{kind=link}
Over the years, our bloggers here at Science-Based Medicine have written time and time again about the intersection of law and science in medicine. Sometimes, we support a particular bill or law, such as laws to protect children against religion-inspired medical neglect; laws making it harder for manufacturers of homeopathic “medicines” to deceive the public; or California Bill AB 2109, a bill whose intent was to make it more difficult for parents to obtain nonmedical exemptions to vaccine mandates but whose implementation after being passed into law was profoundly sabotaged by Governor Jerry Brown. or, more recently, California SB 277, a bill currently wending its way through the California legislature that would eliminate nonmedical exemptions to school vaccine mandates and has, not surprisingly, engendered extreme resistance from the antivaccine crowd, including by Robert F. Kennedy, Jr. In the vast majority of cases we explain how the law lets us down when it comes to science in medicine, and, unfortunately, examples are many: Naturopathic licensing laws; supplement regulation (or, more appropriately, lack of regulation); misguided, deceptive, and patient-hostile “right-to-try” laws; state laws regulating medical practice that allow quackery to flourish unchecked; laws regulating pharmaceutical cost transparency that ask the wrong question.
The case I will discuss here is unusual in that it is a case of the law getting ahead of what the science says in a manner that will likely do little, if any, good for patients, cause a lot of confusion until the science is worked out better, and end up costing patients money for little or no benefit. I am referring to laws mandating the reporting of high-breast-density to women with dense breasts undergoing mammography. These laws are sweeping the country (albeit not as rapidly as “right-to-try” laws), with a total of 22 states having passed them as of today since Connecticut became the first to do so in 2009. The most recent of these laws went into effect in my own state of Michigan exactly one week ago:
Women with dense breast tissue — the sort that can hide potentially deadly tumors from routine mammograms — must be notified in writing and encouraged to consider additional tests under a new state law that is effective Monday.
While mammograms remain the gold standard for detecting breast tumors, they’re less reliable in almost half of women with dense breast tissue. Dense or fibrous tissue shows up as splotches of white on a mammogram — so do tumors.
That will likely surprise many of the millions of women who rely on mammography for catching the earliest signs of cancer, said Nancy Cappello. The Connecticut woman was shocked in 2004, when her gynecologist found a lump — advanced cancer that had already spread to her lymph nodes — just months after a mammogram deemed her cancer-free.
Yes, mammography is imperfect, and we here at SBM have not shied away from describing its imperfections (or the difficulties in general with screening asymptomatic patients for any disease) including one large study that found no reduction in breast cancer-related mortality that was relentlessly (and falsely) attacked as fraudulent by a prominent radiologist. Regular readers know that the sensitivity of mammography is not optimal, and that it likely results in significant overdiagnosis and overtreatment, particularly of the pre-cancerous entity known as ductal carcinoma in situ (DCIS). All these issues aside, a review by the World Health Organization (WHO) International Agency for Research on Cancer (IARC) of mammographic screening hot off the presses last week in the New England Journal of Medicine nonetheless concluded that, for women between the ages of 50 and 74 at least, there is sufficient evidence to conclude that mammographic screening results in a significant reduction in the risk of dying of breast cancer, although the same report affirmed doubts about the adequacy of evidence for women between the ages of 40 and 49 that the USPSTF originally used in 2009 to base its recommendation that mammographic screening not begin until age 50 for most women. In other words, mammography, as imperfect as it is, does reduce the risk of death from breast cancer in women over 50.
Breast density, mammography, and cancer risk
It has long been known that mammography tends to be less effective in women with dense breasts. What is causes “density” on mammographic imaging is the high level of fibrous and glandular tissue relative to fatty tissue compared to breasts that are not considered dense. The reasons why mammographic screening of dense breasts might be less effective are fairly simple to understand. Mammography is basically an X-ray of the breast taken in a specified, highly standardized manner. As such, the image rendered shows up as areas of white and dark, with the white representing denser tissue and the dark less dense tissue, usually fat, which lets X-rays pass through easily. Lesions suspicious for breast cancer manifest themselves as a density that stands out among the darker, less dense tissue, of which there are two kinds: a tissue density or calcifications. I could ramble on and on and on about what characteristics make a tissue density or an area of calcifications suspicious and another area of tissue density or calcifications benign-appearing (or at least much less suspicious). The details aren’t important for purposes of this post. What is important for purposes of understanding the effect of mammographic density on the ability to detect cancer is that it depends on the contrast between the denser lesions that are suspicious for cancer and the surrounding breast and fatty tissue. The less contrast there is, the harder it is for the radiologist, even with computer-aided detection, to differentiate between suspicious lesions and normal breast tissue. That’s why mammography works really well in breasts that are largely replaced by fatty tissue, as is the case in many postmenopausal women, in whom dense breast tissue is less common than in premenopausal women. Basically, as estrogen and progesterone levels plummet, over time the glandular tissue in postmenopausal breasts becomes replaced with fatty tissue.
Just to give you an idea, here are images of breasts of low, intermediate, and high density on mammography:
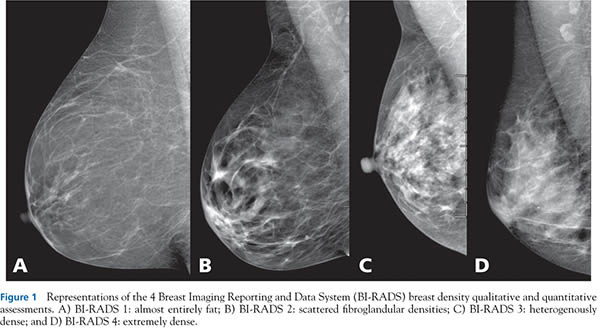
Breast density measurements
And here is an example of what microcalcifications look like:
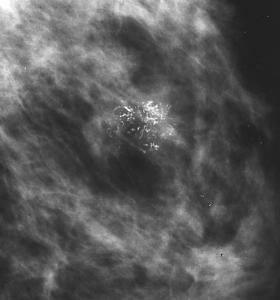
Microcalcifications
And of how breast cancers appear on mammography:
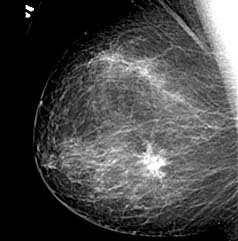
You can see how it would be more difficult to see these lesions in dense breasts, especially when they are more subtle and not as obvious. Indeed, the National Cancer Institute (NCI) points out on its website that the “main cause of false-negative results is high breast density.” In any case, the reason why mammography is more problematic in women aged 40 to 49 boils down to the fact that most premenopausal women have denser breasts due to higher levels of hormones and the incidence of breast cancer is lower, such that a positive finding is much more likely to be a false positive than a true positive than it is in older women. As I’ve explained before, for a screening program to be effective, the disease being screened for has to be sufficiently common for this not to happen. There’s a reason why even the most zealous supporters of mammography don’t recommend that routine screening begin before age 40; breast cancer incidence is just too low in this age group.
So far, so clear (I hope). However, recent science has thrown a new wrinkle into the equation. That science is the consensus that has emerged over the last couple of decades, based on numerous studies, that breast density is an independent risk factor for the development of breast cancer. In other words, women who have dense breasts, all other clinical characteristics being equal, have a higher risk of developing breast cancer. According to a recent review article, women with the highest breast density have a risk that is 2 to 6 times higher than women with the lowest breast density, and that as many as 30% of postmenopausal women still have dense breasts. Breast density correlates with a number of factors, including age (negative correlation), serum and tissue hormone levels (positive correlation), genetics, and body mass index (negative). Paradoxically, although high BMI is correlated with decreased breast density, obesity is correlated with an increased risk of breast cancer in postmenopausal women.
Because breast density is an independent predictor of breast cancer risk, naturally, the question has been asked what the biology is behind this and whether it is a modifiable risk factor. (Indeed, in the interests of full disclosure, I have been involved in a study that asks that very question and uses a new ultrasound technology to quantify breast density.) It is known, for instance, that Tamoxifen can decrease breast density, and it is also known that Tamoxifen can decrease the risk of breast cancer significantly in women at high risk. Are the two related? Does Tamoxifen’s ability to decrease breast cancer risk have to do with its ability to decrease breast density? We don’t yet know. Does the decrease in breast density due to Tamoxifen cause the decrease in risk or is the decreased breast density an epiphenomenon associated with the decreased risk? We don’t yet know. Does reduction in breast density over time correlate with decreased breast cancer risk? Yes, to some extent. A recent case control study, for instance, found that women who did not develop breast cancer showed a decrease in mammographic density between first and second prediagnostic mammogram compared to women who did develop breast cancer, who did not.
In other words, it’s complicated, and the science is far from settled. We know that breast density is associated with an increased risk of breast cancer, but the biology is not well understood, we don’t yet know if it’s a modifiable risk factor, and we don’t know the molecular basis. All we know are factors that are associated with increased breast density and that increased breast density is an independent risk factor for breast cancer. Research is ongoing and likely will be ongoing for quite some time before answers start to become clear.
Mandatory breast density reporting
It’s impossible to discuss mandatory breast density reporting laws without discussing the woman who started the movement, Nancy Cappello, PhD, and her organization Are You Dense? Advocacy, whose mission is described as:
To ensure that women with dense breast tissue have access to an early breast cancer diagnosis. To that end, women need to be informed of their breast density, the limitations of mammography to find cancer in dense breast tissue and the increased risk factor of dense breast tissue.
As described in the story I first cited above, Cappello’s gynecologist found a lump months after she had had a “negative” mammogram in 2004, and she was diagnosed with stage IIIC breast cancer. As she herself relates in a recent article, “Decade of ‘Normal’ Mammography Reports–The Happygram“:
I ate healthy, exercised daily, examined my breasts regularly, and underwent yearly mammography. I had no family history of breast cancer. In 2003, my annual screening mammogram was reported as normal, just as the decade of reports before 2003. I was faithful to my health care regimen; my routine annual gynecologic examination was 6 weeks later. As my physician was examining my breasts, she felt a ridge in my right breast and ordered diagnostic mammography and ultrasound. The diagnostic mammogram revealed nothing, but the ultrasound examination revealed a 2.5-cm mass. A breast biopsy confirmed invasive cancer, which was later verified as stage IIIC breast cancer. At the time of diagnosis, my tumor was more than 1 inch in size, and it had metastasized to 13 lymph nodes. The American Cancer Society reports the 5-year survival rate for stage IIIC breast cancer as 49%, compared with stage I at 88% [1]. I expected, in the event of a cancer diagnosis, an early stage because of my faithful program of annual screening mammography. I questioned my doctors as to what had happened. This was the first time that I was told that I had extremely dense tissue and that, as breast density increases, the sensitivity of mammography decreases.
I was stunned that my doctors knew about dense breast tissue and its impact on the effectiveness of mammography but had never informed me. I also discovered that my physician received reports generated by radiologists that included more details about my mammographic results and, as in most reports, my breast tissue composition. This information is usually not reported in the patient’s “happygram” report. My decade of radiologists’ reports, unknown to me, read, “Patient has extremely dense breasts…no change from prior exam.” My radiologist knew that I had dense breasts. My doctor knew that I had dense breasts. The only person who did not know was me: the woman with the dense breasts.
Regular readers who have been paying attention to my posts on mammography and screening know that there is a huge misconception in this story, namely the belief that catching a cancer earlier results in a better chance of survival. It’s a common misunderstanding, even among physicians. Clearly, Cappello doesn’t understand the concept of lead time bias, but she’s in good company. Neither do a lot of physicians. Basically, earlier detection can make survival after diagnosis seem longer even if the treatments used have no effect at all. It seems an opportune time to explain why this is by resurrecting one of my favorite explanations for lead time bias, by Aaron Carroll:
Let’s say there’s a new cancer of the thumb killing people. From the time the first cancer cell appears, you have nine years to live, with chemo. From the time you can feel a lump, you have four years to live, with chemo. Let’s say we have no way to detect the disease until you feel a lump. The five year survival rate for this cancer is about 0, because within five years of detection, everyone dies, even on therapy.
Now I invent a new scanner that can detect thumb cancer when only one cell is there. Because it’s the United States, we invest heavily in those scanners. Early detection is everything, right? We have protests and lawsuits and now everyone is getting scanned like crazy. Not only that, but people are getting chemo earlier and earlier for the cancer. Sure, the side effects are terrible, but we want to live.
We made no improvements to the treatment. Everyone is still dying four years after they feel the lump. But since we are making the diagnosis five years earlier, our five year survival rate is now approaching 100%! Everyone is living nine years with the disease. Meanwhile, in England, they say that the scanner doesn’t extend life and won’t pay for it. Rationing! That’s why their five year survival rate is still 0%.
As I’ve said before, I don’t think screening for breast cancer is useless. Neither does the WHO. It’s just that the relationship between screening, finding cancer earlier, and increasing cancer survival is not simple. Would finding Cappello’s cancer earlier have increased her chance of survival? There’s no way of knowing because she was one of the lucky ones who survived stage IIIC cancer. In fairness, her treatment probably would have been less brutal, but it’s impossible to know in any single case whether early detection would have made a difference.
So Cappello became an advocate, and a successful one. Over the last several years, she and her collaborators have successfully gotten notification bills passed in 22 states. The new law in Michigan is typical. In the case of a finding of increased breast density, it mandates that the patient receive a letter that states:
Your mammogram shows that your breast tissue is dense. Dense breast tissue is very common and is not abnormal. However, dense breast tissue can make it harder to find cancer through a mammogram. Also, dense breast tissue may increase your risk for breast cancer. This information about the result of your mammogram is given to you to raise your awareness. Use this information to discuss with your health care provider whether other supplemental tests in addition to your mammogram may be appropriate for you, based on your individual risk. A report of your results was sent to your ordering physician. If you are self-referred, a report of your results was sent to you in addition to this summary.
So what’s wrong with this? More information is always a better thing, right? Even if it’s vague and just tells the patient to discuss the matter with her health care provider? There’s more wrong than you might think.
The problem with mandatory breast density reporting laws
There are a number of problems that these laws produce. The most difficult to navigate problems include what to recommend for these patients and how to reassure them. The reasons are simple. First, there is as yet no standardization for determining breast density, and, indeed, measuring density is still a fairly subjective process that radiologists do, with rather high interobserver variability. It is true that there are now automated systems designed to estimate breast density using image analysis, such as Volpara (there are other competing software systems), but most breast centers don’t yet have them and still use the American College of Radiology BI-RADS lexicon. My breast center does (it’s an NCI-designated Comprehensive Cancer Center, after all), but most mammography centers do not. Over time, no doubt the whole process will become much more standardized, but until then there will remain a lot of subjectivity in breast density assessments.
More importantly, indeed, most importantly of all, there is no consensus as to what to do next. As described in an editorial by Marcia Javitt, Section Editor for Women’s Imaging Director of Medical Imaging, Rambam Healthcare Campus in Israel, no large randomized clinical trials have shown that breast cancer mortality is reduced by alternative screening and “although the use of alternative imaging techniques, such as breast ultrasound, breast MRI, digital breast tomosynthesis, and molecular breast imaging (MBI) may enable the detection of mammographically occult cancers in patients with increased breast density, refinement and validation are required for successful large-scale supplemental screening.” The American Cancer Society guidelines call for MRI screening in addition to mammography for women at high lifetime risk (20-25%) to develop breast cancer, but states there is “insufficient evidence to recommend for or against MRI screening” in women whose mammographs indicate extremely dense or heterogeneous breast tissue. Javitt also notes that the potential number of women who would need to be considered for additional imaging after being informed of having heterogeneously or extremely dense breast tissue could be huge, adding that “if all of these women opt for adjunct screening procedures, a staggeringly high number of alternative screening studies in the United States could overwhelm the available resources.”
One of the most commonly suggested alternative additional modalities to use, whole breast ultrasound, is highly operator-dependent and has never been shown to decrease breast cancer mortality, although it can increase the detection rate in dense breasts, but at a cost. For example, the American College of Radiology Imaging Network (ACRIN) 6666 trial showed that using breast ultrasound to supplement mammography in women with dense breast tissue and increased risk for breast cancer resulted in improved cancer detection (an additional 4.3 cancers per thousand women screened) at the cost of an increased recall rate, a large increase in the false positive rate, and reduced positive biopsy rate. Also, there was no control group, and the study only evaluated women at increased risk of breast cancer, not women of average risk. (Once again, in the interests of full disclosure, my cancer center has developed a 3D ultrasound imaging technology that we have high hopes for.)
And I forgot to mention: The vast majority of these laws do not mandate that insurance companies pay for additional screening, which is a big problem, since most insurers don’t cover additional imaging for women with “clean” mammograms. The Affordable Care Act doesn’t require it, and, with the exception of Connecticut, Illinois, New Jersey, and Indiana, states with these mandatory reporting laws don’t require it. So, in most states that have passed these laws, women who get these notices are faced with the choice of just living with it or paying out of pocket for additional testing that has not been validated as being able to decrease their risk of dying of breast cancer. For some tests, MRI for instance, that expense could be quite high.
Finally, not all dense breasts are created equal, if you’ll excuse the cliché. Some are truly high risk, and some are not. At a website set up by radiologists to try to navigate the vagaries of these laws, BreastDensity.info, there is a flow sheet that informs us that:
- If the report states her density is heterogeneously dense, this is associated with minimal risk above average (RR=1.2 compared to average breast density).
- If her density is extremely dense (also sometimes called simply dense), this factor doubles her risk of breast cancer compared to average density, similar to the risk associated with a family history of breast cancer in a mother, sister, or daughter. For example, having extremely dense tissue on its own raises the 10-year risk of breast cancer in the average 50 year old woman from 1 in 42 to 1 in 21.
It also goes on to point out that, in the absence of other risk factors associated with breast cancer, elevated breast density alone does not put a woman at high risk for breast cancer. For instance, a recent prospective cohort study with over 365,000 women found that, in the absence of other risk factors for breast cancer, high breast density alone has a rather modest effect on breast cancer risk, leading the authors to warn:
Breast density should not be the sole criterion for deciding whether supplemental imaging is justified because not all women with dense breasts have high interval cancer rates. BCSC 5-year risk combined with BI-RADS breast density can identify women at high risk for interval cancer to inform patient–provider discussions about alternative screening strategies.
The study also found that about half of all women with heterogeneously or extremely dense breasts did not meet the threshold for high rates of interval breast cancer and that the threshold of screening all women with heterogeneously dense breasts required 1,124 supplemental tests per additional cancer case detected. In other words, an emphasis on breast density alone is probably ill-advised based on what we know now.
I can understand why women like Nancy Cappello become activists. I really can. They think they’ve been wronged by the medical system and that they’ve discovered something that doctors either aren’t aware of or didn’t think important enough to tell them. Unfortunately, in the case of breast density that something is information that is both unreliable and does not as yet have a consensus about it over what to do. As a result, what they’ve done is advocate for laws that are ahead of where the science is, but not in a good way.