
{kind=link}
A mere couple of weeks ago, our fearless leader and founder, Dr. Steve Novella, found an example of a credulous take on acupuncture of the sort that I couldn’t recall having seen in years and years, deconstructing it as deftly as usual. This promotion of acupuncture took the form of an article in the Proceedings of the National Academy of Sciences (PNAS), and Dr. Novella quite rightly called it an example of the “disastrous double standard” in which “regular medicine is held to a high standard, while ‘alternative’ medicine has a standard all its own,” accurately describing the article as “completely gullible, written as if it were a promotional piece entirely by advocates, without a hint of critical thinking or skepticism.” What was particularly disturbing about this article was, of course, that it was published in the official journal of the National Academy of Sciences. As a bit of history, I will mention that PNAS was long problematic, basically the journal into which Academy members tended to dump work that they had trouble getting published elsewhere, largely because Academy members could in the past basically publish almost anything in PNAS, either themselves or as the Academy member submitting favored work by someone else. (It’s how two-time Nobel Prize winner Linus Pauling first got his horrible studies on using vitamin C to treat cancer and the common cold published in the 1970s.) However, in recent years, PNAS has tightened its editorial standards so that members can’t just publish, in essence, anything they want. It appears, however, that the editors have a ways to go when it comes to not publishing ridiculously credulous propaganda about “integrative medicine” and traditional Chinese medicine.
The current example comes not from an academic journal, but from National Geographic. Written by Daniel Siefert, the article is entitled Scientists are finally decoding how acupuncture eases pain. (Spoiler alert: No, they aren’t. Seriously, they aren’t. Certainly no good evidence is cited in this article to support such a conclusion, other than a clinical trial that, above all, once again supports the conclusion that acupuncture is a theatrical placebo.) Before I proceed, in the name of total transparency, I will point out that from 2006-2017 I regularly blogged for a collective known as ScienceBlogs. (May it rest in peace.) This is relevant because National Geographic purchased ScienceBlogs and owned it until its demise in 2017, which meant that I blogged for NatGeo for six years and collected maybe a few thousand dollars in blogging income during the course of that time period. (Honestly, I don’t remember and don’t feel like looking it up. It was several hundred dollars a year.) There you have it, my conflict of interest. Make of it what you will. Also, I am aware that NatGeo has been problematic for several years, since it was acquired by 21st Century Fox in 2015, which was then acquired by The Mouse (Disney) in 2017. (Yes, NatGeo is owned by Disney, like, seemingly, most media these days.) Also, in 2023 NatGeo laid off all its staff writers and switched to a freelance-only model, ultimately ceasing publishing newsstand editions in 2024. So it’s less of a surprise that NatGeo would go all-in on promoting acupuncture, but nonetheless disappointing to those of us “olds” with fond memories of reading our parents’ issues decades ago.
Now, let’s get to the credulous take on acupuncture.
Acupuncture is science, ma-an!
One of the key (and ubiquitous) claims made in pretty much every piece of acupuncture propaganda tarted up as a news feature (as in PNAS) or a serious article for a lay audience (as in NatGeo) is that “Western science” is finally starting to understand the biochemical and physiological mechanisms that “explain” how the “ancient wisdom” of acupuncture does the miraculous things claimed for it. It’s a gambit that I like to describe as saying, “Acupuncture is science, ma-an!” or “‘Western science’ is finally validating Eastern mysticism!” And, make no mistake, as I’ve described many times, acupuncture is based on a prescientific understanding of how the human body works and what causes disease and other physical symptoms. There is no such thing as “qi,” the mystical magical “life force” energy that supposedly magically wends its way down acupuncture meridians and whose flow is “unblocked” by placing needles somewhere along said meridians. (How? Who knows? Don’t ask, unbeliever!)
Unsurprisingly, NatGeo follows this script quite slavishly:
A needle prick doesn’t seem like it should quiet severe pain. But in some cases, it does—easing migraines, dulling pain, even helping patients endure childbirth. In one randomized trial in emergency settings, acupuncture relieved acute pain more quickly and effectively than intravenous morphine, with fewer side effects.
Acupuncture, a practice rooted in Traditional Chinese Medicine (TCM), has long occupied a gray zone between medicine and mystery: widely used to treat pain, yet often dismissed as a placebo.
But advances in imaging and clinical research are shifting that view. Scientists are uncovering how a needle can trigger a chain reaction inside the body, activating immune cells, releasing pain-modulating chemicals, and altering brain activity. What’s emerging is a clearer picture of a measurable, body-wide response—one that is helping position acupuncture as a low-cost, non-addictive option in pain management worldwide.
At the risk of being too repetitive of Steve’s points a couple of weeks ago, I nonetheless find it useful to compare the above passage from NatGeo to a (very) similar passage in the PNAS article. It’s almost as though these articles follow a script:
Although the picture remains incomplete, several lines of research are elucidating the biological underpinnings of acupuncture. They include the involvement of endogenous opioids and the role of loose connective tissue—including fascia, a body-wide network of collagen fibers embedded in an extracellular matrix rich in hyaluronic acid and other proteins. This tissue could be the medium that transmits the effects of local needling to distant systems, echoing the TCM concept of meridians.
By giving ancient ideas a modern scientific footing, recent discoveries are bolstering Western acceptance and strengthening the case that acupuncture’s benefits are not just a placebo effect. “Clinical evidence is important,” says Peter Wayne, director of research for the Osher Center for Integrative Health at Harvard Medical School and Brigham and Women’s Hospital, in Boston. “But without plausible mechanisms, community uptake is much slower.”
Western science and technology are also creating opportunities to enhance acupuncture practice with knowledge from the burgeoning field of bioelectronic medicine (1). Still, many researchers and practitioners marvel at the sophistication of the original practice. “How on earth did they understand that a point lateral in the fifth digit of the foot connected to the eye system?” asks Jeremy Pulsifer, an acupuncturist in New York City. “Modern science is finally saying, ‘We don’t know how they knew, but somehow there was an awareness that is far more sophisticated than we’ve ever given them credit for.’”
See what I mean about the ubiquitous propaganda narratives that “Acupuncture is science, ma-an!” and “‘Western science’ is finally validating Eastern mysticism!” The PNAS article even marvels at how “sophisticated” the ancient Chinese were. You’ll note additional narratives, the most prominent of which is what I like to call “Meridians are anatomy, ma-an, not bullshit.” (Hint: They’re bullshit.)
As I read the NatGeo article, one thing that irritated the crap out of me were all the claims made without any links to the actual studies or articles in which the study results being cited were reported—with only a handful of exceptions. Seriously, when I read the part about how acupuncture in the emergency room supposedly worked better than morphine for pain, I cringed, because no link was provided. I did, however, immediately recognize that Seifert was likely referring to a 2016 clinical study examining the use of acupuncture in the emergency room, published in 2016 in The American Journal of Emergency Medicine, entitled Acupuncture versus intravenous morphine in the management of acute pain in the emergency department. Having a long history with this subject is definitely useful, because I also remembered that I had deconstructed that article in depth soon after it was published, which is why I will not go into detail here other than to point out that there were a lot of problems with the study that led me to conclude that it did not even come close to showing what its conclusions claimed that the data showed. (It’s also possible that Seifert was referring to a different “emergency acupuncture” study that I deconstructed in 2017, but I doubt it, not that it isn’t worth clicking on the link to my old post and enjoying my amusing riffing on one of my favorite 1970s TV shows that I loved when I was a teenager, Emergency! In any case, the claim that acupuncture is better than morphine for pain relief is just another way in which purveyors of unscientific “integrative” medicine see the opioid crisis as an opportunity to peddle their pseudoscience.
As for migraines, Dr Novella, neurologist that he is, has written a number of times about how acupuncture doesn’t work for migraines, dating back at least to 2012. As for easing “chronic pain,” apparently the best reference Seifert could come up with was a KFF article on Ukrainian volunteer acupuncturists working to help rehabilitate veterans of that country’s war with Russia (there’s no good evidence that acupuncture relieves chronic pain), while the evidence that acupuncture can ease the pain from childbirth is a press release from the University of California-Irvine, which, as you might recall, is deep into “integrative medicine” nonsense, thanks to $200 million in funding from the wealthy homeopathy-loving couple, Susan and Henry Samueli, turning UCI into a wretched hive of scum and quackademic medicine.
Next up, following the script, are the supposed “findings” that “prove” that there’s something to acupuncture and that it’s science ma-an, starting with the “ancient wisdom meets cutting edge science and technology” narrative in which those nasty “Western” scientific and medial “skeptics” are slowly being convinced by the overwhelming weight of fantastic evidence being produced by modern science, thus narrowing the chasm between TCM and science:
For centuries, the language of Traditional Chinese Medicine—concepts like meridians and qi, or vital energy—left many Western researchers unconvinced.
That disconnect is now narrowing. As clinical research has progressed, scientists are gaining a clearer picture of what happens when a needle meets tissue, says Mingxiao Yang, an assistant professor at Nanyang Technological University in Singapore, whose integrative health lab explores TCM through cutting-edge technology.
The response begins locally. The slight mechanical tug of a needle, known as mechanotransduction, sets off a cascade of biochemical signals in the surrounding connective tissue. This activity causes skin mast cells (think of them as your body’s first line of defense) to release compounds such as histamine, serotonin, and adenosine into nearby tissue. Those signals then stimulate nerve endings, sending messages to brain regions involved in processing and modulating pain.
Acupuncture may also engage broader pain-regulation pathways, including a “pain inhibits pain,” sensation, in which one stimulus can dampen the perception of another, Yang explains.
The above narrative is nothing more than a combination of very old claims by acupuncturists that acupuncture “works” by releasing endorphins, adenosine, and other substances locally, supposedly magically transporting those pain-suppressing signals to the brain. Mark Crislip long ago reviewed the evidence for the “endorphin hypothesis” and found it wanting, while I’ve written multiple times since 2010 about how unconvincing the evidence for locally released adenosine as the mediator of the claimed analgesic effect of acupuncture has been. All of the above is handwaving nonsense, as are the references to X-ray studies showing “immune cells drifting toward acupuncture needles, where they release pain mediators,” ultrasound showing “the ripple effect of a needle’s tug in real time and how those effects may vary depending on where a needle is placed,” and this lovely passage that basically says that acupuncture is placebo:
Psychologically, the mere anticipation of potential healing plays its own role too, Yang adds. “Treatment expectancy and belief, mediated partly through the brain’s reward circuitry, may also contribute to acupuncture-induced pain relief.”
It’s amazing how acupuncture believers admit explicitly that acupuncture is a placebo without saying explicitly that acupuncture is a placebo, isn’t it?
Then there’s this doozy:
Researchers have reported an 80 percent overlap between classical meridian pathways and connective tissue networks, regions that appear to contain higher densities of nerve fibers than surrounding areas. One analysis found that these dense points may contain 1.4 times as many nerve fibers as non-acupoints.
“The traditional map of the meridians should be reinterpreted as a profound, ancient blueprint of the body’s neural and fascial networks,” says Judith Schlaeger, a professor at the College of Nursing at the University of Illinois in Chicago. “The most effective points are often those that act as high-access ports to the nervous system.”
Wow! 1.4 times as many nerve fibers? Seriously, that’s not very impressive, even if I actually accepted the evidence as spun in the review article cited, which is published in a credulous traditional Chinese medicine journal, as reliable and science-based. As for the 80% overlap claimed, guess whose lab produced the paper cited? Yes, it’s the Helene Langevin, a somewhat regular topic of this blog because she is the Director of the National Center for Complementary and Integrative Health (NCCIH), and, more importantly for purposes of this post, someone who has long been known for desperately trying to use ultrasound studies on cadavers and living humans to claim to find anatomic correlates with acupuncture meridians. Let’s just put it this way. Acupuncture meridians are lines imagined on the extremities and the torso that head towards the spine and brain. Of course some of them track somewhat closely with the paths of major nerves and blood vessels, because that’s how the human body is put together! This coincidence doesn’t imply that meridians and acupoints have consistent anatomical correlates, the efforts of acupuncturists and believers to argue that they do, to the point of mapping these correlates to animals such as dogs and even elephants, notwithstanding.
Before I move on to the study that gets the most attention from Seifert, I think it’s worth pointing out the revisionist history of traditional Chinese medicine championed by Chairman Mao and, since Mao’s death in the 1970s, successive Chinese governments. People seem to think that what is now considered “acupuncture” has always been the same dating back thousands of years, with thin needles precisely inserted into acupoints along meridians, when this form of acupuncture has only predominated for around a century. Dr. Harriet Hall once discussed the memoir of a Scottish surgeon named Dugald Christie who had served in China as a missionary for three decades spanning the late 19th and early 20th centuries, quoting his account of what passed for acupuncture during that time:
Chinese doctors own that they know nothing at all of surgery. They cannot tie an artery, amputate a finger or perform the simplest operation. The only mode of treatment in vogue which might be called surgical is acupuncture, practised for all kinds of ailments. The needles are of nine forms, and are frequently used red-hot, and occasionally left in the body for days. Having no practical knowledge of anatomy, the practitioners often pass needles into large blood vessels and important organs, and immediate death has sometimes resulted. A little child was carried to the dispensary presenting a pitiable spectacle. The doctor had told the parents that there was an excess of fire in its body, to let out which he must use cold needles, so he had pierced the abdomen deeply in several places. The poor little sufferer died shortly afterwards. For cholera the needling is in the arms. For some children’s diseases, especially convulsions, the needles are inserted under the nails. For eye diseases they are often driven into the back between the shoulders to a depth of several inches. Patients have come to us with large surfaces on their backs sloughing by reason of excessive treatment of this kind with instruments none too clean.
Speaking of the “excess of fire” in the child’s body, I like to point out that TCM has a lot in common with “Western” humoral theory. For example, humoral theory has the four humors, blood, yellow bile, black bile, and phlegm, imbalances of which were thought to cause disease and whose “balance” physicians tried to restore, dating back to the time of Hippocrates and continuing until nearly the time of Dugald. TCM, on the other hand, has the Five Elements (wood, fire, earth, water, and metal), and diseases are thought to be due to imbalances of the characteristics of these elements, such as heat/fire and dampness/dryness, whose “imbalances” are corrected by TCM. Interestingly, there is evidence that much of the “theory” behind acupuncture was heavily influenced by astrology and that there are sufficient similarities between needling in China and bloodletting in Europe to warrant strong suspicion that both practices grew from the same conceptual framework.
Another aspect of the revisionist history of acupuncture embodied in the PNAS and NatGeo articles comes from the little-known history of the needles themselves. It turns out that the thin filiform needles now associated with acupuncture didn’t exist until less than 100 years ago. Before that, needles were large and coarse, as described by Dugald. Indeed, in the first two decades of the 20th century, acupuncture was falling out of favor, and it wasn’t until the 1930s that a Chinese pediatrician named Cheng Dan’an proposed that needling therapy be resurrected because (he thought then) its actions could be explained through neurology. He also replaced the previously used coarse needles with the fine filiform needles in use today. No wonder there are so many “styles” of acupuncture. Then, in the 1940s and 1950s, Chairman Mao, facing a shortage of science-based physicians, started promoting TCM and acupuncture not just to his own people but to the “West” as evidence of the superiority of eastern medical systems, complete with reports of “acupuncture anesthesia,” which Dr. Kimball Atwood discussed early on in the history of SBM in epic fashion in a series entitled “Acupuncture Anesthesia”: A Proclamation from Chairman Mao (Part I, Part II, Part III, Part IV, and Part V). It is a tradition that even the rapaciously state-managed capitalism of today’s China can’t resist continuing to promote.
Acupuncture is real, not a placebo, ma-an!
The article’s last half is mostly about a study that is represented as slam-dunk evidence to silence the doubters who argue that acupuncture is an elaborate placebo (which it is). I’ll cite Seifert before turning my attention to the actual study:
For decades, one question has lingered: Does acupuncture work beyond the placebo effect? Answering that has proved difficult.
“The ‘true face’ of acupuncture remained elusive,” says Schlaeger. “Investigators lacked the ability to use the definitive clinical methodology—the double-blind randomized controlled trial—to separate acupuncture’s genuine physiological effects from the placebo effect.”
That barrier may finally be shifting. Her team has just completed what they describe as the world’s first double-blind acupuncture trial (where neither the participants, 89 women suffering from chronic vulva pain, nor the researchers themselves knew if real or sham needles were administered).
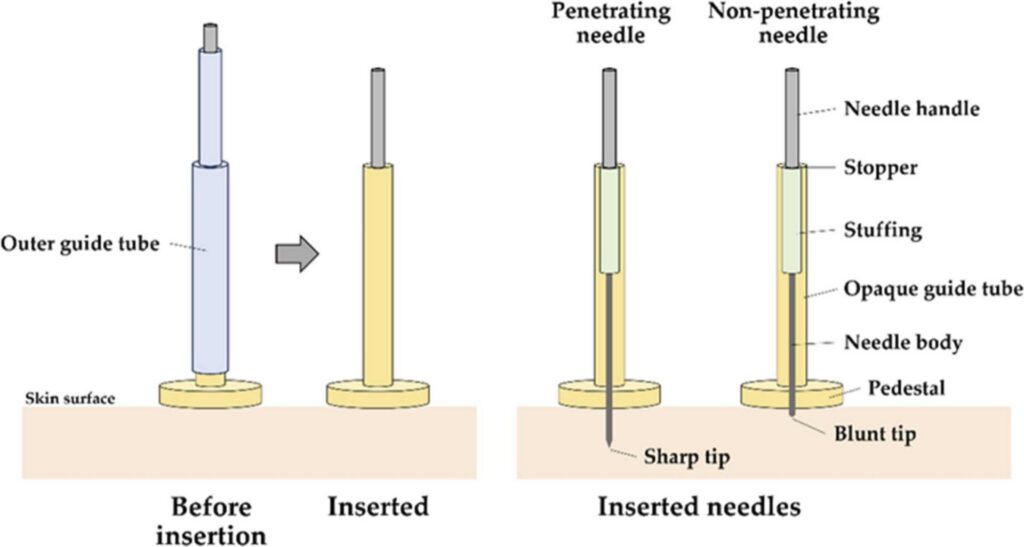
“The trial was made possible by a specially designed placebo needle, developed by Nobuari Takakura of Tokyo Ariake University of Medical and Health Sciences, which conceals the depth of needle penetration. He explains that “without a double-blind study environment, the decoding of the mechanisms of acupuncture would be impossible, because investigators wouldn’t be able to distinguish its true physiological effect from the power of expectation.”
Wait, what? The world’s first double-blind acupuncture trial, you say? Seriously? We at SBM have been deconstructing double-blind acupuncture trials for a long time, and Dr. Novella even noted in 2008 that techniques to study acupuncture using double-blind trial designs had been developed. That same year, I snarkily pointed out the dangers of using valid placebo controls in clinical trials of acupuncture, namely that double-blind studies show no difference between placebo/sham acupuncture and “real” acupuncture. No, believers have been doing double-blind trials of acupuncture for close to two decades. They just don’t like them because the answer is almost always that sham/placebo acupuncture performs no better than “true”/”real” acupuncture in double-blinded trial designs. Indeed, if there’s one thing that’s pretty consistent about randomized double-blind placebo-controlled trials of acupuncture, it’s that sham acupuncture used as placebo is generally indistinguishable from “real” acupuncture. In brief, it doesn’t matter where you stick the needles. The result is the same and easily attributable to placebo effects. Nor are whatever needles used in this study the first needles that conceal the depth of penetration of the needle. We at SBM have been writing about studies using various designs of such needles for at least 15 years.
But, hey, who knows? Maybe this study is the one! You never know.
The study, Long-lasting effect of penetrating acupuncture among responders: Double-blind RCT of acupuncture for vulvodynia, was published in January in The Journal of Pain. Unsurprisingly, I saw an old not-a-friend-of-the-blog, Ted Kaptchuk, listed as one of the authors. Kaptchuk, you might recall, is a tireless promoter of acupuncture and, in other contexts, is known for promoting the idea that it is possible to harness the placebo effect without deceiving the patient. We, of course, have pointed out that his studies show nothing of the sort.
First off, what is vulvodynia? The authors start right out describing this horrible, debilitating condition before pivoting to why they think acupuncture can help:
Vulvodynia is vulvar pain of unknown etiology that lasts at least 3-months, may have other potentially associated factors, and affects 7% of American women.1–3 The pain of vulvodynia renders sexual intercourse virtually impossible and devastates intimate relationships.4–6 Seventy percent of women with vulvodynia report severe pain (greater than 6/10).7 To reduce their pain 60% use alcohol and 43% use alcohol with analgesics (including opioids).8 The severe chronic pain of vulvodynia may lead to physical disability9 and even suicidal ideation.10 The two most common subtypes of vulvodynia are provoked vestibulodynia (PVD), pain limited to the vulvar vestibule and vaginal introitus that is provoked by touch,11 and generalized vulvodynia, spontaneous diffuse vulvar pain that can spread to the perineum and inner thighs.7 Although many have been tried, few therapies have been proven efficacious.12
Acupuncture has been shown to be effective in a meta-analysis of 39 high-quality randomized trials of acupuncture in 20,827 patients for the treatment of four chronic pain conditions: nonspecific musculoskeletal pain, osteoarthritis, chronic headache, and shoulder pain (all p <.001).13 In contrast to these four chronic pain conditions,13 there have been only six acupuncture studies14–19 of which two had acupuncture sham-control focused on feasibility17,18 and four14–16,19 provided some evidence of the effect of acupuncture on vulvodynia. In all of them, women who received acupuncture had less pain, better quality of life, improved sexual health, and improved mental health. However, three were single-group uncontrolled acupuncture studies and none were blinded,14–16 which limits conclusions about the efficacy of acupuncture for vulvodynia.
As you can see, vulvodynia is one of those conditions for which, unfortunately, science-based medicine doesn’t have a good pathophysiological explanation or good treatments that reliably bring relief. Unsurprisingly, the authors are citing one of the meta-analyses by Andrew Vickers that claim to show that acupuncture works but, when examined more closely, do not. Both Dr. Novella and I have both explained why the original Vickers meta-analysis doesn’t demonstrate that acupuncture works. The rest of the studies cited are the usual hodgepodge of dubious studies.
Let’s see how Seifert spins the results of the study, and then I’ll look at the study itself:
The team’s findings, recently published in the Journal of Pain, show that both real and sham acupuncture work can provide relief, just not equally. True acupuncture offers much longer-lasting relief of up to 12 weeks in some cases, while relief from the placebo diminished after four weeks. Since true acupuncture creates a micro-injury that releases a burst of chemical substances, “the central nervous system is excited,” Schlaeger explains, “triggering the body’s natural long-term repair mechanisms”
Takakaura adds, this shows that while the placebo-powered relief of ‘the ritual of care’ exists, “relief fades quickly because there is no lasting stimulus. This is the clear boundary between the fleeting nature of placebo versus the sustained effect of a true intervention.
Even so, questions remain. Larger studies and replication will be needed to confirm these findings and determine how broadly they apply.
Spoiler alert: More studies won’t quite confirm these findings, other than that they will likely confirm that there is no difference in pain relief between sham and true acupuncture; that is, unless they are not truly double-blind:
Eligibility criteria included:
- vulvar pain for at least 3-months duration
- a vulvodynia diagnosis as determined by gynecologic exam
- at least 18 years old
- spoke and read English at the initial screening
- a Tampon Test self-reported vulvar pain intensity score of 4 or greater on the Pain Intensity Number Scale (PINS 0–10) after inserting and removing a tampon because in women with vulvodynia, the pain of inserting and removing a tampon is significantly correlated with daily vulvar pain and dyspareunia (pain with sexual intercourse)
- be acupuncture naïve to enable participants to be blind to group allocation.
Exclusion criteria included conditions that can cause vulvar and vaginal pain but are not vulvodynia:
- pain secondary to atrophic vaginitis
- current vaginitis (candida, bacterial vaginosis, trichomonas vaginalis)
- inflammatory conditions
- neoplastic disorders of the genitals, including cancer or pre-cancer of the vulva, or Paget’s disease
- neurologic disorders affecting the genitals including pudendal nerve entrapment
- spinal cord nerve compression
- genital trauma
- history of surgery radiation, or chemotherapy to the genitals
- hormonal deficiencies.
- pregnancy because, amazingly, “some of the acupoints in the protocol are forbidden in pregnancy,” and I have no idea why.
Here’s the flowchart of study procedures:

And here is the needle design:
And here are the acupoints that were used:

These points do not have any anatomic relationship to the vulva or vagina other than maybe the ones over the groin, but only because they are the closest to the anatomic areas targeted.
The results were pretty unremarkable. Among the 89 women who participated in the study, there was not even a whiff of a hint of a statistically significant difference between the sham and true acupuncture groups for the primary outcome of vulvar pain, in any of the secondary outcomes, such as dyspareunia and the tampon test. Moreover, the percentage of responders was similar in both groups: acupuncture 58%, placebo 57%. I also note that on the ten-point pain scale, the improvements noted in both groups were quite modest, with effects so small that I really do have to wonder if they were at all clinically relevant, a problem many of these acupuncture studies that I discussed in detail when I deconstructed the 2012 Vickers meta-analysis. None of this stopped the authors from analyzing the “responder-participants” using a Kaplan-Meier curve that purports to show that the rate at which the participants’ symptoms returned to baseline was slower for the “true” acupuncture group, with the responders showing, according to the authors, a “consistently higher rate of return to baseline pain during the 12-week post-treatment follow-up in the placebo group compared to the acupuncture group (hazard ratio: 2.72, 95% CI: 1.13–6.54).”
Does this mean anything? Who knows? One big flaw that I saw in the study right away was that the blinding was uneven, with more participants in the “true” acupuncture group guessing correctly which group they were in at baseline and ten weeks compared to the sham acupuncture group. The authors also noted:
However, most of the acupuncturists did not maintain the blind in this double-blind, multi-needle, multi-session study. Therefore, provider expectations, conveyed nonverbally and not measured, may have influenced participant outcomes.63 The finding that the skin-touch placebo achieved blinding for the participants, thus reducing the risk of bias, is further evidence it serves as an acupuncture placebo.64
So, basically, this was an attempt at a double-blind study, but as carried out it wasn’t really completely double-blind. To be fair, this is a problem that all investigators carrying out placebo-controlled RCTs for interventions designed to relieve symptoms with a heavy subjective component, like pain, not just those pursuing acupuncture RCTs. The problem is not that the blinding didn’t work perfectly. That happens not infrequently in RCTs that aren’t for a drug for which a placebo indistinguishable from the drug can easily be made. The problem is how the results of the study were spun.
Specifically, here comes the hand-waving:
This trial revealed the true efficacy of penetrating acupuncture under a rigorous experimental protocol; however, the control of the treatment environment may not adequately represent the actual clinical benefits for patients receiving acupuncture treatments as part of their care. There may be synergy between the acupuncture effect, the therapeutic effect of the relationship between the acupuncturist and participant, and the calming effect of common rituals, such as playing music,62 to enhance the efficacy of acupuncture. Therefore, more clinical benefit than that indicated by the results of this study can be expected. Future studies are needed to clarify the potential of such synergies when using penetrating or placebo needles.
In the duration-of-effect phase of this study, the longer lasting effect of acupuncture is to be expected because it is known that placebo effects do not last as long as treatment effects.60,71 A single systematic review72identified the placebo effect over time for acupuncture treatment periods ranging from 3 to 12 weeks. In the review, the placebo effect increased from baseline up to 12 weeks and then began to decrease. In contrast, findings from the responders after the RCT’s 10 sessions over 5 weeks suggest that the placebo effect diminished after 4 weeks, but the acupuncture effect persisted for 12 weeks for more responders. The prolonged duration of the effect of penetrating acupuncture is an important signpost of acupuncture’s salutogenic properties, meaning the ability to endogenously restore health in chronic pain patients.73,74 The findings that acupuncture not only reduced provoked vulvar pain and that it lasted longer in responders than for those receiving placebo is important. These RCT findings offer a viable treatment option for patients with vulvodynia.
No, they do not. The trial showed that acupuncture doesn’t work for vulvodynia. The authors point out that this study also didn’t have a no-acupuncture “usual care” group, which, I admit, would have been interesting, but all such a group would have provided was an estimate for the placebo effects evoked by the sham and “true” acupuncture needling.
Remember my usual saying when it comes to trials of acupuncture: “Inconclusive literature plus no plausible physiologic mechanism for acupuncture to work equal an ineffective treatment whose effects are nonspecific placebo effects.” The same is true at the individual study level, like this study. This study is, by the authors’ own admission, inconclusive, although, notably, this doesn’t stop the authors from calling for studies investigating the “effects among acupuncture responders and non-responders,” as well as for “larger, pragmatic trials.” Same as it ever was. Again, this study was negative. Yet Seifert swallows the narrative that this study was some sort of bombshell evidence that acupuncture really does work after all. (Take that, you nasty skeptics!) It most definitely isn’t. It’s yet another study that shows that acupuncture doesn’t work, but that also contains enough of a germ of a difference between the study and placebo groups to allow acupuncture advocates to spin it as supporting the use of acupuncture.
Closing the loop on the acupuncture narrative
Unsurprisingly, Seifert’s NatGeo article concludes that all this evidence, especially the new vulvodynia study, tells us that the ancient Chinese really must have been onto something. Never mind that how the Chinese did acupuncture thousands of years ago—or even 100 years ago—hardly resembles what passes for acupuncture now. None of that stops Seifert from credulously quoting acupuncture enthusiasts trotting out the same narratives as in the PNAS paper, such as touting how adopting acupuncture “could reshape how pain is treated globally—offering a low-cost, non-addictive option even as health systems search for alternatives to pharmaceuticals” and:
The results could be transformative. In the United States, where the opioid crisis has claimed more than a million lives since 2000, non-pharmacological approaches to pain management are gaining renewed attention. Some studies suggest acupuncture may reduce both postoperative pain and the need for opioid medications, though results vary.
I couldn’t resist laughing when I read “though results vary.” That phrase is doing a lot of heavy lifting. In any case, as I keep saying, it’s a script, and Seifert regurgitates a variant of that script quite unimaginatively. I also keep saying that, to believers in acupuncture and other alternative medicine, the opioid crisis represents an opportunity, and that’s why a reference to the opioid addiction crisis is always front and center in credulous propaganda about acupuncture. It’s all about more than that, though, as the script tells us:
As the evidence base grows, acupuncture may also serve as a gateway for broader acceptance of other traditional therapies, from herbal medicine to meditation—many of which are now studied with increasing clinical rigor.
Again, same as it ever was. Acupuncture is indeed a “gateway drug,” if you will, to the whole panoply of quackery that “integrative medicine” attempts to “integrate” into science-based medicine. Worse, as Seifert relates, the World Health Organization (WHO) is actively promoting TCM and other prescientific forms of medicine. Sadly, with our own Department of Health and Human Services, thanks to its takeover by antivax activist Robert F. Kennedy Jr. and his “make America healthy again” (MAHA) movement, look for variants of this script to be increasingly applied to spread from acupuncture to all manner of quackery promoted by MAHA.