
This is the third installment of debunking the book “Turtles All the Way Down” (written by “Anonymous”, and edited by Children’s Health Defense lawyer Mary Holland and Children’s Health Defense Publisher Liaison Zoey O’Toole). Because this is a fairly long book, I’ll be spreading my posts out over 10 more reasonably digestible pieces. This is the next installment in the series – debunking Chapter 3 “Deficient by Design: The Vaccine Adverse Event Reporting System (VAERS)”.
As in the previous two installments, I will present quotes or paraphrases of statements from the chapter with their associated debunks, and answers to the questions at the end of each chapter. Statements that are repetitive will be addressed only once or twice even though they might appear several times within the chapter.
1. VAERS suffers from underreporting bias:
This is partially true in that nobody will deliver a VAERS link to your doorstep and solicit reports, however there are multiple means at the public’s disposal to report what they believe to be adverse events. VAERS is a passive surveillance system, meaning it relies on voluntary reporting.
It is certainly now widely known that during the COVID pandemic, systems were at times slow to react to potential vaccine associated side effects. For example, it took a certain period of time for vaccine associated myocarditis to be recognized by all major national health systems. Even mainstream physicians can get behind the call to ask for VAERS reports to be acted upon more quickly.
However, this thought process – which pervades this chapter – has a big logical hole in it: VAERS is not designed nor was it intended to be acted upon alone. It is intended to be used in conjunction with the national and international vaccine reporting databases such as the Vaccine Safety Datalink, university researchers, the British Yellow Card system, the European EMA, and similar systems in other countries.
One of the few times the Vaccine Safety Datalink is mentioned, the authors claim that its data being “concealed forever”. If this were genuinely true, like how classified data is concealed forever, nobody would be able to produce any research projects from it. The VSD is open to any competent researchers with the CV adequate to analyze the data. Contrary to the beliefs of the authors, there is no effort to constrain researchers from using the VSD – a wide variety of researchers have written studies based upon this active surveillance database. Anyone with the academic credentials to design a well thought out research project from the VSD may use it. Contrary to the belief that vaccine safety researchers are willfully blind to rare adverse events, the people who are actually employed to research these side effects are actively thinking about the ways they could be missing blind spots and side effects not easy to spot.
An example of VAERS working as it was intended to work
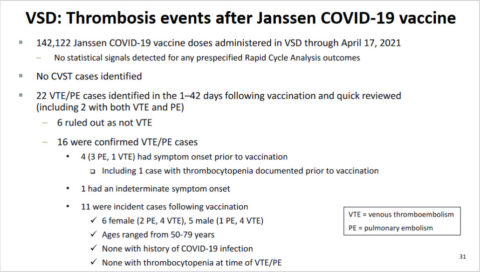
Let’s look at a specific serious but rare vaccine side effect – vaccine-induced thrombotic thrombocytopenia – and the viral vector adenovirus COVID-19 vaccine from Johnson & Johnson. On April 13, 2021, the CDC issued a Health Alert regarding Cases of Cerebral Venous Sinus Thrombosis with Thrombocytopenia after Receipt of the Johnson & Johnson COVID-19 Vaccine:
The Centers for Disease Control and Prevention (CDC) and the U.S. Food and Drug Administration (FDA) are reviewing data involving six U.S. cases of a rare type of blood clot in individuals after receiving the J&J COVID-19 vaccine that were reported to the Vaccine Adverse Event Reporting System (VAERS). … All six cases occurred among women aged 18–48 years. The interval from vaccine receipt to symptom onset ranged from 6–13 days. One patient died. …
CDC will convene an emergency meeting of the Advisory Committee on Immunization Practices (ACIP) on Wednesday, April 14, 2021, to further review these cases and assess potential implications on vaccine policy. FDA will review that analysis as it also investigates these cases. Until that process is complete, CDC and FDA are recommending a pause in the use of the J&J COVID-19 vaccine out of an abundance of caution. …
Further extensive review followed, including comparing cases with VSD:

Subsequently, the pause was lifted on April 23. 2021, and information about the rare side effect was added to the Fact Sheets for healthcare providers and patients. The CDC continued to investigate and monitor cases and by December 2021 calculated an incidence rate of 1/100,000. Subsequently:
In December 2021, after reviewing updated vaccine effectiveness and safety data, the ACIP [Advisory Committee on Immunization Practices (ACIP) – CDC] made a preferential recommendation for the use of mRNA COVID-19 vaccines over the Janssen COVID-19 Vaccine in all persons 18 years of age and older in the United States. The ACIP recommended and CDC endorsed that the Janssen COVID-19 Vaccine may be considered in some situations: when a person has a contraindication to receipt of mRNA COVID-19 vaccines, when a person would otherwise remain unvaccinated for COVID-19 due to limited access to mRNA COVID-19 vaccines, and when a person wants to receive the Janssen COVID-19 Vaccine despite the safety concerns identified.
Based on continued monitoring and research, on May 5, 2022, the J&J vaccine EUA was modified to restrict candidates for this vaccine to “individuals 18 years of age and older for whom other authorized or approved COVID-19 vaccines are not accessible or clinically appropriate, and to individuals 18 years of age and older who elect to receive the Janssen COVID-19 Vaccine because they would otherwise not receive a COVID-19 vaccine.” As of May 10, 2023, this vaccine is no longer available in the US. All this work started with reports to VAERS.
When all the vaccine pharmacovigilance databases are used together, they work as intended. It’s easy to complain that a BMW sports car cannot tow a tractor, but that is only if you have unrealistic expectations.
2. VAERS cannot detect small adverse events:
It is possible to have empathy with those who encountered genuine vaccine related adverse events while also insisting on systematic, rules-guided research on this issue. This statement is mathematically illogical – VAERS, on its own, does not provide a denominator (total number of vaccine recipients). Other systems such as vaccine logs, are necessary to provide that number. People who had a great experience after vaccination generally are not on VAERS describing how uneventful their experience was.
This statement is wrong on several other levels as well: Studies that originated from VAERS data revealed small signals of intussusception with an older rotavirus vaccine, suspicion of corneal graft rejection after COVID immunization, VITT after COVID immunization, and an Australian study of fainting after HPV vaccination. This is obviously a non-exhaustive list.
3. Anyone can report to VAERS/ VAERS is passive reporting:
This is a double-edged sword. It is possible for dishonest actors to encourage false reporting to VAERS at any time, although Dr Shimabukuro, the CDC deputy director, advises us that there is no current evidence of widespread systematic gaming of the system. It is also accurate that this is a “passive surveillance” system, in that anyone is invited to report. However, the system does not actively solicit the recording of adverse events, in the same way V-Safe, a system implemented during the rollout of the COVID vaccines, solicits reports.
Prospective researchers who want to use VAERS should acknowledge that its “open door policy” does allow as many reports as the public is willing to write up, but that appropriate work is necessary to filter out reports that do not make biological sense, are clearly not vaccine related, or are clearly fraudulent — for example the report of a vaccine turning a man into the Hulk.
People who run databases that mirror VAERS (like OpenVAERS) know this – you have to acknowledge that you’ve read the warning on the official VAERS website before you can access the data. But again, I remind the reader that the main goal of the antivax ecosystem is to stir up as much fear as possible about vaccines, without any thought as to whether that fear may have any validity.
Liz Willner, the author of OpenVAERS, theoretically knows to not regard VAERS reports as stand-alone proof of causality, but she and other like-minded people prefer to de-emphasize this. The number of safe vaccines for a dedicated antivaxxer is, has, and always will be zero. These people face absolutely no consequences when someone listens to their advice and contracts a vaccine-preventable disease.
4. The promise of vaccine adverse event reporting systems has not been realized because these systems are intentionally designed to be unable to fulfill their stated mission of monitoring vaccine safety:
See points #1 and #2 above. It is easy to criticize a BMW X5 for being unable to tow a tractor, but that is if you have unrealistic expectations.
5. Questions to ask your doctor:
Are you familiar with the VAERS system? Have you ever filed a case with VAERS?
As a cardiologist I am happy to report suspected cases of vaccination myocarditis to VAERS and respond to their requests for clinical discussion. I encourage other pediatricians to use it as well. Any physician who administers vaccines has to be aware of VAERS. Whether they’ve ever filed a report will depend on whether they’ve observed a reportable event (see below).
If your patient experiences an adverse health event following vaccination, do you check VAERS for reports of similar symptoms before deciding how to proceed with the case? Do you report it to VAERS?
All healthcare providers are required to report certain adverse events to VAERS (see below). If a patient experiences an event following vaccination that doesn’t meet those requirements, it is reasonable to check VAERS personally, before deciding how to proceed with a possible vaccine adverse event case, but this should be done in conjunction with other research as well.
Do you think healthcare professionals should be required by law to report adverse health events following vaccination, similar to their obligation to report cases of notifiable infectious diseases
This aspect of VAERS as represented in the book is a clear misrepresentation. Healthcare workers are already required by law to report certain adverse events:
Under the National Childhood Vaccine Injury Act (NCVIA), healthcare providers are required by law to report to VAERS:
- Any adverse event listed in the VAERS Table of Reportable Events Following Vaccination [PDF – 5 Pages] that occurs within the specified time period after vaccinations
- An adverse event listed by the vaccine manufacturer as a contraindication to further doses of the vaccine
Healthcare providers are strongly encouraged to report to VAERS:
- Any adverse event that occurs after the administration of a vaccine licensed in the United States, whether it is or is not clear that a vaccine caused the adverse event
- Vaccine administration errors
Healthcare providers who administer COVID-19 vaccines are required to report additional adverse events:
- Serious AEs regardless of causality [emphasis added]. Serious AEs per FDA are defined as:
- Death
- A life-threatening AE
- Inpatient hospitalization or prolongation of existing hospitalization
- A persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions
- A congenital anomaly/birth defect
- An important medical event that based on appropriate medical judgement may jeopardize the individual and may require medical or surgical intervention to prevent one of the outcomes listed above
- Cases of myocarditis after a Pfizer-BioNTech, Moderna, Novavax, or Janssen COVID-19 vaccine
- Cases of pericarditis after a Pfizer-BioNTech, Moderna, Novavax, or Janssen COVID-19 vaccine
- Cases of Multisystem Inflammatory Syndrome in children and adults
- Cases of COVID-19 that result in hospitalization or death
Healthcare providers are encouraged to report to VAERS any additional clinically significant AEs following vaccination, even if unsure whether the vaccine caused the event.
Certain side effects are common to most vaccines – sore arm, fatigue, fever, chills, headache, muscle and joint aches. They are usually short lived, lasting a day or two. They are also listed in the vaccine insert and described in the handout that the patient receives. However, it is not necessary for healthcare workers to report every possible sore arm and fever under the sun for the VAERS system to be able to generate information on such side effects, although it is reasonable to debate this particular point.
The fault, dear authors, …
Overall, this chapter is an attempt to explain how VAERS is inadequate to detect vaccine side effects without ever acknowledging that VAERS was designed to work in concert with additional active vaccine adverse event reporting systems. This information has been publicly available for decades. As demonstrated above, this synergy does work to detect vaccine side effects. That they do not produce the result the authors want to hear is not the fault of VAERS, it is the fault of the authors.
The complete series
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down” (part 1/10)
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down” (part 2/10)
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down (part 3/10)
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down (part 4/10)
{kind=link}