
{kind=link}

A black-legged tick responsible for spreading the bacteria that cause Lyme disease.
There’s significant and understandable concern about Lyme disease today. The spirochete Borellia burgdorferi was only discovered in 1982, and the disease only became reportable in the United States in 1991. Today, Lyme is the most common vector-borne disease in the United States (and Europe) with 25,000 cases being reported annually. Understandably, efforts have been growing to find ways to prevent Lyme disease, focusing on personal protection primarily, with environmental protection as a secondary measure. Some may recall that there was a vaccine on the market almost two decades ago, but it’s no longer marketed today. The story of the Lyme vaccine’s rise and fall is fascinating, and raises questions about whether there will ever be another Lyme vaccine marketed again.
What is Lyme disease?
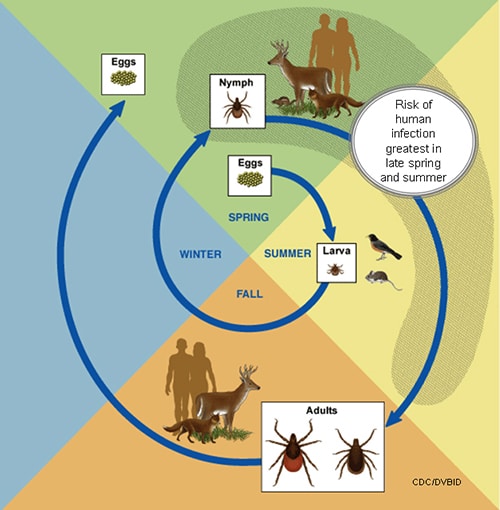
Lyme disease is a bacterial infection spread by ticks. Its name comes from Lyme, Connecticut, where a cluster of cases called “Lyme Arthritis” were reported in 1977. While it’s highly prevalent in New England, Lyme disease has been reported in every state, and its reach continues to grow. Several species of Borrelia have been found to cause Lyme disease, but B. burgdorferi is the primary cause in North America. Lyme disease is carried by various Ixodes ticks, which vary based on geography. Ticks contract B. burgdorferi from a blood meal of infected host – usually a mouse, but it can be any rodent, and also birds. Infected ticks reside on shrubs or grass (peaking in June of each year), and will attach to mammals when they detect warmth and carbon dioxide. It’s preferably the white-tailed deer, but increasingly, a human. They can attach to any part of the body, but it’s locations like the back, armpits and scalp where they may not be noticed for a few days – which is when infection can occur. This image from the CDC gives a good illustration of the circle of (a tick’s) life:
Ticks must be attached for 36-48 hours before a transmission of B. burgdorferi occurs. Infections can be divided into three phases:
- Early localized infection appears as a rash (often in the form of a series of concentric rings, or “bull’s eye rash”) and what feels like a viral illness (fatigue, headache, aches, and sometimes fever). It can occur in about 80% of those infected, usually within a month of infection.
- Early disseminated infection occurs weeks to months after the initial infection. It can include neurologic (e.g., meningitis), and cardiac complications. This may be the first sign of infection in some.
- Late disease occurs months to years after the initial infection. Arthritis is the most common sign, but there may be neurologic signs as well.
Lyme is diagnosed based on signs and symptoms, plus a history of possible exposure to ticks. Laboratory testing may also be used. While there are multiple reports of a condition termed “chronic Lyme” there is no persuasive evidence that “chronic Lyme” exists as a disease related to Lyme disease or its treatment. (More on “chronic Lyme” in the SBM archives.)
Treatment of Lyme disease depends on when it was detected and how it has manifested. Treatment is usually weeks of antibiotics and other therapies when more serious complications are present. When treated early, Lyme responds well to antibiotics, and a full recovery can normally be expected.
The origins of a vaccine
Given the growing incidence of Lyme disease over time, and the challenge in preventing bites, there was interest in developing a vaccine soon after Lyme was discovered. By the early 1980s, it was identified that most patients with Lyme disease had antibodies to a protein associated with B. burgdorferi, called the Outer Surface Protein (OspA). Antibodies against OspA were subsequently shown in animal models to protect against infection with Borellia burgdorferi. Two vaccines were eventually developed: LYMErix – by SmikeKline Beecham and ImuLyme by Pasteur Mérieux Connaught (ImuLyme was never submitted to the FDA for approval). How both vaccines worked was similar: They introduced antibodies in the body that would be ingested by the tick during a blood meal. The antibodies would then neutralize any B. burgdorferi spirochetes present in the tick, preventing any possible infection. LYMErix was a series of three vaccines at 0, 1, and 12 months. A 10,000-subject clinical trial established that LYMErix was generally well tolerated, with an calculated efficacy against symptomatic disease of approximately 76%, after all 3 doses were given.
Based on the efficacy data, LYMErix was approved in 1998. The Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC) recommended the vaccine for people that engaged in activities that resulted in frequent/prolonged exposure to tick-infested areas, where rates of Lyme disease was known to be high. It was not recommended to those with no to minimal exposure to tick-infested areas. Over the first few years, about 1.5 million doses were given.
While the vaccine did work, it was not without limitations. The biggest concern was efficacy: Over 20% of those vaccinated could still contract Lyme disease. And to achieve the 76% efficacy, one had to receive three vaccines given over a full year. Importantly, the vaccine was not tested in young children (the trial enrolled ages 15 to 70), one of the populations at risk of Lyme. And the vaccine did not provide protection against all strains of the disease – especially European forms of Lyme. There was also uncertainty about how long the effects would persist, and if boosters might be required annually.
Media-driven safety fears and the end of LYMErix
During its review the FDA noted the possibility that the vaccine could have a relationship with autoimmune arthritis. Given Lyme arthritis was influenced by immune factors, there was the hypothesis that the vaccine itself could conceivably cause arthritis in some individuals. While this hypothesis was just that – a hypothesis – there was some research in the area that never actually showed the vaccine could cause arthritis. Nor was there any clinical trial or post-marketing data to suggest it was occurring. This eventually moved from the scientific literature to the mass media with headlines like “Concerns Grow Over Reactions to Lyme Shots” in The New York Times around 2000. Growing coverage was also accompanied by the emergence of anti-Lyme-vaccine groups (e.g., Lyme Disease Network) who touted “vaccine victims”. Because the vaccine was not on the routine recommended vaccine schedule, the protections offered to manufacturers under the National Vaccine Injury Compensation Program (NVICP) did not apply. NVICP offers compensation to individuals injured by vaccines, and protects manufacturers from frivolous lawsuits. Because NVICP did not apply, class action lawsuits were launched against the manufacturer.
The FDA examined the safety of the vaccine in 2001. A panel concluded that there was no evidence of arthritis and vaccine based on available evidence, but encourage enrollment in a safety study of the product. Importantly no difference was found in the incidence of arthritis when comparing those that received the vaccine to those that did not. The vaccine adverse event reporting system (VAERS) was also examined for safety signals. In a paper eventually published in 2002, an analysis did not detect any specific safety signals that were not otherwise detected in the clinical trials. No arthritis.
By 2002, there seemed to be little appeal for a Lyme vaccine. Perhaps accelerated by the class-action lawsuits and the anti-vaccine lobby, the demand for the vaccine continue to drop. The manufacturer voluntarily discontinued sales of the product that year – it had been on the market for just 38 months. There was no evidence it caused arthritis, but dwindling sales (and the growing liability of lawsuits) led to its demise.
Is a vaccine possible again?
There are no vaccines available to prevent Lyme disease today in humans, and it seems unlikely (but not impossible) that one will appear anytime soon. There’s a lot of hurdles to overcome – not just regulatory hurdles, but public acceptance as well. Any pharmaceutical company will likely assess the risk of producing a new vaccine carefully, given its history and the persistent but unfounded belief that the vaccine was harmful. But given the growing incidence and regional spread of Lyme disease in North America, and a greater understanding of the harms it can cause, there is arguably a greater need for a vaccine today than ever before. And given we can vaccinate dogs against Lyme, perhaps we should be cautiously optimistic that the continued search for a vaccine may lead to its reappearance someday.