
{kind=link}
Dr. Vinay Prasad, an adult oncologist, recently ignited yet another social media kerfuffle with an article titled “Doctors Must be Honest with Parents About Unknown Risks of COVID-19 Emergency Vaccine”. Addressing experienced pediatricians as if they were first year medical students at best or dishonest charlatans at worst, he wrote that it is “vital that medical practitioners don’t exaggerate or embellish what is known in this moment”. In this article, he warned of vaccine-related myocarditis and quoted the highest reported rate (1 in 5,000) from an insurance company as if it were established fact, ignoring multiple studies that found much lower rates. However, the point of my article is not a point-by-point discussion of such flaws in Dr. Prasad’s article- science communicator Edward Nirenberg has already done this. Rather, while I agree with Dr. Prasad’s ultimate conclusion – “Most likely, vaccinating will end up being a benefit to kids” – the point of my article is to show that Dr. Prasad fails to meet the standards he set for other doctors when he makes statements such as, “It is also reasonable for a parent to decide to sit back and wait a bit for additional safety data to accumulate”.
Informed consent for the COVID-19 vaccine
To understand why, let’s examine the elements of informed consent and how this might apply to the COVID-19 vaccine for children. Informed consent requires patients be educated on several points:
- The risks and side effects of the proposed treatment;
- The benefits of the proposed treatment;
- The alternatives to the treatment, including the risks, side effects, and benefits thereof; and
- The risks of not receiving the proposed treatment.
I’ve discussed the vaccine with many young adults, and though I am not a pediatrician, I imagine my discussion with parents of young children would go something like this.
The good news is your child is almost certainly going to be fine no matter what. Still, I want to help you make the best decision. Since I don’t think too many children will be able to dodge the virus for the rest of their lives, the question we are facing is: Which is more dangerous to your child, the virus or the vaccine? Importantly, we docs don’t just suggest vaccines for no reason. I’ve never suggested anyone get the yellow fever, cholera, or the Ebola vaccine. These are fine vaccines, but your child has no risk from these diseases. So, there is no point in even risking a sore arm.
For COVID-19, however, the virus is clearly more dangerous than the vaccine. First let’s talk about the risks of the vaccine. The most common side effects are what you’d expect; a sore arm, fatigue, headaches, muscle pain, and a fever. These are unpleasant, but overall mild and temporary. The mRNA vaccines come with a risk of myocarditis after the second shot for young men. The exact frequency isn’t clear, but according to several studies, it’s somewhere between 1 in 7,000 to 1 in 10,000 boys after the second shot. It may be much less, perhaps 1 in 37,000, with Pfizer’s vaccine, which is the vaccine your child will receive, than Moderna’s vaccine.
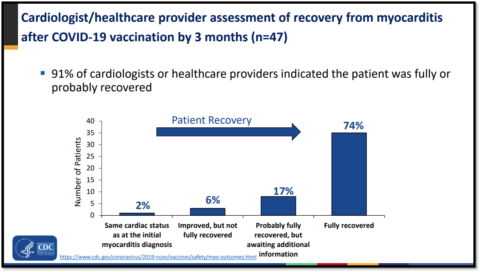
Most people with myocarditis are hospitalized for a few days, mainly for observation. Almost all are treated with simple treatments. In one of the largest studies, 95% of cases the clinical course “was generally mild, with resolution of myocarditis in most cases”. According to the CDC, 77% of affected people have recovered so far, and hopefully the rest are on the way to recovery. Affected individuals are advised to abstain from vigorous activity for a few months and monitoring is ongoing to see if there are any long-term cardiac consequences from this. We will know more about this next year than we do now. The issue should not be trivialized, though pediatric cardiologists have written that on follow-up, these children’s “cardiac MRIs that look very, very reassuring”. I am unaware of any deaths in adolescents from this vaccine, and many millions of them have been vaccinated around the world.
In contrast, according to the CDC’s COVID Data Tracker, the virus has killed over 900 children in the USA so far, and while most had common medical comorbidities such as asthma and obesity, about 20% of children who die of COVID-19 are healthy. Still, the risk of a healthy child dying of COVID-19 is extremely low, likely less than 1 in 100,000, though no one knows the exact number. Death is the worst outcome, but not the only bad one. Tens of thousands of children have been hospitalized, some very sick, needing ICU-level care and intubation. Over 5,500 children have developed MIS-C, and most of these children go to the ICU. These children can have a severe myocarditis and even acute heart failure. 48 children have died from this. Though they don’t need to go to the hospital, many other children just feel sick and rotten for a while. We have to be humble about the possibility of long-term consequences that we cannot currently appreciate. The vast majority of children do just fine with COVID-19 thankfully, but not all. This is also true for many viruses – even polio – and your child likely received vaccines against them already.
Happily, the vaccine is very effective at preventing these rare, but catastrophic outcomes in adolescents. A CDC study found that “Hospitalization rates were 10 times higher among unvaccinated than among fully vaccinated adolescents”. Another CDC study of hospitalized adolescents found that:
Among 179 COVID-19 case-patients, six (3%) were vaccinated and 173 (97%) were unvaccinated. Overall, 77 (43%) case-patients were admitted to an intensive care unit, and 29 (16%) critically ill case-patients received life support during hospitalization, including invasive mechanical ventilation, vasoactive infusions, or extracorporeal membrane oxygenation; two of these 29 critically ill patients (7%) died. All 77 case-patients admitted to the intensive care unit, all 29 critically ill case-patients, and both deaths occurred among unvaccinated case-patients.
Tragically, a number of unvaccinated teenagers have died of COVID-19 this summer after the vaccine was available to them. They and their parents did not know the risks of the virus and the benefits of the vaccine. These deaths were almost certainly preventable. Sadly, the same will be true for children ages 5-11 years who die moving forward. This is a very contagious virus that is spreading in many parts of the country now. Though rates are down from their peak, over 10,000 children are still getting COVID-19 every day in the USA.
Waiting for more safety data sounds nice, but while you wait, your child remains vulnerable. And this vaccine has been studied in children. The vaccine trial for younger children involved 2,268 children. The vaccine was 90.7% effective at preventing COVID-19. Overall, 3,100 children have received the vaccine as part of safety studies. The vaccine was safe in this study, though it was not large enough to detect rare side effects. As myocarditis is generally less common in young children compared to teenagers, vaccine experts are cautiously optimistic it will be less of an issue for them. Already, nearly a million children in the USA have received the vaccine. Vaccine experts voted unanimously to approve the vaccine, and every pediatrician I know was thrilled to vaccinate their own children as soon as possible.
I read many articles this summer of children’s hospitals being overwhelmed with children with COVID-19. I’ve never read any article about any hospital being overwhelmed with children suffering complications from the vaccine. The decision is yours, of course. We are on the same team here. We all just want to keep your child healthy and out of the hospital. The vaccine is the best way to do that. It’s a nice bonus that vaccinating your child will also help protect others and end the pandemic.
Doctors must be honest with parents about known risks of COVID-19
I am sure that pediatricians around the country are having some version of this talk countless times per day. They don’t need anyone to tell them how to do the most basic part of their job. They’ve been doing this for their entire careers. As one pediatrician said:
Pediatricians know their job is to present accurate and thorough information so parents can make informed decisions.
Perhaps then, instead of lecturing pediatricians and blocking them all on Twitter, Dr. Prasad should learn from them. After all, he is one of several contrarian doctors who has written extensively on COVID-19 and children while habitually neglecting to inform readers of crucial facts; namely that 900 children have died, that many thousands have been hospitalized, and that the vaccine works incredibly well at preventing severe illness in adolescents. These doctors, who assuredly consider themselves “pro-vaccine“, have no such reservations about repeatedly discussing vaccine myocarditis (here, here, here, here, here, here). In fact, it’s quite likely that the number of times they have discussed vaccine-related myocarditis exceeds the number of children currently hospitalized with the condition. Dr. Prasad was so concerned about vaccinated-related myocarditis he thought earlier this summer “that the US should suspend all vaccination in children under 18 and give only one dose of vaccine to men under 25”. The UK essentially adopted this policy, earning praise from Dr. Prasad for their “rationality & numeracy“. Shortly thereafter, the headlines predictably declared that “Children Drive Britain’s Longest-Running Covid Surge,” though Dr. Prasad hasn’t acknowledged this reality as far as I know.
Though he claims to support “language that empowers parents to take part in a shared decision-making discussion”, Dr. Prasad’s article did not enumerate how the virus has harmed children, nor did it inform readers that the vaccine can prevent these harms. I may have missed it, but I can’t recall any article by Dr. Prasad where he informs his readers of these basic facts. The closest he comes to acknowledging grave outcomes in children seems merely to rehash versions of the trite arguments that COVID-19 can’t be bad for kids because it’s worse elderly people (discussed here) and more children die of suicide (discussed here). Moreover, while Dr. Prasad’s article discusses the rate of vaccine-related myocarditis, it inexplicably neglects its generally favorable prognosis. Dr. Prasad wrote “it is absolutely essential that we communicate about this vaccine in an informative and nuanced way”. That sounds nice. So, where’s the information in his articles? Where’s the nuance?
Some people may argue that doctors writing for a general audience about children and the COVID-19 vaccine have different responsibilities from a doctor discussing the vaccine with a patient. I don’t see it this way. Any doctor with the privilege of writing in a major newspaper for an audience of millions has an obligation to be both accurate and thorough. As the principles of informed consent require, doctors should not just discuss the risks of the vaccine, but also the risks of the virus and the benefits of the vaccine. Leaving a child vulnerable to COVID-19 isn’t like driving drunk on a dark road at 120 MPH without a seatbelt. There’s no need to exaggerate the risk. But it’s not a risk-free proposition either. As he defends those who “decide to sit back and wait a bit for additional safety data”, I believe Dr. Prasad has an obligation to make it very clear what those risks are, especially considering 107,350 children contracted COVID-19 last week alone and 236 children have died in the past 3 months, according to the American Academy of Pediatrics. To paraphrase Dr. Prasad, doctors must be honest with parents about the known risks of COVID-19 and the known benefits of the vaccine.
This is incredibly easy to do of course. It only requires one paragraph and a writer who cares whether his readers are well-informed or not. Naturally, most doctors are thrilled to trumpet the studies showing the vaccine’s amazing success in keeping adolescents healthy and out of the hospital. Unfortunately, even though some parents are under the false impression that COVID-19 poses no risk to children, it’s clear some doctors don’t care about informing their readers. You don’t have to take my word for it, they readily admit this. As I discussed previously, one doctor even said that my concern was a “rather small nit to pick” and that providing readers with basic facts was a “waste of ink”. Perhaps they can write a rebuttal to this article and title it “In Defense of Omitting Facts”. It’s fine for a doctor to argue their viewpoint, of course, but writers who repeatedly exclude these facts should have their work read with this question in mind: “What information is the author omitting because it would undermine their argument?”
Dr. Prasad wrote, “This is not the time for uninformative persuasion”. I couldn’t agree more. I hope doctors like him start to communicate about this vaccine in an informative and nuanced way.