{kind=link}
Editor’s note:
I decided to take the holiday off. Fortunately, Dr. Howard was eager and itching to go with a post to fill in for me. In fact, Dr. Howard has been such a good and reliable contributor that we decided to make him a regular. He’ll be writing every other Friday, plus other days to fill in when there are gaps and/or he has something to say. We think Dr. Howard has been and will be an excellent addition to our stable of regular bloggers. Please join me in welcoming him aboard!
– David Gorski
I previously wrote about vaccine-myocarditis, and as the CDC recently gave new information on both the virus and the vaccine, an update is in order. As a reminder, myocarditis is inflammation of the heart muscle, and pericarditis is inflammation of the pericardium (the outer lining of the heart). It can be caused by a wide variety of infectious agents, toxins, and autoimmune conditions. It typically presents with chest pain and shortness of breath. Patients often have ECG abnormalities and elevated serum troponin levels, which are both markers of cardiac injury. Myocarditis is more common in young men and can be quite serious, even fatal, depending on the underlying cause.
The CDC’s data comes from two vaccine-safety monitoring systems: The Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD). Each of these two databases has their own strengths and weaknesses. According to the CDC, “VAERS accepts all reports from everyone regardless of the plausibility of the vaccine causing the event or the clinical seriousness of the event”. This makes VAERS useful to rapidly detect potential vaccine side effects that may be rare. But anyone can file a report, and even in the case of well-intentioned reports, it is not possible to establish cause and effect.
VSD surveys nine participating integrated healthcare organizations covering 12 million people. It is a public health surveillance activity that “Monitors a limited set of prespecified vaccine safety outcomes”. It is “Designed to detect statistically significant associations and statistical signals (values above specified statistical thresholds), which do not necessarily indicate a safety problem”. This database is not public as it contains confidential patient information.
There are three important questions. What is the rate of vaccine-induced myocarditis, what are the clinical outcomes, and how does this risk compare to that of the virus?
Vaccine-myocarditis rates
- The CDC’s VAERS report tallied 1,903 cases of myocarditis and 671 cases of pericarditis in all age groups by August 18th, 2021. The highest myocarditis rate was 1 in 14,000 in males age 16-17 after their second dose of the Pfizer vaccine. The rate was 1 in 23,000 for males age 12-15 and 1 in 27,000 for males age 18-24 years after their second dose of the Pfizer vaccine Interestingly, the myocarditis rate was 1 in 32,000 in males age 16-17 after their second dose of the Moderna vaccine. The myocarditis rate was less than 1 in 100,000 for females at any age.
- From CDC’s VSD report, the rate of myocarditis or pericarditis was 37 per 1 million children ages 12-17 years. If we assume that all cases occurred in boys, this yields a rate of 1 in 13,500.
- Another recent study of 6.2 million individuals using safety surveillance data from VSD study identified 34 myocarditis cases in patients 12-39 years old. Among patients 12 to 39 years old, there was a risk of 6.3 additional myocarditis cases per million doses during the first week after vaccination. Since almost all cases were in males, this translates to a rate of 1 in 79,000 for males in this age group. They myocarditis risk was higher with the Moderna vaccine.
- Data from Ontario showed a rate of 1 in 11,000 for males age 12-17 after their second dose and a rate of 1 in 6,100 for males age 18-24 after their second dose
- Data from Israel of people older than 16 years showed a rate of 1 in 37,000 people, and the average age was 25-years-old. However, this data was not stratified by age, and so we cannot deduce the rate for young males highest at risk. Israel previously reported a rate of 1 in 3,000-6,000 males ages 16 to 24.
Vaccine-myocarditis outcomes
While there is still uncertainly regarding the frequency of vaccine-myocarditis, outcome data continues to be consistently favorable in the short-term.
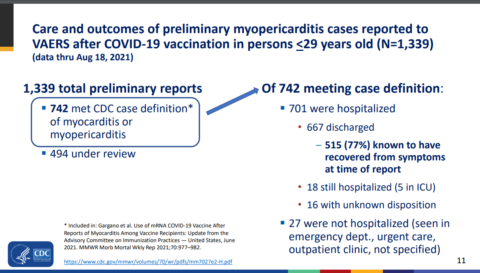
- In the CDC’s VAERS report, 701 out of 742 cases were admitted to the hospital. At the time of the report all but 18 had been discharged home and 5 of these were in the ICU. Typically this is done for monitoring, and no affected adolescents have needed life support as far as I know. 77% had no symptoms at the time of the report.
- The CDC’s VSD report reported on 56 individuals, and all had been discharged from the hospital usually after 2-3 days. 24 individuals were followed at least 7 days after discharge, and of these 6 still had at least one symptom.
- In the study of 6.2 million individuals using safety surveillance data from VSD, “82% were hospitalized (median length of stay, 1 day), and nearly all were recovered at record review…These results from our safety surveillance are reassuring,” said lead author Dr. Nicola Klein.
- According to reports from Israel, “Most cases have been in the hospital for up to 4 days, and 95% are considered to be mild cases.”
- According to reports from Ontario, “Most cases appear to be mild and respond well to conservative treatment (e.g. non-steroidal anti-inflammatory drugs) and rest”.
Other cases series report the following:
- “All patients in this series had a benign course; none required intensive care unit admission”. (Dionne et al)
- “Patients resolved their symptoms rapidly”. (Marshall et al)
- “Hospital course is mild with quick clinical recovery and excellent short-term outcomes”. (Jain et al)
- “All patients received brief supportive care and were recovered or recovering at the time of this report”. (Montgomery et al)
- The clinical course of vaccine-associated myocarditis-like illness appears favorable, with resolution of symptoms in all patients”. (Rosner et al)
- “The clinical course was mild in all six patients”. (Mouch et al)
- “All patients had resolution of their chest pain, were discharged from the hospital in stable condition, and were alive with preserved left ventricular ejection fraction at last contact”. (Larson et al)
Thus far 8.9 million adolescents have been vaccinated. The CDC investigated the deaths of several adolescents and concluded that they were unrelated to the vaccine, though six are still under investigation. Around the world, news from New Zealand reports the death of one woman due to vaccine-myocarditis and there is a report of a 42-year-old man who developed myocarditis two weeks after vaccination and died.
Almost all myocarditis cases occurred several days after vaccination, and there is no doubt the relationship is causal. Though the short-term outcomes for adolescents seems reassuring so far, individuals with vaccine-myocarditis had chest pain and many had shortness of breath. Though most recovered, about 25% had persistent symptoms at last follow-up. They had markers of cardiac injury and are almost always admitted to the hospital. As myocarditis can cause scarring, the potential for arrhythmias exists later in life and affected individuals will have to be monitored over the long-term. Additionally, affected individuals are advised to avoid strenuous physical activity for several months. As such, vaccine-myocarditis should not be trivialized.
Update on the virus
The virus causes myocarditis at a higher rate than the vaccine for children and young adults. According to a study from the CDC, 1 in 754 children younger than 16-years with COVID-19 were diagnosed with myocarditis, while the rate was 1 in 1,024 for people age 16-24 years. The study found that “The myocarditis risk is 37 times higher for infected children under 16 years and seven times higher for infected people ages 16-39 compared to their uninfected peers”.
Moreover, a total of 4,661 cases of Multisystem Inflammatory Syndrome in Children (MIS-C) cases have been reported thus far, and this may be substantial undercount. In one study of 191 children with MIS-C “53% had evidence of myocarditis, 80% were admitted to an intensive care unit and 2 died”. A systematic review of 15 case series/reports found that 75% of children with MIS-C have myocarditis. Complications such as coronary artery aneurysms frequently occur in children with MIS-C. Other studies have reported acute heart failure in children with MIS-C. Other common cardiac complications of myocarditis due to MIS-C include “shock, cardiac arrhythmias, pericardial effusion, and coronary artery dilatation”. Cardiac arrhythmias have led “to hemodynamic collapse and need for ECMO support” in some children. Though 41 children have died in the US from MIS-C, happily, most children seem to do well in the long-term.
Fortunately, the Delta variant does not seem to cause worse outcomes in children. The overwhelming majority of children who get COVID-19 will be fine, thankfully. The CDC found no increase in length of hospital stay or the percentage of hospitalized children admitted to the ICU with the Delta variant. They found that among 3,116 hospitalized children and adolescents with COVID-19 during March 1, 2020–June 19, 2021, 827 (26.5%) were admitted to an ICU, 190 (6.1%) required mechanical ventilation, and 21 (0.7%) died. Among 164 hospitalized children and adolescents with COVID-19 during June 20–July 31, 2021, 38 (23.2%) were admitted to an ICU, 16 (9.8%) required mechanical ventilation, and three (1.8%) died. According the CDC, “The differences in these indicators of severe disease between the two periods were not statistically significant.”
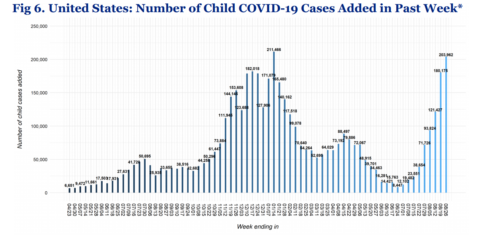
However, because the Delta variant is much more contagious, more children are getting sick now than ever before. According to the American Academy of Pediatrics, 203,962 child COVID-19 cases were reported from August 19th to August 26th, 2021. As a result, schools are being forced to close across many parts of the country due to COVID-19 outbreaks (e.g. Kentucky, Florida, Texas, Georgia, North Carolina, Mississippi, Alabama, South Carolina, Tennessee, Missouri, West Virginia).
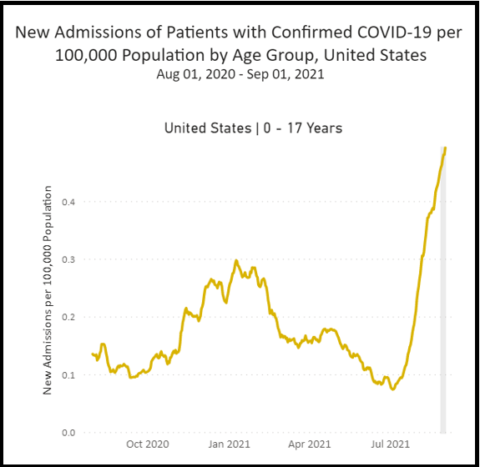
The CDC found that “Weekly COVID-19–associated hospitalization rates among children and adolescents rose nearly five-fold during late June–mid-August 2021”. Currently, an average of 365 children are being hospitalized every day, more than ever before. In Florida alone, an average of 68 children are going to the hospital every day. The American Academy of Pediatrics added 47 new deaths between August 12th and August 26th, 2021. Sadly, multiple adolescents, including some with no underlying health issues, have died of COVID-19 after the vaccine was available to them (here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, and here).
Almost all countries with abundant supply are vaccinating children older than 12-years. Multiple medical organizations, including the American Heart Association and American Academy of Pediatrics agreed and released a statement supporting the vaccine in adolescents. Their statement said:
The facts are clear: this is an extremely rare side effect, and only an exceedingly small number of people will experience it after vaccination. Importantly, for the young people who do, most cases are mild, and individuals recover often on their own or with minimal treatment. In addition, we know that myocarditis and pericarditis are much more common if you get COVID-19, and the risks to the heart from COVID-19 infection can be more severe.
Since then, evidence has emerged that the vaccine works very well for adolescents. According to the CDC, “Hospitalization rates were approximately 10 times higher in unvaccinated compared with fully vaccinated adolescents, indicating that vaccines were highly effective at preventing serious COVID-19 illness in this age group during a period when the Delta variant predominated”. The CDC estimated that the benefits of vaccination for teenagers and young adults are substantial in preventing infection, hospitalizations, and deaths. Assuredly, schools with more vaccinated students will have an easier time staying open.
The bottom line
This infographic shows quite clearly the impact, and benefits, of COVID-19 vaccines in younger people:

In light of this information, Dr. Tom Shimabukuro, the deputy director of CDC’s Immunization Safety Office said, “COVID-19 vaccines continue to undergo the most intensive safety monitoring in U.S. history. Getting vaccinated remains the best way to protect yourself and your loved ones against a virus that has taken millions of lives.” He’s right.
The virus is much more dangerous than the vaccine for adolescents and young adults. Pro-vaccine doctors will share the facts. Anti-vaccine doctors won’t.