
If you haven’t heard about this book yet, it’s written by “Anonymous”, edited by Children’s Health Defense lawyer Mary Holland, Children’s Health Defense Publisher Liaison and Thinking Moms’ Revolution co-founder Zoey O’Toole, and published by “The Turtles Team”. It purports to use only mainstream references to prove its points, but the gist of the book is that they are hostile to all vaccines and will not stop until nobody gets vaccines anymore and all the mandates are removed.
Because this is a fairly long book that employs all of the antivaxxer tactics, I will spread my posts out into 10 more reasonably digestible pieces to show you how, as with all antivaxxer speeches, it is a paper tiger. This book has big promises but, to someone who actually knows the vaccine science, the book doesn’t really deliver much beyond money in the “Anonymous” author’s bank account. A more charitable interpretation of this book is a live masterclass of science denial/antivax techniques as explained here along with this illustration of the major tactics:
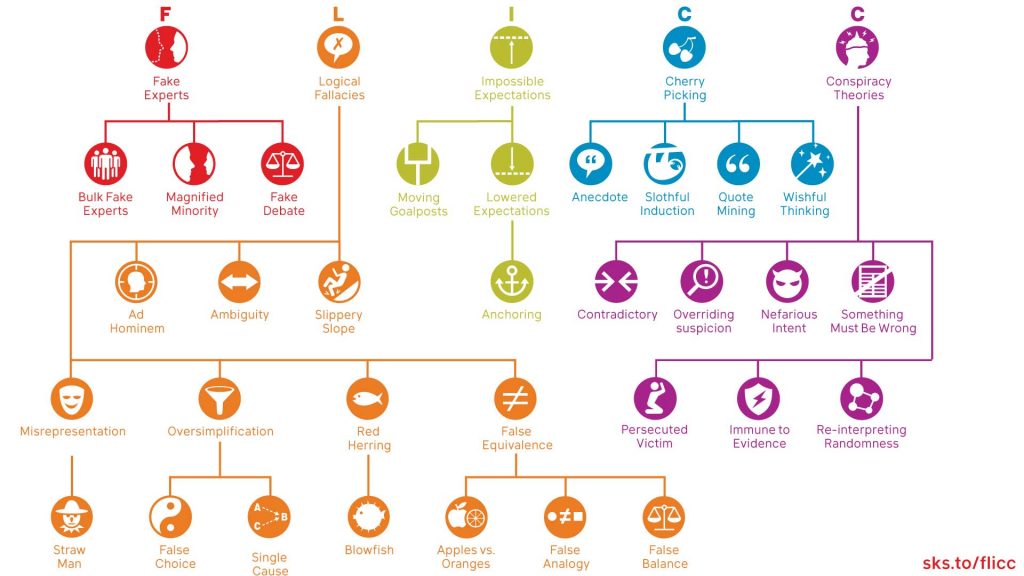
The general way these articles will be constructed is quotes with their associated debunks, and answers to the questions at the end of each chapter, that on first glance, appear to be gotcha questions, but actually are easy to answer with just a little extra medical knowledge. Statements that are repetitive will be addressed only once or twice (which is why not all of the debunks answer every single set of end-of-chapter questions).
If you only remember one thing from this series, remember that there is nothing one can say to a Children’s Health Defense board member, or a dedicated antivaxxer, that would convince them that vaccines are safe and effective. Science doesn’t work that way – even Mary Holland says, in this book, science must be willing to challenge old paradigms. That has been done several times over by dedicated scientists (for example, the removal of an old rotavirus vaccine for intussusception). It is actually CHD who is never willing to change their mind, because it would affect their income if they actually operated honestly.
1. “This paternalistic tendency is evident in long-standing attempts by scientific and medical entities to portray the public conversation on vaccines as a lopsided dispute.”
Actually, the reality is more complicated. Medicine does have a history of being paternalistic towards patients, which is something that even mainstream physicians cannot dispute. I will easily own up to our profession having this as a stain on its reputation in the past. This is why the entire profession has been coaching its medical students, nurses, nurse practitioners, pharmacists, and physician assistants, for an extremely long time, about how to make medicine more of a shared decision making process.
There still are times where it is medically necessary to be strict in giving out medical interventions – a classic example of this is a heart attack. A person actively having a heart attack is actively putting their life in danger if they were to reach for their Arizona homeopath instead of an actual interventional cardiologist trained and ready to help fix the heart artery blockage. Extreme paternalism is required to save a life in this case. At other times, it is medically necessary to give the patient a full explanation of what is going on, plus the risks and benefits of each type of treatment. After the explanation, a shared decision can be made.
How does this apply to vaccine science/research? A research reputation is not built by walking into a research meeting and saying “Hey listen to me, I know how the entire medical establishment got it wrong.” A reputation is built by consistently crafting research questions, creating the project that answers them, and interacting professionally with your colleagues to discover the correct answers (and hopefully eventually delivering that research breakthrough to patients).
Even physicians don’t get respect straight out of the box – those who go into vaccine research start out as nobodies, and have to prove their worth. Our professions are, from a certain perspective, kind of paternalistic to us as students/ junior physicians. Physician respect towards junior physicians is earned, bit by bit, from senior physicians. Mainstream physicians may seem paternalistic from the CHD’s perspective, but the requirement for vaccine debate is the same for everybody – the consistent application of the scientific method.
Let’s bring it back to the main point: once multiple research centers, national health departments, and medical professionals have researched a certain topic thoroughly, the burden is solely on the antivaxxer to prove their case using better scientific reasoning than what was previously provided. In every major vaccine, there is a very large body of literature demonstrating both their safety and utility/efficacy. It is not paternalistic to say to Children’s Health Defense that extraordinary claims require extraordinary evidence, and that being taken seriously at the professional vaccine discussion table requires a certain fee. The entry fee to the discussion table is democratic – scientific debate and a dedication to scientific reasoning is expected of all. Engaging in a vaccine debate first requires a semblance of shared reality, and next requires adherence to all the usual rules of science. Stating that vaccines are magnetic does not engender much enthusiasm from a mainstream physician in participating in debate.
2. “Clinical trials of vaccines are rigged to hide their true (and high) rate of side effects.”
The truth of the matter is that clinical trials – even for a well off “Big Pharma company” – require lots of laboratory, clinical, and financial resources to run. For the foreseeable future, probably all licensed vaccines will have side effects revealed that did not occur during the initial clinical trials submitted for FDA approval. This is absolutely not because any physician is “secretly smiling in a back room wishing for side effects”. Rather, there will always be side effects too rare to detect in the initial clinical trials. To detect a very rare event, a large number of people must be enrolled – and this is not always practically achievable by the chief investigator conducting a clinical trial for initial vaccine approval.
I am well aware of Big Pharma misconduct, and join all members of the public in celebrating each time a pharmaceutical company is penalized for such misconduct. However, based on resource limitations alone (and this is only just one of several reasons), it is not possible to design a million-person clinical trial for every vaccine in the future, or to seek out every possible side effect within one clinical trial (this is an explicit demand set forth in the book although not in these exact words).
How do we search for those rare side effects? This is why the various vaccine safety monitoring systems were set up, including the Vaccine Adverse Event Reporting System (VAERS), the Vaccine Safety Datalink (VSD), the Clinical Immunization Safety Assessment Project (CISA), the Post-licensure Rapid Immunization Safety Monitoring System (PRISM), and most recently V-safe. Ultimately, other research projects are done to detail how they think the side effect happened and how to potentially avoid it in the future. If a phase III clinical trial does not catch the side effect, the side effect monitoring system generally will. If mainstream physicians truly didn’t care about vaccine side effects, these monitoring systems wouldn’t exist.
3. “Adding a vaccine to the American schedule recommended by the CDC instantly guarantees sales of millions of units per year in the US alone, thus assuring its manufacturer a handsome return on its initial investment.”
At this point I would like to remind the audience that successfully bringing a new vaccine to the market requires an extremely large amount of clinical, laboratory, and financial resources. While COVID vaccines are uniquely profitable amongst vaccines, the vaccines against childhood vaccine-preventable diseases are actually one of the least profitable products for the companies that develop them. Vaccine proposals also fail all the time, meaning companies have invested considerable money and received no return.
While I understand the hostility to pharma-funded studies, what other solutions are available to achieve the funding required to complete such a project? It is the antivax community that claims to have the highest standard of safety required to approve a vaccine, and that requires money. Would Robert F. Kennedy Jr. agree to put up his own money to fund such projects? I have never heard of such a clinical trial funded by him. I have never heard what an antivaxxer would consider an acceptable funding source. Perhaps that would mean he would have to agree to a reassuring result, pointing to the safety of vaccines, which would go against his narrative.
If the antivax ecosystem genuinely cared about safety, they would not trawl social media posts insinuating that everyone who died in the news experienced a vaccine side effect (and in this case their fact-checking is so poor that someone they claimed died, didn’t actually die), assault actual pediatrician lawmakers, and create 24/7 media platforms distributing distorted information about vaccines. If they really cared, they would produce actual actionable peer-reviewed research on how to prevent a vaccine side effect, for example.
There is also no self reflection whatsoever, into the income of Del Bigtree’s Highwire, his customized bricks used to line the walkway of his ranch, or the income statements of Children’s Health Defense. I would encourage supporters of Bigtree to think about this for a second – he has requested payment to make bricks on his ranch engraved with the names of donors, so the names of the donors can be stepped upon. Let’s see if a dedicated antivaxxer can come up with a funding source agreeable to their community and produce successfully peer-reviewed research leading to a better solution than what we have currently.
4. Insistence of saline placebo for all vaccines
Dr. Gorski covered this claim in detail here. In the book it’s sort of implied that there have been no true randomized controlled trials for several classical vaccines, which is not true. If you don’t believe me, reference the package inserts for the influenza, pneumonia, HPV, rotavirus, and dengue vaccines. Each new vaccine requires a clinical trial to win approval under the regulations of each of our international health agencies (CDC, EMA, etc., etc.). The book’s authors also insist only the three-arm trial, or comparison to saline placebo, is the right way of doing clinical trials for vaccines. Both assertions are incorrect.
The regulatory burden of a new prospective vaccine candidate, if brand new, is to be better than a placebo “designed to resemble the test drug as far as possible except for the active ingredient”. But for a better vaccine, the comparison should be that it must perform better than its predecessor. A basic premise of the randomized controlled trial, the standard to aim for, in testing new medicines, is that there are two groups, one getting the real medicine, and one getting the “fake” medicine, to see how much better the real medicine is. One reason to use an old vaccine as a placebo is that if you just inject water, it will be easy for the study subjects to tell they had no vaccine. There is also this thing called the “double blind” trial, which means that the patients and the physicians both don’t know who is getting what. Then, the structure of the truly “double blind placebo controlled randomized controlled trial” is created. For a detailed discussion of the ethics of vaccine placebo, see this reference.
Remember – the Children’s Health Defense crew builds their brand on saying vaccines are always wrong and there is no way to test a vaccine that would satisfy them. This is not the position of a rational physician or basic scientist; in most things, we must be prepared to overturn paradigm. I fully realize these words are not explicitly spelled out on their website, but it is in fact spelled out through their actions. As adults in a free country, we are all entitled to our opinions, but the admittance fee to an actual scientific debate is dedication to scientific reasoning and the scientific method.
Mary Holland cares little for that. She will say anything to make people think vaccines are unsafe, regardless of whether or not this is grounded in reality. In this part of the book, they complain that there were no vaccines tested against placebo – this is a failure of very basic fact checking. Just one example can be found in the 9-valent Gardasil immunization that was tested versus a saline placebo. According to the World Health Organization, “Placebo use in vaccine trials is clearly acceptable when (a) no efficacious and safe vaccine exists and (b) the vaccine under consideration is intended to benefit the population in which the vaccine is to be tested.”
They then go on to insist on a “three arm” vaccine randomized controlled trial, while failing to realize that the modern HPV vaccine insert does in fact have data on such a trial where the amount of adverse events in the saline was no different from the plain adjuvant group. This is inconvenient to their narrative so it is naturally excluded.
Ethically, according to the WHO standard above, there are times when a vaccine placebo must be another vaccine – so certain vaccine trials are in fact done this way (specifically, when an older vaccine is available that can provide a bit of protection, it is ethically mandatory to do this rather than giving the patient water and leaving them vulnerable to a dangerous disease). Other vaccine trials are formulated to make the placebo equal in every way to the real vaccine being tested except for the thing intended to generate an immune response – one of the pneumonia vaccine RCTs is done this way.
The primary mission of a vaccine inventor in the eyes of a regulator is to prove a new vaccine improves upon an old vaccine in some way – this is the most direct reason why a placebo is often an old vaccine. The mission is not to prove the vaccine is more effective than plain water. Practically, it would constitute additional unnecessary steps to compare to saline placebo when the vaccine is supposed to be compared against its older predecessor.
5. There is little scientific merit in comparing results from different clinical trials.
The allegation stated in this part of the book is that two clinical trial covering the same topic must not be compared with each other (or with the general population) because there may be confounding variables that are not accounted for. Making such a statement means the authors either never tried to thoughtfully read the limitations section of a clinical trial, or have made a very poor attempt and are completely misunderstanding the point of having that section on a research paper.
Even our most well-respected clinical trials have issues that the authors describe at the end of their research paper. The authors always try to put their paper into context, and describe how their paper is supposed to contribute to the existing knowledge base. Authors also usually reference how they used the knowledge gained from other similar research projects to better answer the research question at hand. Sometimes the paper will provide a new perspective, or bring up an issue that wasn’t thought about before – all this will be explained in the discussions and results section.
Lastly, the authors will explicitly spell out how to compare their paper to similar papers using all the correct guardrails and design specifications of a scientific publication – meaning they will say what would be a good comparison versus an overgeneralization. The authors of the book completely missed all this.
We acknowledge differences in populations, and then compare when it is scientifically reasonable to do so, and always state in our article discussion sections the potential limits of such comparisons. This is a very large hole in the author’s comprehension of how collaboration between scientific institutions is conducted.
6. RCT control groups cannot be replaced with data from another trial, or any other externally calculated background rate.
The claim here appears to be that control groups are being removed after randomization and replaced with externally selected control groups. This is a misrepresentation of what is being done. In every phase 3 clinical trial, the subjects are randomized to test group and control, or some more complex variation of it – the COVID vaccine clinical trial for the original Pfizer vaccine is illustrative here, where their control group selection was described in great detail. Clinical trials are always going to be compared to external populations after the study is done, because that is the point of doing clinical trials in the first place. Why? The researcher wants to be able to generalize to the population. There are many different methods of post-approval surveillance, as mentioned earlier in this article.
Researchers regularly think about the benefits and pitfalls of comparing their studies to an external population; in fact this is regularly taught in public health training programs. That Mary Holland has failed to appreciate this is her fault alone. In addition, there is also the possibility of external investigators verifying or refuting the claims of the original clinical trial investigators. For example – we have pediatric cardiologists who discovered myocarditis as a consequence of the mRNA COVID-19 vaccines when the original investigators failed to do so. This is one of many examples of peer review/scientific debate in action.
7. “As we shall shortly see, this method (design a trial in which the reported rate of adverse events in the control group would likely be very similar to that of the trial group) is exactly the one vaccine manufacturers employ to deliberately obscure the real incidence of vaccine adverse events.”
When you have insufficient medical or research knowledge to put your reading of clinical trials into the wider overall context, you can come to a conclusion in line with any conspiracy theory you wish. There are several pieces of medical knowledge necessary to understand where this claim falls apart.
First, medical problems will occur before, during, and well after vaccine clinical trials, and for the future existence of all humanity. The “side effect free vaccine” is only a dream; in fact there are side effects to most every aspect of medical care/intervention (even choosing to do nothing, which may cause disease progression). To design a vaccine capable of never experiencing adverse medical events would require a vaccine against all disease, which would be amazing, but clearly an impossible demand of the medical ecosystem.
Next, it requires medical knowledge to distinguish a related from an unrelated adverse event – such knowledge can be acquired through careful study in medical school and careful medical investigation. A more straightforward example is coronary artery disease (the most common kind of adult heart disease) – it is not biochemically plausible or logical to claim that a diagnosis of coronary artery disease was the result of a pneumonia vaccine.
Next, the premise is that the usage of placebo substances that aren’t salt water (saline) allows the deliberate obfuscation of vaccine side effects. This premise is quite conspiratorial. The most obvious reason why is that vaccines have a long period, even after formal FDA and ACIP approval, where they are monitored for side effects, and if needed, valid side effects are added to the formal immunization label. The mRNA COVID-19 vaccines had myocarditis added to their immunization labels this way, and the adenoviral vector COVID vaccines had vaccine-induced thrombotic thrombocytopenia added to their labels in this manner.
Next, someone who claims there is an international conspiracy to hide side effects has never had to personally run a randomized controlled trial. In 2023, with modern computing and worldwide communications, whistleblowing and exposing misconduct is quite easy to do during a randomized controlled trial (even though this particular example did not really affect the final data analysis).
The author doesn’t quite come out and explicitly say it in this case, but they are talking this way because they are hostile to the aluminum adjuvant. They also forget that there are multiple ways to test adjuvant safety, that do not involve formal phase III randomized clinical trials. Next, there is no mention of the human safety of all the potential adjuvants that aren’t aluminum. Why no mention of all that testing? It would degrade their narrative.
Lastly in this section, they spend a lot of time talking about the testing of one of the rotavirus vaccines and again, lamenting that salt water was not used as the placebo in that particular clinical trial. By the way, this counts as an internal inconsistency – the book is OK with using sugar, salt, and water, as placebos, but they forget the placebo in this trial had as its major ingredients, sugar and water. They aren’t even willing to follow their own rules. When you have so many statements that are only lightly based in reality, it is difficult to keep track of them all.
8. The Nürnberg Code
This is an old favorite of antivaxxers, along with the revenge fantasy (where they hope to cause harm to physicians who advocate for vaccines). They believe most vaccine trials to be violations of the Code. The actual 1947 Code delineates what is considered to be acceptable medical experimentation on human beings. In clinical trials, nobody is being required to participate in pediatric vaccine trials. If a family did not want to, all they had to do is walk the other way. There is a very, very extensive informed consent process that occurs before enrolling a family in a pediatric vaccine clinical trial. It goes over the monitoring, tests to be drawn, doses to be given, randomization, how they plan on searching for side effects, known and theoretical side effects, and much, much more. Furthermore, the antivax ecosystem frequently forgets that this code is superseded by the Helsinki declaration.
9. Questions at the end of chapter 1 – these are framed as gotchas when they are actually quite easy for pediatricians to answer.
The questions are:
Was the vaccine that you are recommending tested in a pre-licensure clinical trial with a (real) placebo control group? If not, how do you (or anyone else, for that matter) calculate its true rate of adverse events?
The rate of adverse events is calculated by the clinical trials in addition to each nation’s pharmacovigilance system continually monitoring vaccine recipients for a long time after the formal national vaccine approval. The multiple logical errors in insisting on a “true placebo” are explained earlier in this article. Not difficult for a pediatrician to look this information up and share with the family.
While there is plenty for a physician to memorize, a physician should not be graded solely by the volume of memorized information; rather a great pediatrician is a great diagnostician and knows how to put each piece of medical information into context. Physicians are certainly ready and willing to help any families interested in learning about vaccine science, but we insist that the science be learned systematically, just like any other scientific discipline.
The true rate of adverse events is going to be first calculated by the initial clinical trial investigators, which is a number provided in the published study. As was illustrated by the distribution of the COVID-19 vaccines, myocarditis was an adverse event not well captured by the initial clinical trials. The most accurate age-stratified rates of myocarditis were calculated by independent investigators studying the issue at the population level and are now all available to discuss with your physician if desired.
Is it morally acceptable to conduct a clinical trial in infants for a new vaccine, where the “control group” receives an untested compound, i.e., the vaccine-sans-antigen, which is likely to cause irreversible side effects and has no potential benefit?
Is it morally acceptable to fully expose children to the risks of vaccine preventable disease? I would hope it is not political to say no to that. The placebo contents are examined by researchers and regulators using multiple tools, not just the randomized control trial, to specifically assess the risk of side effects.
I will gladly acknowledge the existence of vaccine-associated adverse events, having diagnosed vaccine myocarditis myself in my clinical practice. One that is more germane to infants is Dravet Syndrome in which some infants are just predisposed to have fevers accompanied with seizures. This is nobody’s fault – they just have a genetic problem with a certain aspect of their brain electricity. This can look absolutely terrifying to the parent seeing this for the very first time, but this can also mean that the infant would have a seizure if they had a fever with the real disease. Pediatric neurologists are quite capable of keeping kids as safe as possible from seizures. Do I like to see kids get this? Of course not, but a holistic interpretation of all the potential benefits of not having vaccine preventable disease is also necessary. This chapter does none of those things.
Vaccine myth and no science
This first chapter tried to explain how vaccine clinical trials are “turtles all the way down” – a phrase that implies claims of vaccine safety are based on a very shaky foundation. But the authors did an incredibly poor job of making their case, from not even being able to follow their own rules, to creating clearly impossible demands, to forgetting the rules of even very simple fact checking, to at times making interpretations that are entirely contrary to acceptable scientific practices.
All of us in pediatric medicine are aware of the shortcomings of the currently available vaccine science, which is why the quest to make the better vaccine is a never-ending quest. The authors of the book make little to no effort to sincerely understand why current vaccine clinical trials are done in the manner that they are, and even attempt to complain that things were not done that were actually done. The authors of the book make little sincere effort to make a substantive contribution to advance vaccine science in a way that would suit their demands. This sets the scene for the debunking of the remainder of the book – and a promise to the reader that more biting commentary is to come in the other 9 parts of this debunk.
The complete series
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down” (part 1/10)
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down” (part 2/10)
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down (part 3/10)
- The Grand Debunk of the antivaxxer book “Turtles All the Way Down (part 4/10)
{kind=link}