to be digestive enzymes, which can survive in the harsh chemical environment of the stomach and enzymatic environment of the small intestine. Examples include pancreatic enzymes, whose function can indeed be replaced by oral supplementation because these enzymes are among the enzymes that work in digestion. Nattokinase does not appear to be one of these enzymes. So what is it?
It turns out that nattokinase is an enzyme used to ferment soy bean products that have long been a dietary staple in Japan. It also turns out that it’s been a popular supplement dating back to long before the pandemic. If you do a Google search for just “nattokinase” a lot of the results will be supplement sellers promoting it for its various claimed health benefits. In brief, nattokinase is extracelluar enzyme secreted by the bacterium Bacillus subtilis, used to ferment boiled or steamed soybeans resulting in a preparation called nattō. The Memorial Sloan-Kettering website notes:
Nattokinase is also available as a supplement and is most known for its effects on prevention and treatment of clots and to improve blood circulation.
And:
Nattokinase has been promoted as an alternative anticancer treatment based on the notion that it can help dissolve the fibrin coating around a tumor, and increase oxygen supply in the blood to inhibit cancer cell growth. However, these mechanisms have not been proven in humans.
Nattokinase is also purported to treat Alzheimer’s disease and hypertension and a number of other disorders, because of course it is.
So right away you can see why nattokinase would be attractive to COVID antivax quacks, given that one of the main false claims about these vaccines is that they are causing people to “die suddenly” of clotting disorders leading to strokes and myocardial infarctions (heart attacks). (They aren’t.) To quacks, nattokinase could be a two-for, both supposedly “dissolving” that nasty, toxic, evil spike protein (from the vaccine) and also dissolving clots. It’s also not as though nattokinase doesn’t have activities in vitro (test tube and cell culture) that do have relevance to clotting:
In vitro studies show that nattokinase decreases clot formation by cleaving and inactivating the plasminogen activator inhibitor (PAI) via proteolysis at P1-P1’ peptide bond. PAI is a key inhibitor of tissue plasminogen activator (tPA) that converts plasminogen to plasmin. PAI inactivation allows for greater tPA activity and increased lysis of clots (10) (11). In the absence of PAI, nattokinase affects direct proteolysis of fibrin; however, this effect is less than the protelysis achieved by the PAI-mediated pathway (2). The fibrinolytic activity of nattokinase is estimated to be four-fold that of plasmin (12).
The question, of course, is whether the in vitro activities of nattokinase translate into anything therapeutic in vivo in humans. The answer is: We don’t know. However, it strikes me as highly unlikely that nattokinase does these things in the human bloodstream when taken orally. One WebMD perusal of the evidence is full of “maybes” and other qualifiers like “possibly,” in which it’s claimed that nattokinase “might” increase your risk of bleeding, decrease your blood pressure, etc., but notes that there’s basically little to no clinical evidence to support these uses.
So what evidence do doctors like Dr. McCullough cite when recommending nattokinase? They always have some evidence to cite, but is it in any way convincing? In an earlier Substack post from February, Dr. McCullough was touting the Dissolution of Spike Protein by Nattokinase, which he called the “Holy Grail of COVID-19 vaccine detoxification,” handwaving an “explanation” of why the vaccine-induced spike protein is so much more nasty than the much huger amounts of spike protein produced by an actual infection:
Far and away the most common question I get from those who took one of the COVID-19 vaccines is: “how do I get this out of my body.” The mRNA and adenoviral DNA products were rolled out with no idea on how or when the body would ever breakdown the genetic code. The synthetic mRNA carried on lipid nanoparticles appears to be resistant to breakdown by human ribonucleases by design so the product would be long-lasting and produce the protein product of interest for a considerable time period. This would be an advantage for a normal human protein being replaced in a rare genetic deficiency state (e.g. alpha galactosidase in Fabry’s disease). However, it is a big problem when the protein is the pathogenic SARS-CoV-2 Spike. The adenoviral DNA (Janssen) should broken down by deoxyribonuclease, however this has not be exhaustively studied.
This leaves dissolution of Spike protein as a therapeutic goal for the vaccine injured. With the respiratory infection, Spike is processed and activated by cellular proteases including transmembrane serine protein 2 (TMPRSS2), cathepsin, and furin. With vaccination, these systems may be avoided by systemic administration and production of Spike protein within cells. As a result, the pathogenesis of vaccine injury syndromes is believed to be driven by accumulation of Spike protein in cells, tissues, and organs.
It is, of course, utter nonsense to claim that the vaccines were rolled out with “no idea on how or when the body would ever breakdown the genetic code.” Extensive preclinical work on the vaccines, plus the two decades of work before that developing the mRNA vaccines in general, provided a lot of knowledge on how mRNA, even the modified mRNA used in the vaccines, is broken down in cells and the body. Just because we don’t know everything does not mean that we know nothing, although that is a frequent false dichotomy promoted by antivaxxers.
It is, of course, true that the mRNA vaccines were designed using modified ribonucleotides that are more resistant to being broken down by human ribonucleases, but that’s mainly because most mRNAs are quite short-lived and rapidly broken down this way. To have a chance of making sufficient spike protein to elicit an immune response, a much longer half-life was required. Instead of half lives of minutes to hours which is typical for most mRNAs (the median half-life of all human mRNAs as a group is around 10 hours), a half-life on the order of days was required. (As an aside, the half-life of the mRNA for a gene that I once studied as a graduate student was around 4 hours, but would decrease to less than an hour in response to cell stimulation with serum.) In contrast, the half-life of the mRNA for spike protein used in the Pfizer and Moderna vaccines is on the order of a few days, with the spike protein being detectable for at most a few weeks. While it is true that one study oft-cited by antivaxxers found vaccine mRNA fragments in the blood as long as 28 days after vaccination, I note that this was mostly fragments, meaning that the mRNA would not be expected to generate further spike protein and that the authors speculated that this finding might have been due to slow leakage of the lipid nanoparticles out of the injection site. In any event, contrary to what antivaxxers claim, neither the modified mRNA nor the spike protein coded for by that mRNA persist longterm in the human body. They do not need to be “detoxed.” The body can do a perfectly find job of that.
In the same post, Dr. McCullough cites three studies. One is, unsurprisingly, an in vitro study in which cells infected with SARS-CoV-2 and lysates from cells were exposed to different doses of nattokinase, after which the authors reported:
When cell lysates transfected with S protein were incubated with nattokinase, the S protein was degraded in a dose- and time-dependent manner. Immunofluorescence analysis showed that S protein on the cell surface was degraded when nattokinase was added to the culture medium. Thus, our findings suggest that nattokinase exhibits potential for the inhibition of SARS-CoV-2 infection via S protein degradation.
They also appear to have done some of the appropriate controls, such as heating nattokinase to inactivate it or treating it with a protease inhibitor to inhibit its ability to cleave protein strands and then observing that such treatments eliminated the ability of nattokinase to degrade spike protein. A similar study, also cited by Dr. McCullough, reported that nattokinase can inhibit SARS-CoV-2 infection in cell culture. Of note, both studies examined whether nattokinase had an effect on spike protein produced by the virus (SARS-CoV-2) not whether the enzyme could degrade spike protein produced by cells transfected with the vaccine. Overall, the two findings aresomewhat interesting. They might or might not lead to the use of nattokinase to treat or alleviate COVID-19 infection. My prediction is that they probably won’t, simply because the vast majority of cell culture results don’t translate to a treatment, but I’ll concede that the findings are somewhat interesting nonetheless.
Of course, Dr. Peter McCullough is a lot less…measured…in his reaction to the study:
Based on these findings, nattokinase and similar products such as serrapeptase should undergo well-funded, accelerated preclinical and clinical development programs. The issue at hand is the urgency of time, similar to that with SARS-CoV-2 infection and empiric early therapy. It will take up to 20 years to have a fully developed pharmaceutical profile to characterize the safety and efficacy of nattokinase in the treatment of vaccine injury and post-COVID syndromes. Large number of people are sick now and many believe empiric treatment is justified given sufficiently low risk of side effects and potentially high reward. My recommendation is to discuss this with your doctor or seek a specialist in holistic or naturopathic medicine who is experienced with the safety profile of nattokinase in a range of applications.
Notice how McCullough assumes that this will be used for “vaccine injury,” even though the intent of the researchers who published these papers was to explore whether nattokinase can inhibit the infection of human cells by SARS-CoV-2. Also notice how much he exaggerates the timeline for figuring out whether nattokinase has a clinical effect on SARs-CoV-2 infection. It doesn’t take 20 years to test a compound that already exists and already has some preclinical evidence, even if you count doing the necessary preclinical animal model studies. Far from it! Dr. McCullough is simply exaggerating how long it would take to provide strong clinical evidence for nattokinase in order to justify using it now without any such evidence.
But what about the claimed effects of nattokinase with respect to clotting? There, the evidence is rather mixed. There is, for example, some in vitro evidence for activities in vitro (test tube and cell culture) that do have relevance to clotting:
In vitro studies show that nattokinase decreases clot formation by cleaving and inactivating the plasminogen activator inhibitor (PAI) via proteolysis at P1-P1’ peptide bond. PAI is a key inhibitor of tissue plasminogen activator (tPA) that converts plasminogen to plasmin. PAI inactivation allows for greater tPA activity and increased lysis of clots (10) (11). In the absence of PAI, nattokinase affects direct proteolysis of fibrin; however, this effect is less than the protelysis achieved by the PAI-mediated pathway (2). The fibrinolytic activity of nattokinase is estimated to be four-fold that of plasmin (12).
The question, of course, is whether the in vitro activities of nattokinase translate into anything therapeutic in humans. The answer is: We don’t know, but it strikes me as highly improbable. Let’s look.
Again, nattokinase is an enzyme. It should be expected to be digested when taken orally; it would not be expected to get into the bloodstream where it might actually be able to exhibit its ability to break down clots that it exhibits in a test tube. Its proponents, however, frequently cite this review article that claims otherwise. However, the way this review was written immediately got my skeptical antennae twitching with claims such as:
Nattokinase is considered to be a safe, powerful, low cost, and all-natural supplement for the treatment of heart and cardiovascular disease [5,6,7]. Animal [3,4,8] and human trials [9,10,11] have demonstrated that NK provides support to the circulatory system by thinning the blood and dissolving blood clots.
That first sentence is…something. But what about the cited articles? There are animal studies, but I zeroed in on the human studies. What impressed me about them was that none of them ever actually showed that nattokinase actually got into the bloodstream by measuring its concentration in the blood. For example, this randomized, double-blind study randomized healthy volunteers to receive a single dose of nattokinase supplement or placebo after a baseline blood draw. After the dose, blood was collected at 2, 4, 6, and 8 hours and various clotting parameters measured. The results? Basically nothing, although the authors sure tried to make it seem otherwise:
As a result, D-dimer concentrations at 6, and 8 hours, and blood fibrin/fibrinogen degradation products at 4 hours after NK administration elevated significantly (p < 0.05, respectively). Factor VIII activity declined at 4 and 6 hours (p < 0.05, respectively), blood antithrombin concentration was higher at 2 and 4 hours (p < 0.05, respectively), and the activated partial thromboplastin time prolonged significantly at 2 and 4 hours following NK administration (p < 0.05 and p < 0.01, respectively). All the changes, however, were within the normal range. In conclusion, thus, a single-dose of NK administration appears enhancing fibrinolysis and anti-coagulation via several different pathways simultaneously.
The key passage: “All the changes, however, were within the normal range.” In other words, no clear effect was demonstrated, and the authors did not actually even measure nattokinase in the blood of study subjects, which is odd, given that they went to the trouble to draw all those timed blood samples.
In fairness, there is a pharmacokinetic study in humans—a ten year old study!—suggesting that nattokinase can get into the bloodstream, but interestingly the study did not say that it detected bioactive nattokinase. Given that it used an enzyme-linked immunosorbent assay (ELISA) to detect nattokinase in the blood, it is entirely possible that the antibody in the assay detected consisted of large fragments of degraded nattokinase or nattokinase that had been denatured (the protein unfolded) and was therefore inactive, leading the authors to note that “looking for intact enzyme and bioactive nattokinase peptides should be a consideration for future studies investigating the pharmacokinetic profile of nattokinase.” No kidding, as I noticed that a lot of the human studies of nattokinase (for example, this one) didn’t measure it in the blood even by ELISA. This all left me wondering whether it was actually nattokinase or something else in the concoction that might be affecting what was observed.
As you might expect, I couldn’t resist doing my own PubMed search on nattokinase to see what sorts of studies had been done more recently on nattokinase. I couldn’t help but immediately find this 2021 double-blind randomized controlled clinical trial that found zero effect of nattokinase versus placebo on the progression of atherosclerotic disease, which is one of the indications claimed for this enzyme. My entire take on nattokinase with respect to clotting and atherosclerosis is that it’s possible that maybe some intact enzyme survives digestion in the gut to be absorbed into the bloodstream to do something therapeutic, but that the evidence that it actually does anything clinically relevant in cardiovascular disease when administered orally is quite weak.
However weak the evidence is for oral nattokinase as a clot buster and drug to prevent atherosclerosis, the evidence base to support a conclusion that it does anything therapeutic whatsoever for COVID-19, long COVID, or COVID-19 “vaccine injury” is far, far weaker, as in close to nonexistent. None of this stops Dr. McCullough or others from promoting this quackery.
But what about bromelain? I think you know the answer.
Bromelain
Bromelain is an enzyme extract derived from the stems of pineapples, although it exists elsewhere in the pineapple as well. Wikipedia tells me that bromelain is commonly used in cosmetics, as a topical medication, and as a meat tenderizer, the last of which is something I always look for in a therapeutic enzyme. (That’s sarcasm. I realize that nearly all of you realize that, but I can never count on everyone realizing it.) In any event, bromelain contains proteases, which break down proteins by using water to break the bonds between the amino acids, usually at specific sites based on short peptide sequences recognized by the enzyme. It turns out that bromelain has a fairly broad specificity.
So what does Dr. McCullough claim about bromelain for “detoxing” spike protein? He starts out by referencing a review article by Varila et al, noting:
Bromelain is available in topical Nexobrid to cleanse third degree wound eschars. One vial contains 2 g of concentrate of proteolytic enzymes enriched in bromelain, corresponding to 0.09 g/g concentrate of proteolytic enzymes enriched in bromelain after mixing (or 2 g/22 g gel). The proteolytic enzymes are a mixture of enzymes from the stem of Ananas comosus (pineapple plant).
Oral bromelain has been safety tested up to 12 grams per day which is considerably higher than the typical 500 mg once a day used for Base Spike Detox. Bromelain partially degrades the Wuhan Spike protein and is a mild blood thinner. The review by Varilla points out that the PT and PTT blood tests can be prolonged with Bromelain. I have found patients taking Bromelain and Nattokinase together in Base Spike Detox need to be informed of the risks of bleeding and for them not to undergo d-dimer, PT, or PTT testing since the results will be abnormal as a result of therapy.
Again, just like activity as a meat tenderizing, I always look for something that, when used topically, breaks down burn wound eschars, which is the black burned skin overlying third degree burns and deep second degree burns that needs to be debrided (removed) before skin grafts can be applied. Oddly enough, Dr. McCullough even includes the prescribing information for Nexobrid:
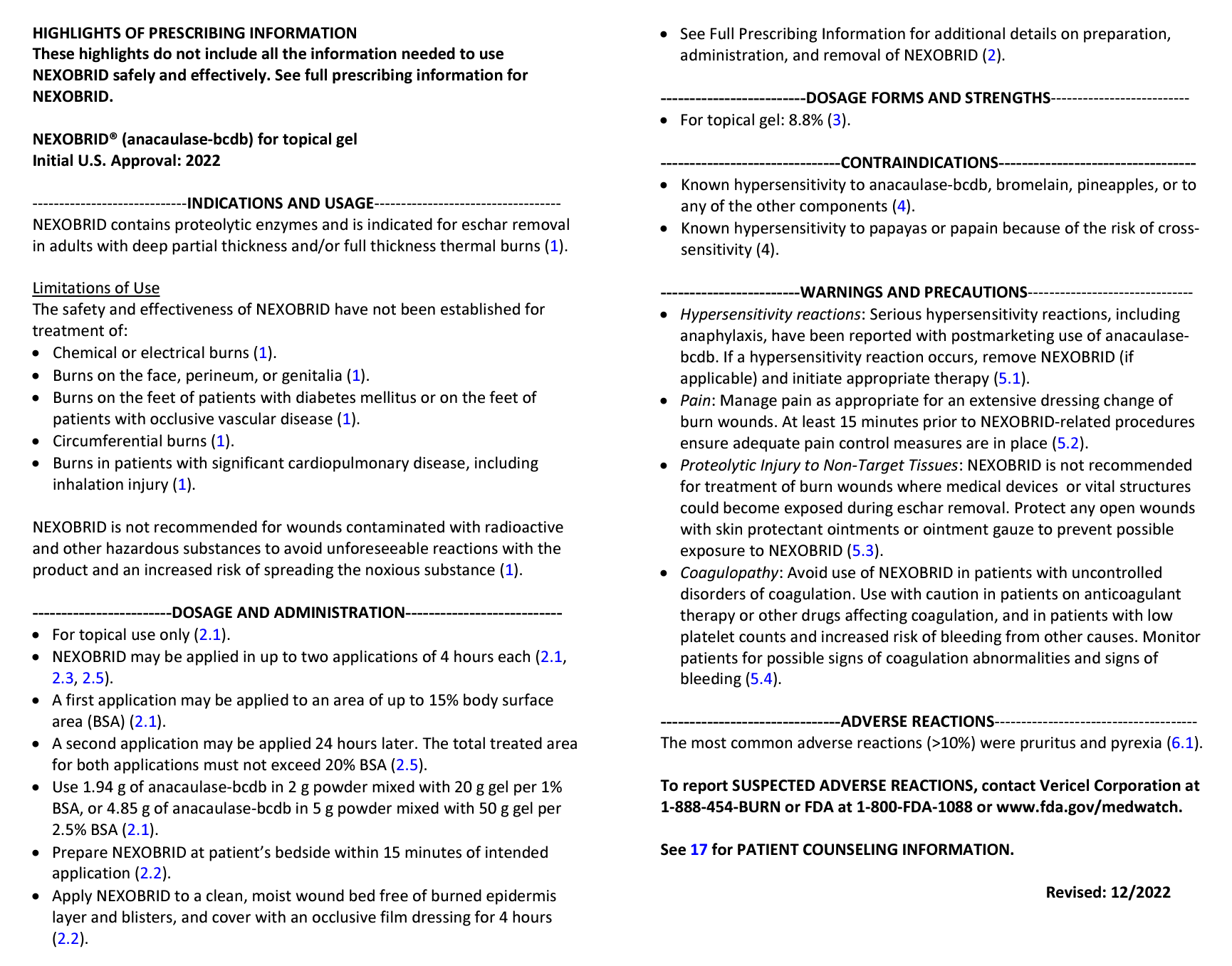
Nexobrid prescribing data. Not e the part about Nexobrid being able to cause injury to non-target tissues unless you’re careful.
This is all very interesting to me as a surgeon, but it is irrelevant to whether or not Nexobrid (and bromelain) are useful at all for treating COVID-19 or “detoxing” spike. It’s just information that looks impressive to nonphysicians.
Still, bromelain is one of the proteins that can be absorbed orally and retain its activity in the bloodstream, the evidence being more robust than the evidence for nattokinase:
Bromelain is absorbed efficiently in the human body and thus has a high bioavailability in an in vitro study [35]. This occurs as a result of its ability to bind to the two principal antiproteinases in the blood, alpha 2-macroglobulin and alpha1-antichymotrypsin. Without any significant side effects, it has been recorded that almost 12 g/day of bromelain can be taken in an in vivo study [36]. In addition, bromelain is absorbed in its active form throughout the gastrointestinal tract, with approximately 40 percent of the total bromelain absorbed in its high molecular weight form from the intestine [37]. In terms of pharmacokinetics, the maximal level of bromelain in the blood was obtained an hour after oral dosing [35]. Furthermore, [36] found that bromelain retains its plasma proteolytic function. Based on this, a more recent in vitro test showed that after 4 h, approximately 30% of bromelain remained stable in artificial stomach juice and that after the same time, roughly 20% of bromelain also remained stable in artificial blood [35].
Of course, just because bromelain can get into the bloodstream as an active enzyme does not mean that it does anything for COVID-19. This bothers Dr. McCullough not in the least, as he doesn’t even try to claim that bromelain does anything other than get into the bloodstream in active form and possibly break down clots:
We await additional post-COVID-19 and vaccine injury studies with Bromelain. It is reassuring it has bona fide proteolytic effects in the form of an approved topical therapy and its oral formulation is well absorbed and at doses of 500 mg patients are well below a threshold of concern. Since the Spike protein is known to be thrombogenic and many of the post-COVID-19 and vaccine injury syndromes are potentially related to micro- and macro-thromboses, Bromelain is well positioned as a component of Base Spike Detox.
Let me get this straight. Even Dr. McCullough admits that bromelain is unproven in COVID-19 and that there are no studies. (He can’t even cite an in vitro study showing that bromelain can actually digest spike protein in cell culture!) Out of curiosity, I did a quick PubMed search for studies examining bromelain and the SARS-CoV-2 spike protein. I found three. One study suggested that antibodies to SARS-CoV-2 can cross react with bromelain (among a number of other antigens from food). I looked at the chart, and it only shows 30% crossreactivity. Make of that what you will. I don’t make very much of it. Another study found that a lectin constituent of bromelain could bind spike protein with a “low micromolar KD,” which is not particularly tight binding for a drug. (Let’s just say that I’ve worked with repurposed drugs whose concentration to achieve 50% effect is in the low micro molar range and rapidly learned the hard way that such compounds are generally not considered particularly good drug candidates because generally a lot of drug is needed and that means toxicity. The third study presents evidence that bromelain can decrease the expression (amount made) of the ACE2 receptor, which is what SARS-CoV-2 binds to via its spike protein to get into the cell. However, the concentrations of bromelain required are huge, as high as 75 µg/ml, which reminds me of ivermectin, where the amount of drug required to inhibit SARS-CoV-2 in cell culture is a couple of orders of magnitude higher than what can be achieved safely in the bloodstream.
No wonder quacks love it. In fairness, there are other papers on bromelain and COVID-19 that have been published that only come up if I search just “bromelain” and “COVID-19.” One study showed that bromelain can inactivate SARS-CoV-2, but required, again, very high concentrations of bromelain (at least 50 µg/ml). Another study is quite speculative, combining curcurmin and bromelain and suggesting that they might modulate the immune system to treat COVID-19. (Unsurprisingly, Dr. McCullough loves this study.) Then there’s an in silico modeling study suggesting that bromelain can bind to the spike protein. (Dr. Paul Alexander loves this one.) I could go on, but you get the idea. This is all very thin gruel indeed even to try to use as preliminary evidence to justify a randomized clinical trial, much less to treat anyone with in the absence of clinical trials.
Treatments targeting spike protein
In the end, everything old is new again. If you are an antivax physician, you believe that vaccines are toxic sludge pits that poison your body with “toxins” that need “detoxing.” In the age of COVID-19, the only difference is that the “toxins” being targeted by “detox” regimens are different. They’re the spike protein, primarily, even if the antivax quacks have to find a way to portray that evil “unnatural” spike protein made by the vaccines as so much worse than the “natural” spike protein from the infection that to them causes no harm other than producing “natural immunity.”
I like to say that the antivax movement is, when you boil it all down, a purity cult, and the quacks who use unproven treatments like nattokinase and bromelain to treat a disease like COVID-19 through “detoxification” are just catering to that belief.