
{kind=link}
On June 22nd, 2021 well-known anti-vaxxer Robert F. Kennedy, Jr. published an article titled “Children’s Health Defense and Robert F. Kennedy, Jr. Protest Efforts to Vaccinate Underage Children Without Parental Knowledge or Consent.” It said the following:
- Even as the CDC is discussing the known cardiac risks and heart inflammation affecting children and young adults following COVID-19 vaccination, a concerted effort is underway to coerce this same group to get the vaccine anyway.
- According to the American Academy of Pediatrics, children comprised only 0.00%-0.23% of all COVID-19 deaths, and eight states reported zero child deaths. When children do get the disease, they’ll likely have lifelong immunity.
- The CDC reports that children are less likely to develop severe illness or die from Covid-19 and are more likely to be asymptomatic or show mild systems. And there are lower rates of infection among children compared with adults. CHD demands that CDC provide the reasoning behind these perplexing recommendations. Why would a vaccine be recommended that perhaps carries more risk to children’s health than the actual disease, and which has no long term safety data to support its use?
Robert F. Kennedy, Jr. is a well-known anti-vaccine propagandist and a member of the “Disinformation Dozen“. It’s pretty easy to label just about anything he says as anti-vaccine misinformation. It’s true that only a small percentage of children who contract COVID-19 get gravely ill and that adults are affected much more severely. A child I love recently got COVID-19 at school and brought it home to his little sister. I wasn’t worried about them, and they were barely sick. However, millions of American children have contracted the virus, and rare outcomes can add up. Hundreds of children have died and tens of thousands of children have been hospitalized. As it would undermine his agenda, Mr. Kennedy and other anti-vaccine activists don’t want you to know this. While vaccine-induced myocarditis is real, vaccines cause myocarditis less often than the virus and vaccine myocarditis is generally less severe. The vaccine can prevent devastating outcomes and deaths in adolescents. As is often the case with anti-vaxxers, Mr. Kennedy deceives by omission, leaving out facts that would cast the virus in a negative light or the vaccine in a positive light.
Unfortunately, many doctors with stellar academic credentials who consider themselves pro-vaccine, have similarly opposed vaccinating children using identical talking points as Mr. Kennedy. As with Mr. Kennedy’s article, the totality of how COVID-19 has harmed children is brushed off with meaningless bromides that “the old have a thousand-fold higher mortality risk than the young”. This is true, but utterly irrelevant as to whether or not the vaccine can protect them from a virus with potentially grave consequences.
What then is the fundamental difference between these doctors and Mr. Kennedy, at least as far as children are concerned?
What does it mean to be pro-vaccine?
To me, being pro-vaccine means taking into account all of the relevant data to make a fair, accurate risk-benefit calculation about a vaccine. I clearly believe adolescents should be vaccinated against COVID-19. My case would be strengthened were I to maximize the harms of the virus and minimize the harms of the vaccine. However, the overwhelming majority of kids with COVID-19 will be just fine. Severe outcomes occur at a very low rate for children, thankfully. I’ve said this in every article I’ve written on this topic. Similarly, I’ve written about vaccine myocarditis as fairly as possible and have said every time that it should not be trivialized. Though most vaccines are overwhelming safe and effective, their imperfections cannot be ignored or wished away.
Being pro-vaccine does not mean blindly suggesting all vaccines. I’ll never need to order the Ebola vaccine, for example. Certainly, before the Delta variant arrived – when it seemed that Covid might fade away and vaccine myocarditis was just popping up – it was not entirely unreasonable to question the vaccine’s risk/benefit ratio in healthy, teenage boys. Not every concern about the COVID-19 vaccine in children is necessarily anti-vaccine. The risk/benefit ratio differs depending on whether that child is in Florida or New Zealand and whether the child has previously contracted COVID-19 or not. We need to leave room for people to have good faith disagreements and questions without inappropriately smearing them as “anti-vaxxers”.
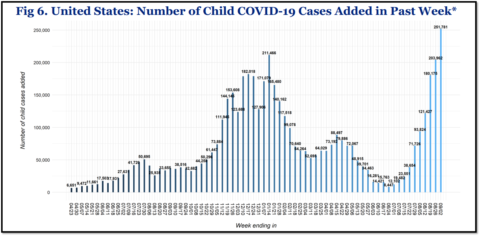
Though it’s fair for people to ask questions about the COVID-19 vaccine, this is true only if they’re genuinely prepared to accept the answers. Right now, the virus is causing more damage to children than ever before in the US, and there have been no catastrophic vaccine outcomes in adolescents. As I have discussed previously, the data clearly shows that the virus is more dangerous than the vaccine for adolescents, especially given that a record number of children – 250,000 – who contracted the virus last week alone in the US. This is a reality that some “pro-vaccine” doctors are determined to ignore, even though they happily commented when pediatric cases were at their low point several months ago.
What does it mean to be anti-vaccine?
Obviously there is no clear-cut criteria for who is anti-vaccine, and there is a very wide spectrum of beliefs in the anti-vaccine movement. Some people proudly announce they are anti-vaxxers, while other notorious spreaders of anti-vaccine misinformation, including Robert F. Kennedy, Jr., adamantly reject this label. To me, the core that unites anti-vaccine thought is: 1) inappropriate minimization of the risk of the virus, and 2) inappropriate minimization of the safety and efficacy of the vaccine
Given the way the virus is harming children at present, arguments against vaccinating them must use one or more of the following techniques: gross errors of fact, blatant omissions of relevant data, or insinuations that negative data can’t be trusted, e.g. “COVID-19 isn’t really that bad for children”. Highly credentialed doctors from prestigious universities have used all of these techniques in some form to bolster their argument that not all children should be vaccinated against COVID-19. All of their errors and omissions downplay the dangers of the virus or the safety/efficacy of the vaccine – never the reverse. These are not just errors then, they are systematic biases. (I discussed this all in detail here.)
Won’t somebody please think of the children who didn’t die of COVID-19?
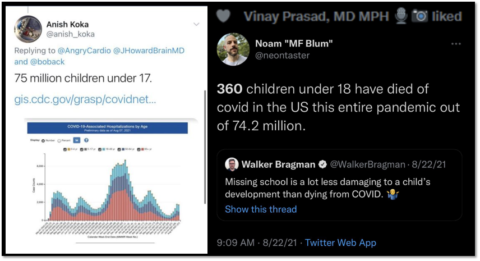
In addition to the errors, omissions, and insinuations, there’s one other technique used to minimize how COVID-19 has harmed children. I’ll call it the “think of all the children who didn’t die” gambit. It’s not wrong. The vast majority of children were not killed by COVID-19. However, this is true of everything that kills children, including cancer, suicide, accidents, and school shootings. If you wouldn’t minimize these tragedies by pointing out that there are 75 million children who didn’t die this way, then you probably shouldn’t do that with COVID-19 either. No child is supposed to die. Hundreds of children are not supposed to die. Imagine if you lost a child and someone responded this way.
The pro-vaccine test
So how can you tell if a doctor is actually pro-vaccine? I propose a simple test. Here are 5 facts about the virus and 5 facts about the vaccine for children and adolescents.
Five facts about the virus
-
- COVID-19 can kill children: Between 486-521 children (depending on which CDC website one uses) have died from the virus in America, including adolescents and children and with no underlying conditions who were eligible to be vaccinated. Sadly, more children are dying now than ever before. Since the start of July, The American Academy of Pediatrics added over 100 deaths to their tally. A newborn just died in Florida.
- COVID-19 has hospitalized many children: Tens of thousands of children have been hospitalized due to COVID-19. More children are being infected than ever before, and therefore more children are being hospitalized now than ever before. Currently, 367 children are being hospitalized every day with COVID-19. This number has been going straight up for awhile now, and I fear it will be awhile before it starts to come down again. Though most children stay just a few days, up to 33% of these need ICU-level care and 6-10% need intubation. According to the CDC, “During March 1, 2020–August 14, 2021, the cumulative incidence of COVID-19–associated hospitalizations was 49.7 per 100,000 children and adolescents”. 1 in 2,000 children in the US have been hospitalized over the course of this pandemic, and cases are higher now for children than ever before.
- Long-COVID may not be rare: There are more questions than answers about long COVID-19 in children, but one recent study from England found that infected children were twice as likely than uninfected children to report multiple symptoms such as headache and “unusual tiredness” 15 weeks later. Other studies found a lower rate, perhaps 2%, but this adds up to a large number of very sick children when multiplied by the millions of children who contracted the virus. This is a new virus and we have to be humble about its potential long-term side effects. Even the majority of children who turn out just fine were often very sick and uncomfortable for several days at a minimum.
- COVID-19 causes myocarditis: A CDC study found that 1 in 754 children with COVID-19 younger than 16 years developed myocarditis, while the rate for their uninfected peers was 1 in 28,000. The risk of myocarditis for children under 16 years was 37 times higher for children infected with COVID-19
- COVID-19-related myocarditis can be severe: Multisystem inflammatory syndrome in children (MIS-C) can cause severe myocarditis , and there have been at least 4,661 cases in the US, possibly many more. Studies have reported coronary artery aneurysms and acute heart failure in children with MIS-C. Other common cardiac complications of myocarditis due to MIS-C include “shock, cardiac arrhythmias, pericardial effusion, and coronary artery dilatation”. Cardiac arrhythmias have led “to hemodynamic collapse and need for ECMO support” in some children
Five facts about the vaccine
- Vaccine myocarditis is less severe: Vaccine myocarditis is much less severe than viral myocarditis. Short-term outcomes in vaccine myocarditis from multiple case series and government agencies in different countries have been consistently favorable. Most individuals are hospitalized, but almost all leave the hospital in just a few days after receiving simple treatments. No child has needed to be intubated as far as I know. About 75% are symptom-free after follow-up. Nonetheless, long-term monitoring is needed, and the condition should not be trivialized.
- Vaccine myocarditis is not common: The exact rate of vaccine myocarditis is not clear. It is not rare, but it is not common either. Israel initially reported a rate of 1:3,000-6,000 young men. Since that time, two vaccine safety databases maintained by the CDC (here and here) report a give a rate of about 1:13,500 for teenage men after their second shot. Data from Ontario showed a rate of 1 in 11,000 for males age 12-17 after their second dose. Another large study of people age 12-39 years using safety surveillance data from Vaccine Safety Datalink put the rate at much less than this, about 1 in 79,000. No pediatric hospital has been deluged by children suffering from vaccine-myocarditis. The same cannot be said for the virus.
- The Vaccine worked in trials: The vaccine successfully prevented adolescents from getting COVID-19 in clinical trials (Pfizer, Moderna). In these trials, a total of 20 COVID-19 cases were observed, none in vaccinated adolescents.
- The vaccine is working in the real world: A recent study by the CDC found that unvaccinated children are hospitalized 10 times more often than vaccinated ones. Most countries with abundant supply are vaccinating adolescents.
- No vaccine deaths: According to the CDC, nearly 9 million American adolescents have been vaccinated, and none are known to have died from the vaccine.
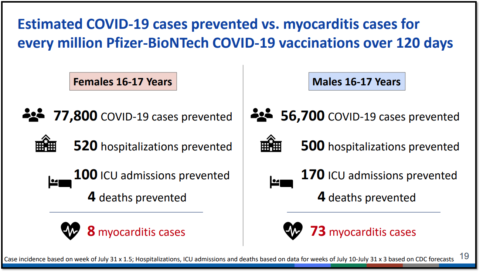
The CDC summarized the risks and benefits of the COVID-19 for 16 and 17-year-olds as follows.
Pro-vaccine doctors shouldn’t just be willing to share some at least version of these facts, they should do so eagerly whenever they discuss the topic. Many parents and young people remain ignorant of this information. Only 32% of adolescents are fully vaccinated in the US. The consequences have been severe for some of them. Some children would likely still be alive right now if these facts were more widely known. One father, whose 15-year-old died said:
It’s something that’s going to be stuck with me for my whole life, thinking maybe I should have done that sooner. Maybe I could’ve done something to help prevent this. I don’t want any other parent to go through what I did — seeing my daughter perfectly healthy one day then following a week and a half, she’s gone.
More preventable tragedies await. I feel it’s important to actually read about some of these children occasionally to remind yourself they are more than just statistics on a CDC website. These are young people robbed of their entire life. Yet, astonishingly, several doctors have written multiple articles or produced long Twitter threads on the topic of COVID-19 vaccines for children without acknowledging these basic facts. For some, these facts are just unmentionable.
Passing the pro-vaccine test should be extremely easy. It only requires someone to acknowledge and share basic facts when opining on children and the vaccine. As a bonus, sharing these facts will help prevent significant suffering for a significant number of children. I mean honestly, this is an extremely low bar. Yet, I know several doctors who will fail the pro-vaccine test. Even as they extol the virtues of honestly discussing the risks and the benefits of the vaccine, they will refuse to share these core facts.
By what measure can they be considered pro-vaccine?