{kind=link}
In today’s social media laden climate, it is de rigueur for people to instantaneously react and become simultaneously defensive and offended when any of our sacred cows are challenged. It’s part of the human condition and we can’t help ourselves. We dentists had the opportunity to feel assaulted a couple of weeks ago when an article in The Atlantic by Ferris Jabr entitled “The Truth About Dentistry: It’s much less scientific—and more prone to gratuitous procedures—than you may think” was published. Dentists worldwide were summarily outraged, and vast hordes of people who for some reason aren’t fond of dentists collectively pointed their virtual fingers at us and virtually screamed “AHA! WE KNEW IT!!”
So I suppose the purpose of this post is to “unpack” the article and attempt to objectively assess the claims put forth therein. Moreover, I would like to give a superficial overview of what science-based dentistry is, with some excellent links and other resources should you want to dive in further. I will try my best to not be too defensive and to lay out my case objectively. We’ll see how well I do.
The Atlantic article
I don’t want to spend a whole lot of time criticizing the parts of the article with which I disagreed; not only will that appear to be very defensive on my part (which, if you recall, I promised I’d try not to be), but primarily because it was covered really well in other posts by my friends and colleagues Dr. Alan Mead and Dr. Chip Payet. If you read their pieces, you’ll get a sense of how Mr. Jabr perhaps misrepresented the issue a bit in some areas. Dr. Payet really picks apart the positives and negatives about the article, and deftly explains why certain areas of dental research can be so difficult to undertake. Dr. Mead’s article addresses Mr. Jabr’s piece from a journalistic perspective – that it perhaps is a bit sensationalistic and hyperbolic, and framed in such a way to get a lot of ‘clicks’ which is the goal of many publications these days, even if accuracy and fairness are sacrificed in the process. As for me, I feel that it was a bit heavy handed and focused too much on the evil doings of one derelict unethical dentist who did horrible things to his patients – causing pain, costing them significant and unnecessary costs, and violating the sacred trust that all health care professionals strive to maintain with the people in their care. What that rogue criminal dentist did was tangential to the real question “How scientific is dentistry?”
Because I don’t want to leave all of the heavy lifting to Al and Chip, I’ll give a couple of examples of where Mr. Jabr went a bit overboard, resorting to a bit of fear mongering as well as simply getting a few things wrong. When he discussed one of “Dr. Evil’s” patients, he said “she was born with one tooth trapped inside another…” which isn’t really a thing in dentistry. I suspect that perhaps a tooth was congenitally missing in this case, or perhaps didn’t erupt properly and remained impacted. When a procedure was described thus: “He also chiseled out her bridge…” I have to smile a bit because most dentists I know rarely, if ever, use a chisel when doing fillings, crowns, and bridges. This, in my opinion, was simply the author’s way of casting an evil and greedy light on the procedures done by that evil and greedy dentist. To generalize from the one to the all is a bit disingenuous, and I say this with no offense taken and not being defensive.
I also bristled when the article stated:
A multitude of factors has conspired to create both the opportunity and the motive for widespread overtreatment in dentistry. In addition to dentistry’s seclusion from the greater medical community, its traditional emphasis on procedure rather than prevention, and its lack of rigorous self-evaluation, there are economic explanations.
This accusation paints all dentists as greedy and uncaring, who only want to do expensive treatment on their hapless, powerless victims. Contrary to his erroneous assertion, the emphasis in modern dentistry is on prevention, but keep in mind that we are not in control of our patients’ risk factors and lifestyle choices. To accuse us thus is akin to accusing cardiac surgeons of only being procedure-oriented and not preventive. Primary care physicians from cradle to grave, as well as specialists, ceaselessly attempt to educate their patients on preventive care – good diet, adequate sleep, exercise, not smoking, etc. But what their patients choose to do with that information is up to them. Those of us in the “body repair” business are simply there to try to pick up the pieces once the damage has been done. To paint us all as moneygrubbers who only do procedures if they’re profitable is a bit disingenuous and unfair.
That being said, Mr. Jabr does rightfully mention the science (or lack thereof) of the six month recall that is standard in dentistry. I wrote about that very subject last year, and while not scientifically rigorous, that doesn’t mean it’s wrong or that we are trying to mislead our patients. I wish he would have been “fair and balanced” in this area but again, his angle was to portray dentists as non-scientific greedy predators.
Dentistry and science
Is dentistry scientific? That’s the crux of this blog post and I hope I can lay out a solid case for the affirmative. I do believe that dentists are more than tooth carpenters and gum gardeners, and while Mr. Jabr points out that dentists only have four years of post-graduate education and training (unless one pursues a specialty), he failed to inform his readers about what our education entails. I won’t bore you with the details, but please indulge me while I bore you with the details.
- To be accepted to an accredited dental school in the United States (standards are similar in other countries), one must pass the Dental Admissions Test (DAT), which tests the applicant’s knowledge in such topics as biology, general chemistry, organic chemistry, reading comprehension, perceptual ability, and quantitative reasoning.
- While a Bachelor’s degree is not required, most dental students do have a Bachelor’s degree, usually in a science field such as biology or biochemistry.
- Once in dental school, our basic science education mirrors the training found in medical schools, encompassing anatomy, physiology, immunology, embryology, histology, pathology, pathophysiology, microbiology, biochemistry, neuroanatomy, and so on. In fact, when I was in dental school (University of Oklahoma), we took our basic science courses with the medical students. So I do think it’s fair to say that we have a decent scientific and medical foundation.
- In order to practice dentistry, we must pass a comprehensive board exam which reviews our knowledge in the basic sciences and dental topics, followed by completing work on live patients. To maintain our licenses, we must complete significant numbers of hours of continuing education each year.
Dental research in the 21st century is vast and varied, from improving the materials we use for fillings and crowns, to advances in technology, to Buck Rogers type stuff such as creating new teeth from stem cells, genetic testing and therapies, and other amazing biotechnologies. Yegane Guven wrote an excellent review on the scientific basis of dentistry, areas of current and future research, and how this is translated into dental education and practice.
Evidence-based dentistry
On this blog and elsewhere, distinctions have been made between the terms “evidence-based medicine (EBM)” vs. “science-based medicine (SBM).” The same differences and debates could be made in the realm of dentistry, but for us the term “evidence-based dentistry (EBD)” is more widely utilized, therefore I will be using EBD in this post with the understanding that I am applying the concepts and philosophies of SBM to the topic. The American Dental Association itself has an arm called The Center for Evidence Based Dentistry, which is an excellent resource for dentists and non-dentists alike. They host workshops and training for dentists and others in the dental field, helping us to apply the best scientific evidence into our clinical practices for the benefit of the patients we serve as well as the public at large.
According to the website, EBD can be defined as:
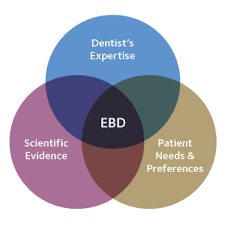
an approach to oral healthcare that requires the judicious integration of systematic assessments of clinically relevant scientific evidence, relating to the patient’s oral and medical condition and history, with the dentist’s clinical expertise and the patient’s treatment needs and preferences.
One of the best in depth discussions I have read on EBD is an article by Afrashtehfar and Assery, and for those of you who want to do a deeper dive on the subject, I highly recommend reading it.
This EBD triad of care encompasses the necessary components of what constitutes the standard of care for dentistry: the best scientific evidence, the needs and preferences of the patient, and the clinical expertise of the practitioner. If any aspect of this approach is violated (as it most certainly was in the Atlantic article), then the entire system of quality ethical care breaks down. An important point to make is that in medicine, dentistry, and every other area of health care, we rely on the “best available scientific evidence.” Science (including medicine and dentistry) progresses sequentially, in fits and starts, building upon previous knowledge. Therapies and procedures that are in use today may be overturned tomorrow if sufficient evidence dictates it. This is the strength, not a weakness, of the scientific process.
Conclusion: Maybe you’re defensive!
How did I do? Did I come across as offended or defensive? I really tried not to, but if I did, I apologize. What I do hope is that you, dear reader, have come away with a better understanding about the practice of dentistry as it takes its rightful place under the larger umbrella of Science Based Medicine.
What can you as a dental consumer do to ensure that you are receiving appropriate dental advice and treatment so that you don’t become a victim of an unethical practitioner like the dentist in the Atlantic article? The good news is that if you are a frequent reader of this blog, you are probably 99% of the way there. You have learned the tools of science and critical thinking and are able to apply them in your daily life. That being said, here are some other steps you can take:
- “Patient friendly” websites such as the Center for EBD (discussed above), the Cochrane Library, and PubMed are excellent places to research current evidence and guidelines in dentistry and other fields.
- Never hesitate to ask your dentist or hygienist to explain all of your options (including the option of no treatment at all), what the risks and benefits of a procedure are, all costs, and the experience and expertise of the provider. If you don’t understand the treatment, ask questions until you do. If you feel that you are being “sold” on any treatment, it is advisable to get a second (and maybe even third) opinion.
- Seek advice from objective science based dentists on social media, dental schools, or other platforms. We are always willing to help demystify dentistry and give general advice to people who contact us.
- Keep reading Science Based Medicine and other blogs who promote a science based worldview and foster critical thinking.
It was a tragedy that the dentist in The Atlantic article took such wanton advantage of his patients. Fortunately, situations like this don’t happen very often, but there are charlatans out there in all walks of life, so to arm oneself with the tools of critical thinking is one of the best defenses against such mistreatment in the dental office and elsewhere.