
{kind=link}

While ticks are responsible for spreading Lyme disease, there’s no evidence long-term antibiotics treat chronic Lyme disease, or do anything beneficial at all.
Lyme disease is a real and growing concern in much of North America. The spirochete Borellia burgdorferi was only discovered in 1982, and today, Lyme is the most common vector-borne disease in the United States. While Lyme disease is treatable, some people have prolonged or non-specific symptoms that they may attribute to Lyme disease, sometimes on the basis of nonstandard/unorthodox testing or diagnostic criteria. While the debilitating symptoms may be real, the relationship to Lyme disease is not. There is no evidence that “Chronic Lyme” exists, but there are repeated reports of signs and symptoms that are regularly attributed, incorrectly, to Lyme infections.
Along with the emergence of “Chronic Lyme” have been self-identified experts in treating these symptoms, often with a variety of unproven treatments, of which long-term antibiotic therapy is the most common recommendation. There is no evidence that long-term antibiotics are evidence-based, appropriate, or effective. Recently the Association of Medical Microbiology and Infectious Disease Canada has put out a position statement on the diagnosis and treatment of people with persistent symptoms attributed to Lyme disease. The position statement outlines why unproven, unorthodox treatments like long-term antibiotics are more likely to harm, rather than help, patients.
What is Lyme disease?
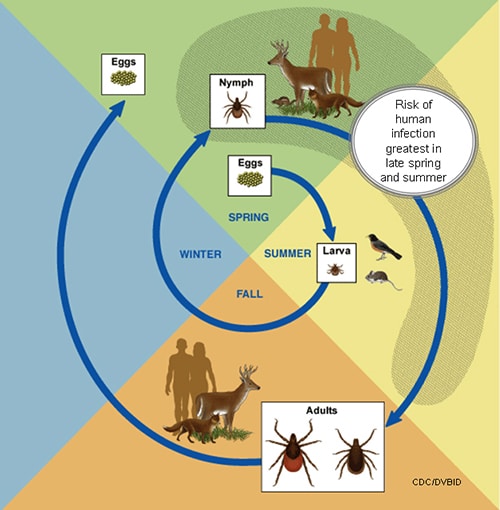
Lyme disease is a bacterial infection spread by ticks. Its name comes from Lyme, Connecticut, where a cluster of cases called “Lyme Arthritis” were reported in 1977. While it’s highly prevalent in New England, Lyme disease has been reported in every state, and its reach continues to grow. Several species of the Borrelia bacterial family have been found to cause Lyme disease, but B. burgdorferi is the primary cause in North America. Lyme disease is carried by various Ixodes ticks, which vary based on geography. Ticks contract B. burgdorferi from a blood meal from an infected host – usually a mouse, but it can be any rodent, and also birds. Infected ticks reside on shrubs or grass (peaking in June of each year), and will attach to mammals when they detect warmth and carbon dioxide. It’s preferably the white-tailed deer, but increasingly, a human. They can attach to any part of the body, but it is locations like the back, armpits and scalp where they may not be noticed for a few days – which is when infection can occur. This image from the CDC gives a good illustration of the circle of (a tick’s) life:
Ticks must be attached for 36-48 hours before a transmission of B. burgdorferi occurs. Infections can be divided into three phases:
- Early localized infection appears as a rash (often in the form of a series of concentric rings, or “bull’s eye rash”) and what feels like a viral illness (fatigue, headache, aches, and sometimes fever). It can occur in about 80% of those infected, usually within a month of infection.
- Early disseminated infection occurs weeks to months after the initial infection. It can include neurologic (e.g., meningitis), and cardiac complications. This may be the first sign of infection in some.
- Late disease occurs months to years after the initial infection. Arthritis is the most common sign, but there may be neurologic signs as well.
Lyme is diagnosed based on signs and symptoms, plus a history of possible exposure to ticks. Laboratory testing may also be used. Treatment of Lyme disease depends on when it was detected and how it has manifested. Treatment is usually weeks of antibiotics and other therapies when more serious complications are present. When treated early, Lyme responds well to antibiotics, and a full recovery can be expected.
Treating after treatment
Some people with Lyme disease report symptoms after treatment that are attributed to the infection (and some people with no history or signs of infection also report similar symptoms). There is no evidence to demonstrate that B. burgdorferi infections cause chronic occult infections after standard treatments endorsed by the Infectious Disease Society of America (IDSA), AMMI Canada, the CDC, or, in the UK, the National Institutes for Health and Care Excellence. The cause of these symptoms may not be clear, and may be non-specific (e.g., fatigue, pain, difficulty concentrating.) While it is important that these symptoms receive proper investigations, there is a lack of evidence supporting the use of long-term antibiotics.
Unorthodox and unproven testing and diagnostics are commonly used by practitioners to arrive at a diagnosis of “chronic Lyme”. The AMMI notes the following:
Concordant with the NICE guidelines (2018), AMMI Canada recommends that Lyme disease testing be done in accredited laboratories that participate in proficiency programs and use validated methods (“Validation should include published evidence on the test methodology, its relation to Lyme disease and independent reports of performance”) (NICE 2018). Given the high rate of false positive results (some as high as 50%) (Fallon et al, 2014), the use of laboratories that do not use FDA or Health Canada approved tests or use alternative interpretive criteria is not recommended.
Alternative and unproven testing methods are necessary to propagate the “chronic Lyme” diagnosis in order to explain away the negative results of conventional, established testing. As Steven Novella noted in 2017,
Patients with alleged chronic Lyme may have negative blood tests for Lyme, but that’s OK because the antibody titers and Western blot tests are not 100%. They may also not have all the classic symptoms of Lyme, but a long list of non-specific symptoms that do not point specifically at an infection or Lyme. They also are not cured by a single round of antibiotics, but that is because, it is argued, they have treatment-resistant strains of the Lyme spirochete.
In essence the argument is that chronic Lyme disease represents an atypical presentation of seronegative treatment-resistant Lyme. That is what we call special pleading – inventing a specific explanation for each instance of evidence (or lack of evidence) that would seem to falsify a hypothesis.
Long-term antibiotics do not benefit and may harm
In addition to the cost and ineffectiveness of long-term antibiotics, many patients experience adverse effects. The AMMI notes:
Well-designed studies have shown that long-term antibiotic treatment –beyond standard recommended treatment– is of no more benefit to the patient than a placebo, but caused significant adverse events in up to 26% of participants including Clostridioides difficile, intravenous catheter site infections (when intravenous catheters are used for medication delivery),and significant allergic reactions (Patel et al., 2000; Fallon et al., 2008; Holzbaueret al., 2010; Klempner et al., 2013; De Wilde et al., 2017; Marzec et al., 2017).
The AMMI points to a program at BC Women’s Hospital, the Complex Chronic Diseases Program, as a model approach to helping patients manage debilitating symptoms. That program offers group-based education, and self management support, in addition to medical consultation for myalgic encephalomyelitis/chronic fatigue syndrome, fibromyalgia, and symptoms attributed to chronic Lyme. They do not offer long-term antibiotics.
The AMMI has published a fact sheet on Lyme that answers common questions about the disease and its treatment.
Conclusion
People who believe they have “chronic Lyme” are suffering and deserve compassionate treatment. But giving medicine not based in evidence is magical thinking, not good science. Regrettably, practitioners that do believe they are treating “chronic Lyme” continue to propagate erroneous information and offer dubious treatments despite good evidence they are ineffective. Multiple organizations in Canada, the United States and worldwide caution against the indiscriminate use of intravenous antibiotics for the treatment of symptoms attributed to Lyme disease.