
{kind=link}
A Flashback
The first few times I read anti-vaccine articles, I found them superficially plausible. I lacked the background knowledge to spot their flaws and was blissfully ignorant of the mendaciousness that characterizes the anti-vaccine movement. It was only when I dug further that I realized their grave flaws. For example, in a collection of articles titled “200 Evidence Based Reasons NOT To Vaccinate,” Sayer Ji, the founder of the anti-vaccine site GreenMedInfo listed an article titled “A Measles Outbreak Was Reported in a Highly Vaccinated Population, San Diego, 2008.”
Sounds bad, right?
However, the actual title of the article, which was published in the journal Pediatrics in 2010, was “Measles Outbreak in a Highly Vaccinated Population, San Diego, 2008: Role of the Intentionally Undervaccinated.” The article concluded that “measles outbreaks can occur among clusters of intentionally undervaccinated children, at major cost to public health agencies, medical systems, and families.” In attempting to convince people vaccines don’t work, Mr. Ji distorted the findings of articles that showed vaccines work quite well.
Previously, this sort of blatant deception was practiced only by the most egregious anti-vaccine grifters.
A Review
With this in mind, let’s again discuss vaccine-myocarditis. Broadly speaking, there are two types of studies on this rare side effect, those on its frequency and those on its clinical course. Generally speaking, studies on the frequency of vaccine-myocarditis tell us nothing about its severity, and studies on its severity tell us little about its frequency. We only know that vaccine-myocarditis is relatively rare, since most studies on its severity contain dozens, not thousands of patients.
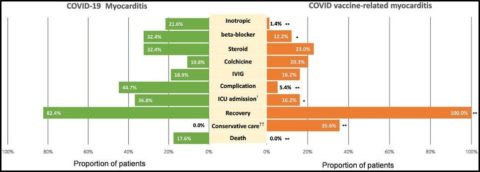
Studies on its frequency require researchers to comb through databases to find needles in haystacks, and unsurprisingly, there is a large variation in what they’ve found. In contrast, studies on its clinical course start with those needles and report on patient outcomes. Fortunately, there is complete agreement amongst over 25 studies that “most myocarditis cases associated with mRNA vaccines are mild in nature and do not have serious complications and require only a few days of hospital admission.” Several studies (here, here, and here) have compared the severity of vaccine-myocarditis to COVID-myocarditis and classic viral-myocarditis. These studies all found that vaccine-myocarditis was by far the mildest, which is not a surprise given its generally favorable prognosis.
Patients with vaccine-myocarditis fare better than those with COVID-myocarditis.
A New Study
Another recent study, Clinical Outcomes of Myocarditis After SARS-Cov-2 Mrna Vaccination In Four Nordic Countries: Population Based Cohort Study, again confirmed the unsurprising news that vaccine-myocarditis is milder than viral-myocarditis. The study used a Nordic myocarditis cohort and examined 7,292 patients 12-years or older who had a diagnosis of myocarditis as a main or secondary diagnosis from 2018-2022. Anyone admitted to hospital for myocarditis within 28 days of vaccination with a mRNA vaccine was categorised as having vaccine-myocarditis, while patients admitted to hospital for myocarditis within 28 days of a positive SARS-CoV-2 PCR were categorised as having COVID-myocarditis. The study found:
Among patients aged 12-39 years with no predisposing comorbidities, the relative risk of heart failure or death was markedly higher for myocarditis associated with covid-19 disease than for myocarditis associated with vaccination.
This all seems pretty straightforward. While vaccine-myocarditis can make young people sick, COVID-myocarditis can make them much sicker. Though myocarditis is rare from both the vaccine and the virus, when tragedies occur, the virus is always to blame.
Contrarian Doctors Misinform
However, one aspect of the Nordic study allowed contrarian doctors to claim its authors did not understand their own results. In this study, 530 (7.3%) patients had vaccine-myocarditis, 109 (1.5%) had COVID myocarditis, and 6,653 (91.2%) had conventional myocarditis. Since 530 is larger than 109, contrarian doctors concluded the vaccine was more dangerous than the virus.
Dr. Tracy Hoeg, who boasted on Twitter about her child getting both COVID and chickenpox, composed a long Twitter thread that concluded, “the overall risk of developing myocarditis post vax appears higher post vax than post covid.” Dr. Marty Makary, who said herd immunity arrived in spring 2021, spread Dr. Hoeg’s misinformation and added:
The myth that myocarditis was more common after covid than after the vax was propagated by the medical establishment with poor studies of vax-associated myocarditis that had low capture methodology. Hundreds of thousands of young ppl got myocarditis for no good reason.
In reality, no hospital in the world had to open a vaccine-injury unit, though many were deluged with sick children at multiple points during this pandemic.
Dr. Anish Koka, a cardiologist who thought concerns about the Delta variant’s impact on children were 😂, said:
COVID myocarditis = mostly older ppl with bad hearts that spill troponins. Their prognosis is bad. Comparing their prognosis to the teenager that has vaxx myocarditis makes not a whole lot of sense.
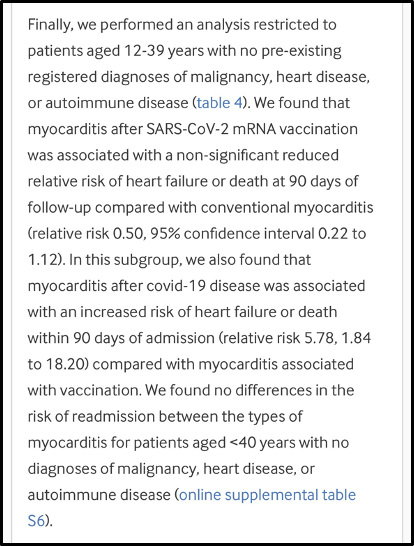
Dr. Koka is right that it makes no sense to compare cardiac outcomes in older patients with COVID to younger men with vaccine-myocarditis. That’s why the authors did this:
Doctors Inform
Unsurprisingly, there were some serious problems with the musings of Drs. Hoeg, Makary, and Koka. Most importantly, the Nordic study was a study on the severity vaccine-myocarditis versus COVID-myocarditis. It was not designed to determine the respective rates of these conditions. It did not present the denominators, namely how many people were vaccinated versus how many tested positive for SARS-CoV-2 via PCR. These numbers were not the same. As Dr. Bob Morris pointed out:
What Dr. Hoeg is dutifully missing here is that this study was not designed to compare vaccine induced myocarditis rates to COVID induced rates. It was designed to compare severity. She is completely misrepresenting the study results…
During the study period, the Scandinavian countries had an average of 1200 cases of COVID per 100,000 people and delivered 8200 vaccine doses/100k people every 4 weeks. In other words, every 4 weeks 8.2% of people got a shot. 1.2% were diagnosed with COVID. SO, IF MYOCARDITIS WERE COMPLETELY UNRELATED TO COVID OR THE VACCINE, WE WOULD STILL EXPECT 8.2% OF CASES TO HAVE BEEN VACCINATED AND 1.2% TO HAVE BEEN DIAGNOSED WITH COVID IN THE PRECEDING 4 WEEKS.
Dr. Jeffrey Morris similarly noted:
There are no denominators, but at end of 2022 for vaccines would be ~63 million doses, and for infections be ~9 million PCR+ infections, so they are not equivalent.
Moreover, the Nordic paper only included subjects with a diagnosis of myocarditis as a main or secondary diagnosis. In other words, someone hospitalized with COVID and myocarditis that was not severe enough to rank as a main or secondary diagnosis would not be captured by this study. Sick COVID patients can have a dozen things wrong with them, I am certain that this study missed many cases of COVID-myocarditis.
The distortions spread by contrarian doctors were so egregious that Dr. Anders Hviid, the paper’s senior author, was forced to respond. After reading Dr. Koka’s obviously false assertion that he compared COVID-myocarditis in older patients to vaccine-myocarditis in younger patients, Dr. Hviid said:
But that is not what we have done?! Our primary reference grp is conv. myo. Comparing vaxmyo vs c19myo directly, we restrict to “individuals aged 12-39 years, with no predisposing comorbidities”.
Dr. Hviid later felt obligated to make an announcement that said:
PUBLIC SERVICE ANNOUNCEMENT. Our recent study on myocarditis is a prognostic study of myocarditis patients. It is NOT a study designed to compare excess risks of myocarditis following vax vs inf. Please interpret responsibly.
“The point of our study is that vax myo does not carry the same risk of HF (heart failure) and death as other types of myo”, he added.
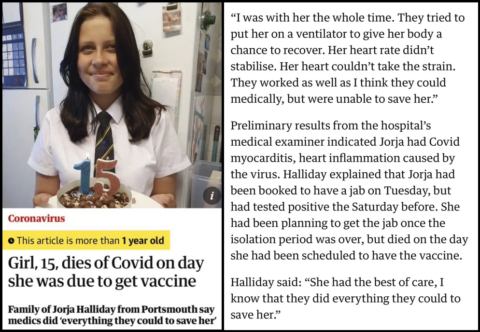
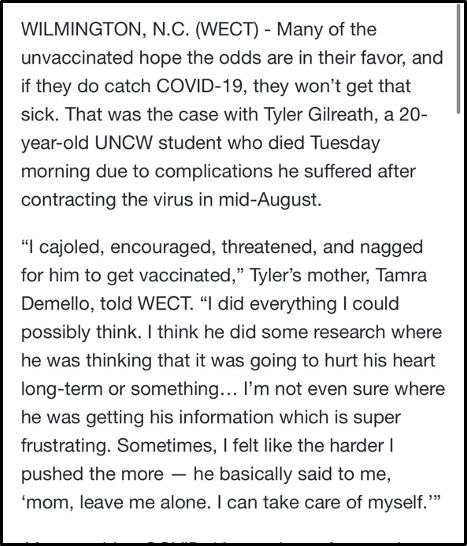
Beyond this, even if Dr. Hviid’s study somehow showed that vaccine-myocarditis was more common than COVID-myocarditis, that is not the proper comparison. The proper comparison is which can do more harm overall, the vaccine or the virus. Dr. Hviid’s paper showed once again that COVID-myocarditis is much more severe than vaccine-myocarditis, though this understates the risk of SARS-CoV-2 whose harms are not limited to myocarditis. Tyler Gilreath, a healthy 20-year-old, died of a brain abscess after getting COVID, not myocarditis. He didn’t get vaccinated because he was worried about myocarditis though.
Though Drs. Hoeg, Makary, and Koka will never inform their audience of this, some children have needed amputations or lung transplants after their bout with COVID. Others have had strokes. The virus has killed hundreds of teenagers, and teenage athletes have died of COVID after the vaccine was available to them. No children are known to have died from the vaccine, which has proven effective at limiting COVID’s greatest harms, including death. Say what you will about vaccine-myocarditis, it shouldn’t be controversial to state that it is less severe than death. Yet, this is a very controversial opinion amongst doctors.
Let’s review one of the study’s core conclusions:
Among patients aged 12-39 years with no predisposing comorbidities, the relative risk of heart failure or death was markedly higher for myocarditis associated with covid-19 disease than for myocarditis associated with vaccination.
It’s a sad commentary on our pandemic discourse that doctors -who will never care for a sick child themselves- twisted this result to scare parents away from vaccination. Dr. Hviid had to spend his time correcting obvious misinformation spread not by random internet quacks, but by doctors with large social media followings and access to powerful politicians (Florida/Virginia). I’m sorry he had to see his research misrepresented this way.
Those of us who were aware of unsavory characters like Sayer Ji before the pandemic knew to double check his every claim. It is now necessary to do this with many doctors as well.
Dr. Sabina Vohra-Miller summarizes this essay