{kind=link}

A chiropractor doing spinal manipulation.
While generic spinal manipulation is an acceptable physical medicine modality, spinal manipulation based on chiropractic vertebral subluxation theory is scientifically unacceptable. Since a significant number of chiropractors base their practice on subluxation theory which supports use of spinal manipulation as a primary treatment for a broad scope of health problems, it continues to be necessary to inform the public about the controversial aspects of chiropractic care and the role of spinal manipulation as a form of manual therapy.
This updated fully-referenced review of chiropractic past and present will be helpful in connecting the dots for persons who have questions about chiropractic or who might be concerned about the practice of chiropractic as an alternative healing method. This review also offers useful tips and warnings dealing with spinal manipulative treatment for neck and back pain, including specific reasons why infants and small children should never be subjected to spinal manipulation, especially “spinal adjustments” provided by subluxation-based chiropractors.
Chiropractic subluxation theory: still no evidence
The vertebral subluxation theory that gave birth to the chiropractic profession in 1895 proposed that 95 per cent of diseases are caused by displaced vertebrae that place pressure on spinal nerves. Today, chiropractic is defined as a method of removing nerve interference to restore and maintain health by adjusting a “vertebral subluxation complex,” which has been described as “changes in nerve, muscle, connective, and vascular tissues which are understood to accompany the kinesiologic aberrations of spinal articulations”.
There is no credible evidence to support the theory that a vertebral subluxation can affect general health or cause internal organs to become diseased. Spinal nerves are commonly compressed by osteophyte formation or by a herniated disc. Even the most severe compression of a spinal nerve, which may cripple the supplied musculoskeletal structures, does not cause organic disease. In the absence of fracture or pathology, vertebral misalignments rarely affect spinal nerves.
Organs are not supplied by spinal nerves
Spinal nerves supply the sensory and motor (voluntary) functions of musculoskeletal structures. Involuntary function of the body’s organs is regulated by autonomic nerve ganglia and plexuses located outside the spinal column and by autonomic cranial and sacral parasympathetic nerves that pass through solid bony openings (where subluxations do not occur). The all-important vagus nerves (cranial nerves that originate in the brain stem) pass through openings in the base of the skull and travel down through the neck, thorax, and abdomen to supply organs along their path. Preganglionic autonomic (sympathetic) fibers, which emerge from the spinal cord and pass through spinal segments from the first thoracic vertebra to the second lumbar vertebra, terminate in sympathetic trunk and splanchnic ganglia located outside the spinal column.
The vagus nerves along with autonomic ganglia and nerve plexuses provide overlapping sympathetic and parasympathetic nerve supply from many directions and sources (in concert with chemical, hormonal, and circulatory factors) to assure continued function of the body’s organs, independent of spinal nerves. This is why severance of the spinal cord in the neck area, shutting off brain impulses to spinal nerves, can cause paralysis of muscles from the neck down while the body’s organs continue to function. (A serious transverse spinal cord lesion above C5 in the upper neck can cause respiratory paralysis and often death.) Transplanted organs, relying upon hormones supplied by blood flow, can function without reconnection of severed nerves.
Since the spinal cord ends at the level of the 2nd lumbar vertebra, spinal nerves travel down from the spinal cord (like the hair on a horse’s tail) to pass out through openings (foramina) between the lumbar vertebrae and through solid bony openings in the sacrum to supply bladder and bowel sphincter muscles. Except in severe cases of lower lumbar spondylolisthesis (sliding forward of a vertebra as a result of a fracture or a congenital defect in the bony bridges that connect the vertebra with the spinal joints), sacral spinal nerves are not affected by vertebral misalignment but can be compressed by protrusion of a lower lumbar disc into the spinal canal, affecting voluntary control of sphincter muscles (cauda equina syndrome), a medical emergency requiring the attention of a neurosurgeon.
The effect of spinal manipulation on joint mechanoreceptors and nociceptors might temporarily relieve back pain, and mobility might be improved by releasing adhesions and stretching connective tissues. But there is no evidence to indicate that such effects have a significant effect on the body’s organs.
A chiropractic vertebral subluxation or “joint dysfunction” alleged to cause disease by interfering with nerve supply to organs has never been proven to exist and cannot be equated with an orthopedic subluxation, a partial dislocation that causes musculoskeletal symptoms.
Tenuous subluxation theory
Generic spinal manipulation designed to relieve pain and restore mobility is not the same as a chiropractic adjustment that is claimed to improve health. While some chiropractors use spinal manipulation appropriately in a practice limited to treatment of musculoskeletal problems, many “adjust” the spine to correct “subluxations” in an attempt to restore and maintain health by removing “nerve interference.” The theory underlying such treatment is so tenuous that it cannot be explained or tested, resulting in a number of vague and implausible definitions that are supported only by placebo effects and anecdotal case reports.

The first clue I had that the chiropractic vertebral subluxation theory was not a valid construct was provided in the anatomy and physiology textbooks I used during my course of study at Lincoln Chiropractic College.
Resting on the principles of its founding father, chiropractic in the United States continues to be defined as a method of correcting vertebral subluxations to restore and maintain health. A 2015 publication of the National Board of Chiropractic Examiners (NBCE), Practice Analysis of Chiropractic 2015, states that “The specific focus of chiropractic practice is known as the chiropractic subluxation or joint dysfunction. A subluxation is a health concern that manifests in the skeletal joints, and, through complex anatomical and physiologic relationships, affects the nervous system and may lead to reduced function, disability, or illness”. This definition of chiropractic is in keeping with a paradigm formulated by the Association of Chiropractic Colleges (ACC) in 1996, signed by 16 North American chiropractic college presidents:
Chiropractic is concerned with the preservation and restoration of health, and focuses particular attention on the subluxation…a complex of functional and/or structural and/or pathological articular changes that compromise neural integrity and may influence organ system function and general health.
A new definition of the chiropractic subluxation, formulated by The Rubicon Group, an international consortium of seven chiropractic colleges which includes three subluxation-based chiropractic colleges in the United States (Life Chiropractic College West, Life University, and Sherman College of Chiropractic), describes a “neurologically-centered model of subluxation”:
We currently define a chiropractic subluxation as a self-perpetuating, central segmental motor control problem that involves a joint, such as a vertebral motion segment, that is not moving appropriately, resulting in ongoing maladaptive neural plastic changes that interfere with the central nervous system’s ability to self-regulate, self-organize, adapt, repair and heal.
The International Federation of Chiropractors and Organizations (IFCO), disagreeing with the Rubicon definition of a chiropractic subluxation, responded with this statement:
The IFCO asserts strongly that any attempt to define chiropractic subluxation without emphasizing the importance of vertebral subluxation is a diminution of the profession.
The IFCO offered this definition of a chiropractic subluxation:
A vertebral subluxation is an alteration of the intervertebral relationships of one or more articulations of the spinal column or the immediate weight bearing components of the axial skeleton; accompanied by a change in the morphology of the tissue occupying the neural canal and/or intervertebral foramina; as well as an alteration of neural function sufficient to interfere with the transmission of organizing information, considered to be homologous to the mental impulse.
A 2015 Position Statement on Clinical and Professional Chiropractic Education, representing seven European chiropractic colleges, does not support chiropractic subluxation theory:
The teaching of vertebral subluxation complex as a vitalistic construct that claims that it is the cause of disease is unsupported by evidence. Its inclusion in a modern chiropractic curriculum in anything other than an historical context is therefore inappropriate and unnecessary.
Despite the obvious implausibility of chiropractic subluxation theory, explained in the scientifically incomprehensible language of pseudoscience, studies done by chiropractors rarely dispute the basic tenets of subluxation theory. One exceptional landmark study by a team of academic chiropractors, however, concluded that:
No supportive evidence is found for the chiropractic subluxation being associated with any disease process or of creating suboptimal health conditions requiring intervention.
But belief in subluxation theory persists. An independent study by chiropractic researchers revealed that:
Despite the controversies and paucity of evidence the term subluxation is still found often within the chiropractic curricula of most North American chiropractic programs
A survey of North American chiropractic students published in 2015 reported that a majority “would like to see an emphasis on correction of vertebral subluxations”.
The American Chiropractic Association (ACA), the leading association representing chiropractors, says that:
Chiropractic is a health care profession that focuses on disorders of the musculoskeletal system and the nervous system, and the effects of these disorders on general health.
With no mention of the word “subluxation,” the ACA advises prospective patients that “Doctors of Chiropractic (DCs) care for patients of all ages, with a variety of health conditions”. Embracing a broad scope of practice based on the effect of musculoskeletal problems on the nervous system (a position that leaves the door open for advocates of subluxation theory), it appears that the ACA might be refraining from renouncing subluxation theory in order to preserve its membership – a dilemma that compromises the association’s credibility in representing chiropractic as a science-based profession.
The International Chiropractic Association (ICA), the smaller of the two American chiropractic associations, clearly defends subluxation theory:
The basic premise of chiropractic science is that abnormalities and misalignments of the spine, defined as subluxations(s) in chiropractic science, can and do disrupt the normal function of the nervous system and may create negative health consequences. The correction and/or reduction of subluxation(s) through the adjustment of spinal structures can remove nervous system interference and restore the optimal function of the body.
Subluxation deniers vs. subluxation believers
Controversy surrounding the validity of subluxation theory has divided chiropractors into camps of “subluxation deniers” and “subluxation believers.” Chiropractors often deny that subluxation believers are in the majority, even though state laws and the National Board of Chiropractic Examiners in the United States define chiropractic as a profession “focused on the chiropractic subluxation”. It certainly appears that subluxation deniers in the chiropractic profession may be in the minority, making it difficult to find a chiropractor who does not subscribe to subluxation theory or who does not offer spinal manipulation as a treatment for anything other than a musculoskeletal problem.
Making an effort to separate themselves from the stigma associated with chiropractic subluxation theory, some subluxation believers no longer use the “subluxation” word, instead substituting vague descriptions of a spinal problem, such as a “joint dysfunction” or a “neuro-biomechanical lesion.” Some of these descriptions do not involve displacement of a vertebra, but all are alleged to have an adverse effect on the nervous system and general health. You cannot rely upon the care of a chiropractor who claims to have abandoned the vertebral subluxation theory but who continues to manipulate the spine in an attempt to restore and maintain health by removing nerve interference – care that is no different from that of a subluxation believer.
Consumers should be wary of the rhetoric of chiropractors who say “I do not treat disease. I simply remove nerve interference so that the body can heal itself.” Such chiropractors assume that for every disease there is a corresponding vertebral subluxation, requiring life-long treatment to correct or prevent subluxations.
Spinal manipulation as a treatment option for back pain

Although there is considerable literature dealing with the use of spinal manipulation as a treatment for neck and back pain, there are few reliable studies providing adequate proof supporting such treatment. A 2015 Cochrane review, for example, dealing with manipulation for neck pain, reported that “No high-quality evidence was found, so uncertainty about the effectiveness of mobilization or manipulation for neck pain remains”.
Low-back pain is most often the subject of credible reviews and studies that examine the effects of spinal manipulation, a treatment now being provided by physical therapists, osteopaths, physiatrists, orthopedists, and chiropractors. Scientifically-oriented reviews dealing with use of generic spinal manipulation as a treatment for back pain, however, do not offer strong support for such treatment:
- A 2011 Cochrane Systematic Review of spinal manipulative therapy for chronic low-back pain reported that “High-quality evidence suggests that there is no clinically relevant difference between SMT [spinal manipulative therapy] and other interventions for reducing pain and improving function in patients with chronic back pain”.
- A 2013 Cochrane review of spinal manipulative therapy for acute low-back pain concluded that “SMT is no more effective for acute low back pain than inert interventions, sham SMT or as an adjunct therapy. SMT also seems to be no better than other recommended therapies. Our evaluation is limited by the few numbers of studies; therefore, future research is likely to have an important impact on these estimates.”
- A 2012 National Center for Complementary and Alternative Medicine review of back-pain studies reported that “Overall, studies have shown that spinal manipulation is one of several options─including exercise, massage, and physical therapy─that can provide mild-to-moderate relief from low-back pain. Spinal manipulation also appears to work as well as conventional treatments such as applying heat, using a firm mattress, and taking pain-relieving medications.”
- A systematic review and meta-analysis of the use of spinal manipulative therapy in the treatment of acute low-back pain published in The Journal of the American Medical Association in 2017 concluded that such treatment resulted in “modest improvements in pain and function at up to 6 weeks.
Some chiropractic colleges offer decent instruction in the care of musculoskeletal problems, including skillful use of spinal manipulation as a treatment for back pain. But such treatment is tainted by subluxation theory that encompasses a broad scope of ailments. For this reason, physicians who refer back-pain patients to chiropractors for spinal manipulative therapy must be cautious in selection of a chiropractor, and they must take responsibility for the diagnosis, lest inappropriate treatment makes them vulnerable to liability for damages. Care must also be taken to make it clear that referral to a selected chiropractor who uses manipulation appropriately is not an endorsement of chiropractic subluxation theory.
Unfortunately, manipulative techniques used by chiropractors may vary from one practitioner to another. While some chiropractors may use generic spinal manipulation in an appropriate manner, many of their colleagues use subluxation-based proprietary manipulative techniques that have no known value and no reciprocal compatibility in working with other health-care professionals. The techniques and goals of mobilization or generic spinal manipulation, however, when properly performed and based on the science of anatomy, are always basically the same, no matter who the provider might be.
Although evidence supporting use of spinal manipulation as a treatment for back pain may be weak, and the benefits of such treatment modest or temporary, it is important to understand that while chiropractic manipulation based on subluxation theory has been rejected by the scientific community, generic spinal manipulation is a plausible and acceptable treatment option that can be beneficial in the care of carefully selected mechanical-type back problems.
Manipulation/mobilization/adjustment
Mobilization of joints has been traditionally identified as a physical therapy procedure. Most physical therapists who use manual therapy use manipulation as well as mobilization. Chiropractors, on the other hand, are identified primarily by their use of a “spinal adjustment,” a procedure that is used for a reason that differs from the principles supporting use of standard manipulation or mobilization.
On the physical therapy side, mobilization and manipulation are used to improve range of motion in any joint that does not function normally. Grade I through Grade IV mobilization, for example, moves joints through normal ranges of movement, while Grade V mobilization (thrust-type manipulation) forces movement of joints beyond their normal end-range of motion. A chiropractic adjustment based on subluxation theory is a thrust-type manipulation directed at a specific vertebra to remove “nerve interference.”
Manipulation that forces slight separation of joint surfaces can produce cavitation (popping sounds). Although cavitation or “gapping” of joints during spinal manipulation may temporarily increase range of movement or signal release of joint adhesions, the sound associated with such treatment (which can occur in normal joints) is generally not considered to be significant. In the case of a chiropractic adjustment, however, in which the stated goal is to correct a subluxation causing nerve interference, the popping sound can have a powerful placebo effect. Taking advantage of the power of suggestion, some chiropractors lead their patients to believe that the popping sound heard during a spinal adjustment means that vertebral subluxations are always present, requiring regular adjustments to keep selected vertebrae properly aligned. The nocebo effect (fear of illness) that occurs as a result of not getting regular adjustments further perpetuates unnecessary treatment.
Spinal manipulation as a treatment for neck and back problems has been used for thousands of years. A specific chiropractic adjustment, a thrust-type manipulation directed at selected vertebrae in an effort to restore and maintain health by removing nerve interference, is a fairly recent development, invented by D.D. Palmer in 1895. Subluxation-based chiropractors are quick to explain that long-lever spinal manipulation or mobilization is not the same as a specific short-lever chiropractic adjustment applied to a vertebral subluxation, thus clinging to a belief system that continues to define the practice of chiropractic.
A physical therapist who uses mobilization or manipulation (Grade V mobilization) to relieve pain and restore mobility in a compromised area of the spine is more likely to use manipulation appropriately than a subluxation-based chiropractor who uses “specific adjustments” up and down the spine to correct asymptomatic “subluxations” or to remove “nerve interference.”
Complementary vs. alternative
In observing the web sites and promotional materials of newly graduated chiropractors, it appears that many of these chiropractors are combining science-friendly treatment methods with the pseudoscience of subluxation theory in order to “remove nerve interference and improve health.” Some are claiming to be primary care providers, combining “spine care” with “health-and-wellness care” in a holistic approach that entails treatment and prevention of the gamut of human ailments, often including “functional medicine” and other questionable healing methods under the banner of “alternative medicine” or “integrative medicine.”
Although the public generally thinks of chiropractors as back specialists, few chiropractors limit their care to treatment of back pain. According to the Association of Chiropractic Colleges, “chiropractic is associated with the field of complementary and alternative medicine as a method of improving and preserving health.” Apparently, the chiropractic profession at its core has chosen the complementary and alternative medicine (CAM) route rather than seeking to develop as a scientifically acceptable back-care musculoskeletal specialty, despite the fact that back pain and musculoskeletal conditions are the No. 1 and No. 2 causes of disability worldwide.
Substituting an unproven spinal adjustment for a variety of proven or reasonably effective treatment methods for a variety of health problems places subluxation-based chiropractic care squarely in the camp of alternative medicine where bogus and unproven treatment methods gather for undeserved recognition.
It is important not to confuse a nonsensical unproven alternative treatment method (such as homeopathy or subluxation-based chiropractic) with scientifically acceptable massage or generic spinal manipulation that can be described as a primary or complementary form of treatment for some musculoskeletal problems. As said by Marcia Angell and Jerome Kassirer in 1998:
It is time for the scientific community to stop giving alternative medicine a free ride….There cannot be two kinds of medicine─conventional and alternative. There is only medicine that has been adequately tested and medicine that has not, medicine that works and medicine that may or may not work. Once a treatment has been tested rigorously, it no longer matters whether it was considered alternative at the outset. If it is found to be reasonably safe and effective, it will be accepted.
Back care vs. spine care

Generic spinal manipulation can sometimes be helpful in treating mechanical-type low-back pain.
While a good chiropractor can offer a service of value in conservative care for uncomplicated mechanical-type back pain, a chiropractor is not a “spine specialist” capable of providing care for complicated conditions affecting the spine. Isolated from the mainstream of healthcare, solo chiropractors do not have access to the multiple medical facilities and the pharmaceuticals needed to diagnose and treat spinal problems involving severe injury, disease, infection, or pain of unknown origin – a service now being provided by some orthopedic surgeons who identify themselves as a spine specialist.
I have always believed that the chiropractic profession would be more acceptable socially and scientifically as a conservative back-care specialty or as a subspecialty of medicine – contingent, of course, upon changes in state laws and the curriculum of chiropractic colleges. Low back pain, the fifth most common reason for all physician visits in the United States, is difficult to diagnose and treat – a time-consuming responsibility that few physicians are qualified to handle or willing to accept and who would probably welcome a back-care specialty.
Physical therapy offers care and rehabilitation for a broad scope of neuromusculoskeletal problems – care that includes use of manual therapy. But there is not yet a certified physical-medicine specialty or subspecialty limited to conservative care for neck and back pain.
The path of chiropractic
At the present time, there are no indications that chiropractic colleges in the United States will seek specialization in conservative care for back problems, retreating from the definition of chiropractic as a form of alternative medicine. The National University of Health Sciences, for example, formerly the National College of Chiropractic (a leading chiropractic college), offers programs in naturopathic medicine, acupuncture, and oriental medicine as well as a degree in chiropractic medicine. Such dubious alternative healing methods are gaining acceptance as a form of “integrative medicine,” a designation that bends the rules of science in order to meet public demand for questionable care that can be financially lucrative when combined with conventional care.
There is no reason to believe that the subluxation theory will ever be discarded by all chiropractors. Adjustment of chiropractic vertebral subluxations, a belief system perpetuated by pseudoscience and monetary returns, will continue to be guided by whimsical thinking and misinformation. Chiropractic subluxations that are not detectable by conventional diagnostic procedures, for example, are allegedly being located by such dubious procedures as thermography, surface electromyography, applied kinesiology, and leg-length checks. Dozens of different antithetical manipulative techniques are used to correct such subluxations.
A 1995 publication endorsed by the Association for the History of Chiropractic listed 97 “named chiropractic techniques” used by chiropractors, most of which are too implausible to warrant consideration. For example, some chiropractors use a spring-loaded stylus in an attempt to tap vertebrae into alignment in order to “help the body heal itself”. A few use “reflex” techniques to realign vertebrae without manipulating the spine. Upper cervical chiropractors believe that aligning the atlas (the vertebra at the top of the spine) will “influence the central nervous system and brain stem function” as well as realign vertebrae from the neck down. And so on.
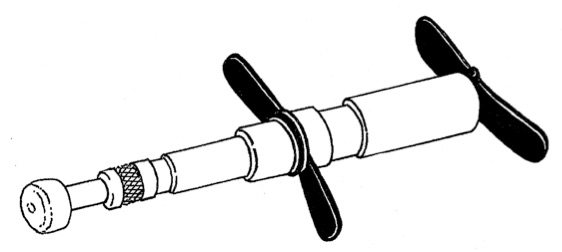
An adjusting instrument used by some chiropractors to tap alleged vertebral subluxations into alignment.
While the chiropractic profession continues to be mired in the pseudoscience of vertebral subluxation theory, use of spinal manipulation is gaining greater acceptance as a physical treatment option in the armamentarium of physical medicine, providing competition for chiropractic treatment of back pain. On a path of no return as a form of alternative medicine competing with conventional medical care, the chiropractic profession is becoming increasingly dependent upon its spinal nerve-interference theory to justify its existence and its independence as a healing art.
Red flags and back-pain symptoms that warn against use of spinal manipulation
The next time you have back pain and you want to try using spinal manipulation to relieve your symptoms, there are some red flags you should know about in order to avoid inappropriate use of such treatment, no matter who does it. You cannot always depend upon a chiropractor or a manual therapist to inquire about subjective symptoms that might be helpful in planning treatment. It is always a good idea to be as well informed as possible when submitting to any form of treatment, especially spinal manipulation or a spinal adjustment that might be potentially harmful.
It goes without saying that spinal manipulation for acute back pain should not be done immediately following injury or without a definitive diagnosis.
- If you are on a treatment program requiring prolonged ingestion of a corticosteroid or a thyroid hormone, especially if you are past middle age, sudden appearance of back pain that restricts movement might be an indication that an osteoporotic vertebra has collapsed. Manipulation should not be considered.
- If you have a history of lung, breast, or prostate cancer and you develop a gradual onset of back pain, or if you have persistent back pain for no apparent reason, you should be tested for bone disease. Some forms of malignancy commonly metastasize to the ribs or the vertebrae, making them vulnerable to fracture during manipulation.
- Backaches can be caused by a kidney infection that may go undetected until an elevation in temperature is discovered. Always take your temperature when you have a backache. If you have a fever, you should always see your family physician, regardless of what you think might be causing your backache.
- Mechanical-type back pain that originates in musculoskeletal structures is relieved by rest and aggravated by movement. Back pain that has an internal origin is unaffected by movement. If you develop constant back pain that is not affected by movement of your body, you should see your family physician to rule out such things as organic disease, infection, or an aortic aneurysm.
- Persistent backache that defies diagnosis should undergo testing and observation in a search for such elusive diseases as ankylosing spondylitis or rheumatoid arthritis, which could be aggravated by manipulation.
- Kidney stones can cause acute back pain. Unlike mechanical-type back pain that restricts movement, the referred pain of a kidney stone produces pain that will not allow you to rest or sit still. If you have the misfortune of experiencing back pain that causes you to squirm about or roll around on the floor, you should go to a hospital emergency room as soon as possible.
- Pain, numbness, and other symptoms radiating down one or both legs, or weakness in one leg or foot may be an indication of encroachment upon spinal nerves in the lower portion of the spine. Such symptoms can be caused by disk herniation, osteophyte formation, or some other pathological process. When a spinal disc is herniated or when a spinal nerve is pinched, spinal manipulation is not indicated. (A pinched spinal nerve in the thoracic area of the spine can refer pain into musculoskeletal structures in thoracic and abdominal areas, often mimicking angina or an organic disease. Pain anywhere in the torso should be brought to the attention of a physician.)
- Loss of bladder or bowel control with numbness in the perineal (saddle area) of your pelvis is a medical emergency (cauda equina syndrome) requiring the immediate attention of a neurosurgeon. Such symptoms can be caused by a lumbar disk protrusion that has entered the spinal canal.
The clear and hidden dangers of neck manipulation
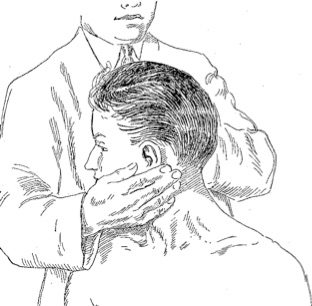 Numerous reports have associated upper cervical manipulative therapy with stroke involving injury to vertebral or internal carotid arteries. Such strokes have occurred in young, healthy persons, some of which have been confirmed by imaging studies that show dissection of healthy vertebral arteries due to trauma. Although strokes believed to be caused by neck manipulation are rare, there is good reason to warn against use of neck manipulation that involves rotation of head and upper cervical (occiput-atlas and atlanto-axial) structures beyond normal ranges of movement.
Numerous reports have associated upper cervical manipulative therapy with stroke involving injury to vertebral or internal carotid arteries. Such strokes have occurred in young, healthy persons, some of which have been confirmed by imaging studies that show dissection of healthy vertebral arteries due to trauma. Although strokes believed to be caused by neck manipulation are rare, there is good reason to warn against use of neck manipulation that involves rotation of head and upper cervical (occiput-atlas and atlanto-axial) structures beyond normal ranges of movement.
The vertebral arteries in particular are vulnerable to injury when mobilization and manipulation techniques involve a rotatory component greater than 45 degrees at the atlanto-axial level. Risk always outweighs benefit when neck manipulation of any kind is used to correct alleged chiropractic subluxations.
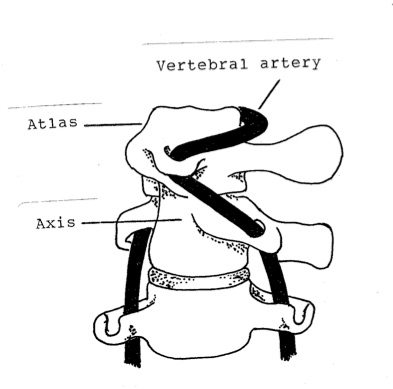
Forced passive rotation of the atlas on the axis past 45 or 50 degrees stretches the vertebral artery. Normally, during active cervical rotation, all of the cervical vertebrae move together, a little movement in each joint, allowing about 80 degrees of rotation right and left. The atlantoaxial joint, where there is no intervertebral disc, is capable of about 50 degrees of independent rotation right and left, allowing excessive rotation during upper cervical rotatory manipulative techniques.
The normal anatomical configuration of the top two cervical vertebrae that provide a bony pathway for the vertebral arteries places these arteries at risk when there is extreme head or upper neck rotation. In addition to possible disease or malformation in the network of vertebrobasilar and internal carotid arteries in the base of the skull, there are some rare, often undetected, structural abnormalities that threaten the vertebral arteries when the head and neck are rotated.
Obvious contraindications for cervical spine manipulation include atlas instability in rheumatoid arthritis, nerve root impingement or disc herniation, osteoporosis, use of blood thinners, carotid bruits, atherosclerosis, symptoms of vascular insufficiency (such as fainting) on active and passive head rotation within a normal range of movement, the short neck of basilar invagination (congenital migration of the upper cervical spine into the base of the skull), and so on.
Often undetected structural contraindications for upper neck manipulation include these cervical spine abnormalities:
- A retrolenticular vertebral artery ring, an abnormal bony bridge that encompasses the vertebral artery where it passes over the posterior arch of the atlas, can severely compress a vertebral artery during rotatory upper cervical manipulation.
- Chiari malformation, a structural defect that allows a portion of the cerebellum to pass down through the foramen magnum and enter the spinal canal, can cause headache that begins on the back of the head and neck, resembling a cervicogenic headache or a muscle-contraction headache. Upper cervical manipulation in such a case would be dangerous.
- Bow hunter’s syndrome, a rare vertebral artery insufficiency caused by an abnormal fibrous band or an osseous prominence that compresses the vertebral artery at the atlantoaxial level during active or passive head rotation in a certain direction, often within a normal range of movement. Such symptoms detected during range of motion testing in the cervical spine are an obvious contraindication for cervical spine manipulation. Any symptom of circulatory insufficiency, such as dizziness or drop attack, caused by rotation of the head or by extension of the cervical spine warns against use of cervical spine manipulation or any form of manual therapy applied to the neck.
- Os odontoideum is a congenital absence or lack of fusion of the odontoid process, a dowel-like projection of bone from the axis that serves as a pivoting point for rotation of the atlas. Since there is no intervertebral disc between the atlas and the axis, a defective odontoid process would allow dislocation of the atlas when the upper cervical spine is forcefully manipulated, with or without rotation.
Bottom line: There is no credible evidence to support use of spinal manipulation for anything other than uncomplicated mechanical-type neck or back pain and related neuromusculoskeletal problems. Upper neck manipulation, however, is so risky (with little evidence of benefit) that I usually advise against submitting to such treatment.
If you are looking for a chiropractor who treats back pain, look for one who does not subscribe to subluxation theory and who limits care to musculoskeletal problems – one who is willing to exchange office notes with your family physician. Remember that most of the time, acute low-back pain is a self-limiting condition that will resolve in four to six weeks, with or without treatment. Appropriate manipulative treatment may, however, relieve symptoms and reduce need for medication.
If acute back pain grows progressively worse or persists unrelieved for longer than a week, or if there is no measured improvement after two to four weeks, manipulation should be discontinued. Uncomplicated back pain that lasts longer than three months may be classified as chronic, requiring use of self-help measures (such as exercise and postural ergonomics) and occasional treatment for symptomatic relief as needed.
Chiropractic and children

According to the International Chiropractic Association’s Council on Chiropractic Pediatrics, “Chiropractic care can never start too early.” Patient education provided by the council advises that:
A 1992 survey showed that the most common conditions for which children visit a chiropractor are: earaches, neck pain, check-up, headache, upper respiratory, low back pain, allergies, asthma, enuresis, and thoracic pain. Other reasons are ADD and ADHD, colic, torticollis, insomnia, growing pains, and persistent crying in infants.
I do not know of any medically acceptable diagnosis that would warrant manipulating the spine of a pre-adolescent child. The cartilaginous, immature spine of an infant or a small child should never be manipulated, as some chiropractors are doing to correct alleged “subluxations”.
When British author Simon Singh stated in an April 19, 2008, issue of the Guardian that the British Chiropractic Association’s (BCA) claims that chiropractors can help treat children with “colic, sleeping and feeding problems, frequent ear infections, asthma and prolonged crying” were bogus, he was sued for libel by the BCA. The BCA was unable to present adequate scientific evidence to support chiropractic treatment for children. The suit was withdrawn in 2010 when the court ruled that Singh’s comments were legally permissible as “fair comment”.
There has also been some speculation that manipulating the spine of a child younger than 6 to 8 years of age might fracture or damage cartilaginous epiphyseal growth centers, an occult injury that could result in development of pre-adolescent spinal deformity such as scoliosis or Scheuermann’s kyphosis.
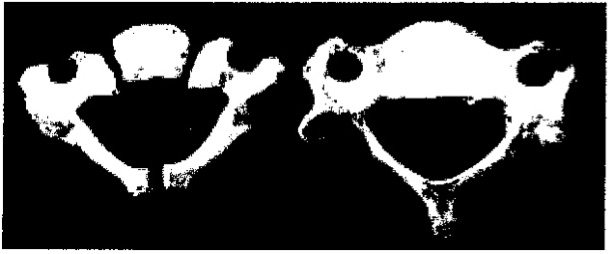
Ossification centers in the thoracic vertebra of a child age 1 and age 6.
In general, “Potential complications and unknown benefits indicate that SMT should not be used in the pediatric population.”
The above statement was made by a neurosurgeon. I have not seen any credible medical publications that recommend use of spinal manipulation for children. When the U.S. Department of Health and Human Services published Acute Low Back Problems in Adults [PDF], suggesting that spinal manipulation might be helpful for patients with acute low back problems without radiculopathy, it excluded children younger than 18 years of age, “since diagnostic and treatment considerations for this group are often different than for adults.”