{kind=link}
Yes, there are antivaccinationists who actually believe this.
As hard as it is to believe after seven and a half years of existence and nearly 2,400 posts on SBM, every so often, something reminds me that we here at SBM haven’t discussed a topic that should be discussed. So it was a couple of weeks ago, when I saw a familiar name in a news story that wasn’t about vaccines. You might recall a news story last month when a shadowy group with ties to radical antiabortion groups, the Center for Medical Progress, led by a man named David Daleiden, ran a highly questionable “sting” operation (complete with fake IDs) to “prove” that Planned Parenthood was selling aborted fetuses for medical research.
While reading news stories about Daleiden and CMP, I came across a familiar name, a name that many of us who discuss antivaccine misinformation are familiar with. I’m referring to Theresa Deisher, founder of the Sound Choice Pharmaceutical Institute. It turns out that Deisher helped to prepare Daleiden for his role as a biomedical representative that he assumed in order to deceive representatives of Planned Parenthood. She taught him how to talk the talk and walk the walk, so to speak, so that he was convincing as a representative of a biomedical research firm.
I can hear you asking: So what? What do Daleiden and CMP have to do with vaccines? It’s not CMP per se, but Deisher who is relevant. The reason that Deisher is so relevant to Science-Based Medicine (SBM) is because she is one of the foremost promoters of a particularly pernicious form of antivaccine misinformation that tries desperately to create a religious basis to oppose vaccines with antivaccine activism. It is a form of misinformation designed to deceive those who believe abortion is a moral wrong into thinking that vaccines, too, are a moral wrong because some of the viruses used to make specific vaccines are grown during the manufacturing process in cell lines derived from human fetuses decades ago. But Deisher goes one huge step beyond just guilt by association for vaccines. She is, as the news story cited above notes, the foremost promoter of a related and equally pernicious form of antivaccine information that claims that DNA from the fetal cell lines used to grow vaccine strains of viruses is a cause of autism. The truly depressing thing about Deisher is that she is, in fact, a real scientist (or at least was).
In any event, it occurred to me that, although I’ve mentioned Deisher briefly before in the context of the Disneyland measles outbreak, I’ve never deconstructed her antivaccine misinformation in detail here. Yet, her work is often cited by antivaccine activists to persuade those whose religion tells them abortion is morally wrong that they shouldn’t vaccinate their children by adding to the false claim that somehow “fetal parts” are used in the making of vaccines the even more false claim that fetal DNA somehow gets into the brain, recombines with the DNA in neurons, and causes autism. She’s also just released what appears to be a new paper claiming to show how fetal DNA causes autism. The confluence of her name coming up in stories about CMP and Planned Parenthood and her release of this new “paper” makes this a perfect time to write about Deisher.
Fetal cell lines and vaccines
Before I discuss Deisher’s pseudoscience about vaccines, I think it important to discuss briefly exactly how and when fetal cells are used to make vaccines. First, you need to realize that fear mongering about “fetal parts” in vaccines is, not surprisingly, a distortion of the real situation, which is that the human cell lines are used to make some vaccines. Specifically, the WI-38 cell line is a human diploid fibroblast cell line derived from a three month old fetus aborted therapeutically in 1962 in the US. Another cell line, MRC-5, was derived from lung fibroblasts of a 14 week old fetus in 1966 in the United Kingdom. These are currently the only fetal cell lines used to grow viruses for vaccines, with most other vaccines requiring cell lines from animals (which, of course, leads antivaccinationists to disparage them as “dirty” and using “monkey cells” and the like). In any case, the only commonly used vaccines in whose manufacturing these cell lines are utilized include:
- Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
- Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
- Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
- Zoster (shingles) vaccine [Zostavax/Merck]
There are more, but these are the main ones.
Although antiabortion antivaccine activists frequently try to make it sound as though scientists are aborting fetuses left and right just to grind them up to make vaccines (presumably twirling their mustaches and cackling evilly as they slice and dice them), in reality there are only two cell lines used this way, and they are so far removed from the original abortions that even the Catholic Church has told its members that not only is it morally acceptable to use such vaccines, but vaccinating children against deadly diseases is a great good. True, the statement from the Pontifical Academy for Life does urge scientists to develop vaccines that don’t use these cell lines, but it also concluded that the extreme good of protecting children’s lives far outweighs the distant evil (in the Church’s view) that created the cell lines, concluding in a FAQ, “There would seem to be no proper grounds for refusing immunization against dangerous contagious disease, for example, rubella, especially in light of the concern that we should all have for the health of our children, public health, and the common good” and “It should be obvious that vaccine use in these cases does not contribute directly to the practice of abortion since the reasons for having an abortion are not related to vaccine preparation.”
Overall, the view that somehow vaccines whose virus strains are grown in these two cell lines are the product of pure evil seems to rely on a magical thinking that an evil (in the view of those who oppose abortion) from over 50 years ago continues to taint these cell lines over hundreds of passages seems rather like the law of contagion in sympathetic magic, more than anything else. Of course, at some level, antivaccinationists probably know this, which is why they need more than just revulsion among those who belong to religions that teach that abortion is murder. Also, the number of people who would be persuaded by this line of attack is relatively small in this increasingly secular society. So antivaccinationists need more. Enter Theresa Deisher.
Fear mongering about fetal DNA in vaccines
Before I get to Deisher’s most recent paper, it’s worth discussing her background a bit, as well as what she has been claiming. I first “met” Deisher online in 2009, which is when I first encountered her particular variant of the claim that the fetal cells used to make certain vaccines somehow “contaminated” the vaccine in such a way as to cause autism when injected into babies. Here’s a sample published, appropriately enough, on Whale.to:
The earliest aborted fetal cell-produced vaccines such as Meruvax (rubella) and MMR II do not even inform consumers that the vaccines contain contaminating DNA from the cell used to produce them. Furthermore, it is unconscionable that the public-health risk of injecting our children with residual contaminating human aborted fetal DNA has been ignored.
How could the contaminating aborted fetal DNA create problems? It creates the potential for autoimmune responses and/or inappropriate insertion into our own genomes through a process called recombination. There are groups researching the potential link between this DNA and autoimmune diseases such as juvenile (type I) diabetes, multiple sclerosis and lupus. Our organization, Sound Choice Pharmaceutical Institute, is focused on studying the quantity, characteristics and genomic recombination of the aborted fetal DNA found in many of our vaccines.
Deisher isn’t the only one who’s been making this claim. For instance, I discussed a similar claim made by Helen Ratajczak, who specified that homologous recombination of fetal DNA in various vaccines with the DNA in babies’ brains results in altered proteins on the surface of neurons, provoking an autoimmune reaction. Homologous recombination is a process by which DNA strands with the same or very similar sequences can break and recombine.
This is an incredibly implausible hypothesis. If the fetal DNA did undergo homologous recombination, it would still be human DNA making human proteins. The body recognizes a cell as foreign or “altered” through the expression of its cell surface proteins. Consequently, the only likely currently known mechanism by which homologous recombination of human DNA from vaccines might conceivably result in such an autoimmunity phenomenon would be if the DNA from the vaccine somehow resulted in the expression of a foreign or altered protein on the cell surface that the immune system could recognize as foreign. That would mean either integrating into the gene for a cell surface protein or producing a cell surface protein itself. While not impossible, that’s pretty darned unlikely to happen on a scale that would affect more than a single cell, a few at most. To recap: To do what Ratajczak and Deisher claim, human DNA from vaccines would have to:
- Find its way to the brain in significant quantities.
- Make it into the neurons in the brain in significant quantities.
- Make it into the nucleus of the neurons in significant quantities.
- Undergo homologous recombination at a detectable level, resulting in either the alteration of a cell surface protein or the expression of a foreign cell surface protein that the immune system can recognize.
- Undergo homologous recombination in many neurons in such a way that results in the neurons having cell surface protein(s) altered sufficiently to be recognized as foreign.
- That’s leaving aside the issue of whether autoimmunity in the brain or chronic brain inflammation is even a cause of autism, which is by no means settled by any stretch of the imagination. In fact, quite the opposite. It’s not at all clear whether the markers of inflammation sometimes reported in the brains of autistic children are a cause, a consequence, or merely an epiphenomenon of autism.
In other words, this hypothesis is incredibly implausible on the basis of what we know about molecular biology and human biology. It’s not quite homeopathy-level implausible, but nonetheless incredibly implausible. Worse, Dr. Deisher should know this, given that she is actually a molecular biologist. Indeed, she has a PhD in Molecular and Cellular Physiology—egad, that’s the same field I have my PhD in!—from Stanford University and worked for 20 years in the biotech industry for companies like Amgen Genentech, Repligen, ZymoGenetics, and Immunex. Then something happened, though, and Deisher left the conventional biotech industry to found the Sound Choice Pharmaceutical Institute and AVM Biotechnology, the latter of which is described as the “premier pro-life biotech company worldwide, certifying that it does not use morally illicit material in any process.” SCPI is described as having been “founded to promote consumer awareness about the widespread use of electively aborted fetal material in drug discovery, development and commercialization” and having a corporate mission to “stop human trafficking and exploitation in biomedical research and commercial products.”
To this end, over the last six or seven years, Deisher has been publishing a stream of papers purporting to show that (1) vaccines manufactured using virus grown in cell lines derived from human fetuses correlate with autism diagnoses and (2) that there is fetal DNA in these vaccines that can recombine with infant DNA to cause autism. In trying to prove (1), Deisher has used the typical inept—or just plain bad—epidemiological techniques that have been used by antivaccinationists of all stripes since time immemorial (or at least since the 1980s). In particular, she is enamored of “change point” analyses to try to show that the rate of increase in autism prevalence changed at certain points when new vaccines were introduced. Unfortunately, she does a very bad job of doing actual change point analyses, as mathematician Mark Chu-Carroll has pointed out. Unfortunately, there’s more of the same in this paper, as you will see. As for demonstrating the presence of that evil fetal DNA, Deisher has been known to be—shall we say?—less than rigorous in her molecular biology techniques. Think of this paper as being like the sequel to a bad superhero movie: Bigger, faster, louder, but just as dumb.
No, actually, it’s even dumber.
Change points and dubious correlations
So now let’s take a look at Deisher’s paper, published in Issues in Law and Medicine and entitled “Epidemiologic and Molecular Relationship Between Vaccine Manufacture and Autism Spectrum Disorder Prevalence.” Helpfully, for those of you who don’t want to take my word for how embarrassingly bad this paper is and want to find problems with it that I either missed or ran out of time and space to discuss, Deisher has helpfully included a link to the PDF of her full paper on her website.
I always judge where the authors are coming from on a paper by their introduction. If their introduction is a balanced, reasonable discussion of the state of the evidence regarding their hypothesis citing good scientific papers, chances are that the paper will at least be reasonable, even if I end up not agreeing with its conclusions. However, if the introduction is biased and cites pseudoscientific papers, well, you know the rest of the paper is likely to be bad. Guess which category Deisher’s introduction falls under:
A worldwide autism epidemic is copiously established by the number of peer reviewed articles on the subject, including the observations from numerous institutions that de novo genetic insertions and mutations are excessive in children with autism.1 Autism disorder (AD), a subset of Autism Spectrum Disorder (ASD), is a neurological and developmental disorder whose symptoms usually appear within the first three years of life.2 The autism epidemic obviously creates significant public health burden and demands critical assessment of environmental factors that may trigger this epidemic. A previous publication from our group focused on overlooked, universally introduced environmental factors, including human fetal and retroviral contaminants in childhood vaccines, advancing paternal age and changes in diagnostic criteria. As the US Environmental Protection Agency (EPA) requires, discovery of potential environmental triggers for autism requires statistical assessment to identify birth year change points for autism spectrum disorder prevalence. Iterative fitting algorithms identified 1980.8, 1988.4 and 1996.5 as “changepoint” years for the United States AD prevalence,3 in substantiation of a report from the Environmental Protection Agency (EPA) that identified a 1988 worldwide AD change point.4
Note first, that there really isn’t a “worldwide autism epidemic.” Note also that Deisher’s previous papers she cites about “changepoint” years supposedly not related to changes in the DSM criteria for diagnosing autism and autism spectrum disorders are very bad papers that have been thoroughly deconstructed elsewhere. For instance, her 2010 paper used a highly dubious “changepoint analysis” that was statistically invalid and based on a whole lot of assumptions. Worse, it used two different data sets, and one of the change points just happened to show up at a year where the data switched over, as Mark Chu-Carroll points out:
So… Let’s summarize the problems here.
- They’re using an iterative line-matching technique which is, at best, questionable.
- They’re applying it to a dataset that is orders of magnitude too small to be able to generate a meaningful result for a single slope change, but they use it to identify three different slope changes.
- They use mixed datasets that measure different things in different ways, without any sort of meta-analysis to reconcile them.
- One of the supposed changes occurs at the point of changeover in the datasets.
- When one of their datasets shows a decrease in the slope, but another shows an increase, they arbitrarily choose the one that shows an increase.
You get the idea. Basically, as Mark described back then, you can always find “changepoints” if you iteratively partition the data into smaller and smaller sets, and, of course, mixing datasets the way Deisher did is a no-no. The main paper supporting this work is nonsense. So is Deisher’s 2014 paper, which suffers from the same problems. So already you know that where Deisher is coming from in this article is suspect. So what does she do wrong this time?
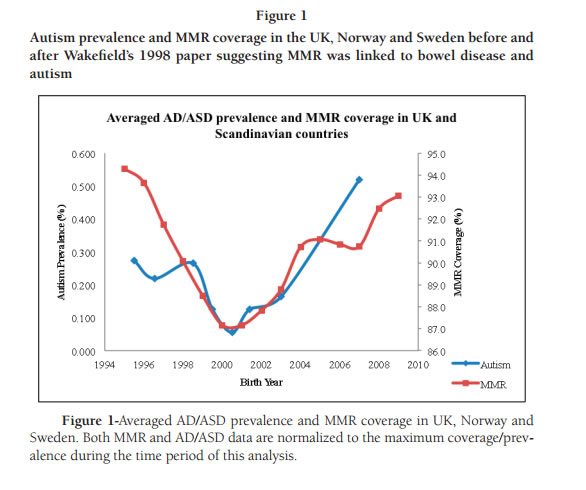
The basic hypothesis she is testing is whether, in the wake of the “Wakefield scare” that occurred after the 1998 publication of Andrew Wakefield’s now-retracted Lancet case series claiming to link the MMR vaccine to bowel problems in autistic children and that was later used to link the MMR to autism itself, which resulted in greatly decreased uptake of MMR, there was a similar decline in the rate of autism. That’s the epidemiological part. The other part of her paper consists of cell culture experiments purporting to show that the evil demon fetal DNA can recombine with human DNA. Let’s deal with the epidemiology first.
Lying with graphs
The most curious thing I noticed here was that Deisher combined data from three countries, Norway, Sweden, and the UK. Why these three countries? For instance, why not just the UK or, more specifically, England and Wales, where the impact of the Wakefield MMR scare was the most profound? Why not other European countries, such as France (which suffered some pretty severe measles outbreaks due to low MMR uptake as long as 13 years after Wakefield’s paper was published)? Moreover, in just the UK itself, even as far out as 2008-2009, there was wide variation by region in MMR uptake. In any case, using population data aggregated from three countries (even using country-level population data) is a great way to produce the ecological fallacy in a big way. It’s a problem we’ve seen before in papers claiming to link vaccines to autism and infant mortality.
But let’s concede this design to Deisher for a moment and assume that these three countries were in fact the most appropriate to choose to look at this “natural” experiment in which MMR uptake declined, allowing us to see whether there was a decline in autism prevalence in the birth years affected by the “Wakefield scare.” Note that in the analysis the decline in MMR uptake begins in the birth year before 1998 because children don’t receive all their MMR vaccines in their birth year. Of course, one problem that leaps out here is what, exactly, does Deisher mean by “MMR coverage”? Does she mean having received no doses of MMR? Not having received all the recommended doses of MMR? It’s not at all clear, and it’s very difficult to check what the heck she is talking about without actually contacting the Norwegian Institute of Public Health, the National Board of Health and Welfare in Sweden, and Public Health England, which are the data sources for MMR coverage reported in the paper. In other words, anyone wanting to check Deisher’s work either has to contact her or replicate her requests for these data.
How the data for each country are aggregated becomes problematic as well, mainly because it is unclear how Deisher did it. Did she, for example, weight the MMR uptakes by population when averaging them? I hope she did at least that much, but we have no way of knowing whether she did. What about autism prevalence? There are wide variations in reported autism prevalence between nations in different years. For instance Table 1 shows a prevalence of 0.29% in Norway and 0.038% in Sweden for birth year 2003. That’s a 7.6-fold difference! Yet, in Figure 1, the point plotted for the same birth year is around 0.17% or so. Given that the mean of 0.038 and 0.29% is 0.164%, it makes me wonder if Deisher just averaged the prevalences without taking population into account. The population of Sweden was nearly twice that of Norway in 2003 (8.96 million compared to 4.56 million), so it makes a difference.
Now let’s take a look at the graph in Figure 1:
How bad it this graph? Let me count the ways…
If you want to see dishonesty in the use of scales on axes, here you have it. Notice how the curve for autism prevalence has a y-axis (left) has a range from 0 to 0.6%. Now notice the y-axis (right) for MMR coverage. Notice anything? That’s right, the MMR coverage axis only ranges from 86% to 95%, thus making small absolute changes in MMR uptake look enormous. Indeed, if the MMR uptake y-axis were presented from 0 to 100%, the curve would go nearly flat. Don’t believe me? Check out a re-normalized graph, courtesy of Matt Carey:
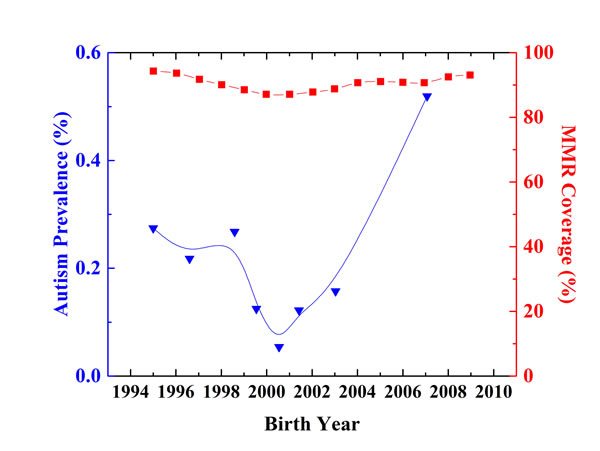
See how different the data look if you present them properly?
Wow. That’s different, isn’t it?
It’s a classic deceptive technique all too commonly used with graphs, which is why I call this lying with graphs. Indeed, if we were to take these graphs at face value, a 10% drop in MMR uptake resulted in a 60% drop in autism prevalence. That’s some powerful fetal DNA! If this model held (at least in a linear fashion), there’d have been no autism if MMR uptake fell below 75%. In any case, if this association were real, MMR uptake should account for less than 100% of autism prevalence, but that’s not what this graph shows. It’s utter nonsense. In fact, I’m embarrassed for Deisher. As someone with a PhD in the same field as Deisher, I’m ashamed that someone like her has a doctorate in the same as I do.
But it’s worse than that.
Look even more closely. For birth years 1995 and 1996, there are only data shown from the UK. Looking at Figure 1, I see that the graph appears to show those numbers from the UK for those two birth years. I kid you not. Look for yourself. For 1995, the prevalence graphed appears visually to be around 0.28%. The number reported in Table 1 is 0.274, pretty similar. I bet Deisher used 0.274% for that point. For 1996, the number graphed appears on a visual basis to be around 0.21% or 0.22%. The number reported in Table 1 is 0.219%, again suspiciously similar. We can do this same exercise for other birth years not represented by other countries, for instance 2007, which only has data from Sweden, listing a prevalence there of 0.52%. Now let’s look at the graph again. Yep, the point for birth year 2007 sure looks to be a little more than 0.50% and could well be 0.52%.
In other words, we have a graph showing a conglomeration of MMR uptakes that are not defined and whose provenance we can’t examine without a great deal of work, being correlated with figures from three countries that are incomplete and don’t contain values for each birth year presented on the graph. For years where there are values for more than one country, it appears that Deisher just did an arithmetic mean (as she appears to have done for birth year 2003) without correcting for population differences between the countries, and for years where she only has one country’s worth of data she just uses that on the graph. Then, to top it all off, Deisher deceptively fiddles with the Y-axis to make small differences in MMR uptake look enormous. Next, she says that both “MMR and AD/ASD data are normalized to the maximum coverage/prevalence during the time period of this analysis.”
I’m still scratching my head over what all this is supposed to mean. For instance, how do you normalize to get an autism prevalence of 0.12% in Sweden in birth year 1998? What was the maximum autism prevalence normalized to? The same problem occurs for MMR uptake. What do these values between 87% and 94% MMR uptake mean? How do you normalize to get them? What was the highest uptake normalized to? The whole thing is a mess so ridiculous that it can only be due to gross incompetence on an epic scale or deliberate deception coupled with utter contempt for the antivaccine audience who is expected to eat this crappy science up. Take your pick.
But what about the cell culture?
I almost left this section out because after the epic nonsense in the epidemiology part of this study, I almost—almost!—don’t care about all the cell culture studies presented because they really don’t have any relevance to anything claimed by Deisher in her epidemiology. After all, Deisher is trying to argue that there was a correlation between a decline in MMR uptake and a decline in autism prevalence. So Deisher found some human double- and single-stranded DNA in vaccines, specifically Meruvax II and Havrix. Most of the DNA was short (around 215 base pairs), but the DNA from Havrix did not migrate through an agarose gel, suggesting that it is at least several thousand base pairs long. So far, this is not a huge deal.
Next up, Deisher examined whether human Cot1 DNA could be taken up by cells. Cot1 DNA is DNA from human placenta consisting of fragments measuring 50 to 300 bp in length, enriched in repetitive sequences, such as Alu and Kpn family members. The common use for Cot1 DNA is as an agent to block nonspecific hybridization in microarray experiments and the suppression of repetitive sequences. If you don’t know what that means, don’t worry. Suffice to say that this is DNA with highly repetitive sequences different from the presumably more or less random fragments of DNA from the cell lines used to make the vaccines. In any case, Deisher labeled this DNA and incubated it with human cell lines at a concentration of 500-750 ng of DNA per 107 cells. Basically, the DNA was added to the media and the cells gently shaken over 24 to 48 hours before cells were examined for uptake of labeled DNA, and—lo and behold!—Deisher found DNA uptake in some of the cell lines.
Here’s the problem. This is a highly artificial experiment. For one thing, 750 ng of DNA is a lot of DNA, and it’s being put into only a few milliliters of medium and ten million cells, which is not a huge number either. Compare this to the amount of DNA found in each vaccine. The most DNA found by Deisher in any vaccine was 276 ng single-stranded and 36 ng double-stranded DNA per vial. This is injected into muscle. Also remember that the Cot1 DNA is double-stranded. In other words, Deisher’s experiment isn’t even remotely relevant to real life! Basically, she ramped up the concentration of DNA per number of cells to a level that has no direct relevance to physiology, marveled when she found that these cells, when flooded with DNA, actually do take up some of it, and is now claiming that her experiment indicates a grave problem that desperately needs to be studied:
In summary, vaccines manufactured in human fetal cell lines contain unacceptably high levels of fetal DNA fragment contaminants. Human DNA fragments of similar length and epigenetic signature spontaneously integrate into the genome of primitive cell lines, a process that can be augmented in the setting of inflammation. The human genome naturally contains regions that are susceptible to double strand break formation and DNA insertional mutagenesis, regions that are particularly concentrated within the exons of genes that have been shown to be causative or associated with ASD phenotype. The ‘Wakefield Scare’ created a natural experiment that indicates a causal relationship between fetal cell-line manufactured vaccines and ASD prevalence. Our paper calls for additional study and investigation of this potential relationship.
Deisher’s study shows nothing of the sort. She found some cellular DNA uptake using a very high concentration of DNA and also observed found some integration of that DNA in the chromosomes of cultured cells. Of course, Alu and Kpn repeats are very common in the genome; so by choosing Cot1 DNA Deisher virtually guaranteed there would be a lot of sites where any DNA that got into the nucleus could pair with and undergo homologous recombination. Her experiment is not at all analogous to what DNA from a vaccine would do, if it could even get past the blood-brain barrier and obtain access to the infant’s neurons.
The bottom line
Theresa Deisher is a puzzling and sad case. A real molecular biologist who did real research for various biotech and pharmaceutical companies, apparently competently, for 20 years, she suddenly embraced antivaccine pseudoscience, apparently based on her embrace of fundamentalist Catholicism. Complicating this story is that Deisher’s son Henry Streuli developed an aggressive Burkitt’s lymphoma, which recently claimed his life. Henry’s long struggle with what ultimately turned out to be a fatal cancer for him appears to have led Deisher to think that vaccines cause childhood cancers in addition to autism. (She started linking fetal DNA in vaccines to autism in 2009; Henry was diagnosed with Burkitt’s lymphoma in 2014.) Although conservative Catholicism appears to be what first led Deisher to embrace her pseudoscientific hypothesis about fetal DNA in vaccines and autism, the tragic death of her child less than a month and a half ago is unlikely to do anything but cement in her mind the evils of vaccines made using fetal cell lines.
As much sympathy as I might feel for Deisher’s having to watch her 14 year old son battle and ultimately succumb to cancer at far too young an age, given how she has become the foremost promoter of the pseudoscientific antivaccine talking point linking fetal DNA in vaccines, I can’t hold back deconstructing her pseudoscience, weak arguments, and demonization of vaccines because I feel sorry for her. Nor can I fail to note that her original idea that fetal cell DNA in vaccines causes autism was almost certainly religiously motivated and developed long before her son developed cancer. As a (highly) lapsed Catholic myself, I can understand how people believe abortion is wrong. What I can’t understand is how one can use that moral belief to demonize something that even her own Catholic Church finds morally acceptable, or at least morally tolerable. Finally, what I really can’t tolerate is science this bad, particularly from someone who used to be, from all accounts, a decent scientist.