
{kind=link}
This will not be my typical Science-Based Medicine post.
What it is not
This will not be:
- About vaccines, diet, pseudoscience, quackery, or alternative medicine
- A critique of a questionable treatment, claim, or practice
- A skeptical evaluation of questionable evidence
- A book review
- A complaint about celebrities or the media
What it is
- Information about a diagnosis you may not have heard of
- Information about a strange set of positional maneuvers that can provide a seemingly miraculous cure with only one or a few treatments
- A review of the scientific evidence showing that the treatment is effective
- An example of how science works
- A cautionary tale
The diagnosis: Benign paroxysmal positional vertigo (BPPV)
Vertigo is a kind of dizziness where a person feels as if they or the objects around them are moving when they are not. Benign paroxysmal positional vertigo (BPPV) is one of the most common types of vertigo. It is an inner ear disorder that produces a spinning sensation with certain changes in the position of the head, such as rolling over in bed. The room seems to jerk repeatedly in the same direction. The episode typically lasts less than a minute; it is sometimes accompanied by nausea. It can be brought on by trauma, but a specific cause is usually not found. The incidence increases with age and it is more common in women. It sometimes resolves spontaneously but can recur.
The gold standard diagnostic test is the Dix-Hallpike maneuver where the examiner lowers the patient from a sitting to a supine position while keeping the head turned to the side and the neck extended. The test is positive if it reproduces the vertigo and produces nystagmus (repetitive jerking of the eyes). The estimated sensitivity (positive results in those who have BPPV) is 79% and the estimated specificity (negative results in those who don’t have it) is 75%, but those estimates are based on a single study with poor methodology.
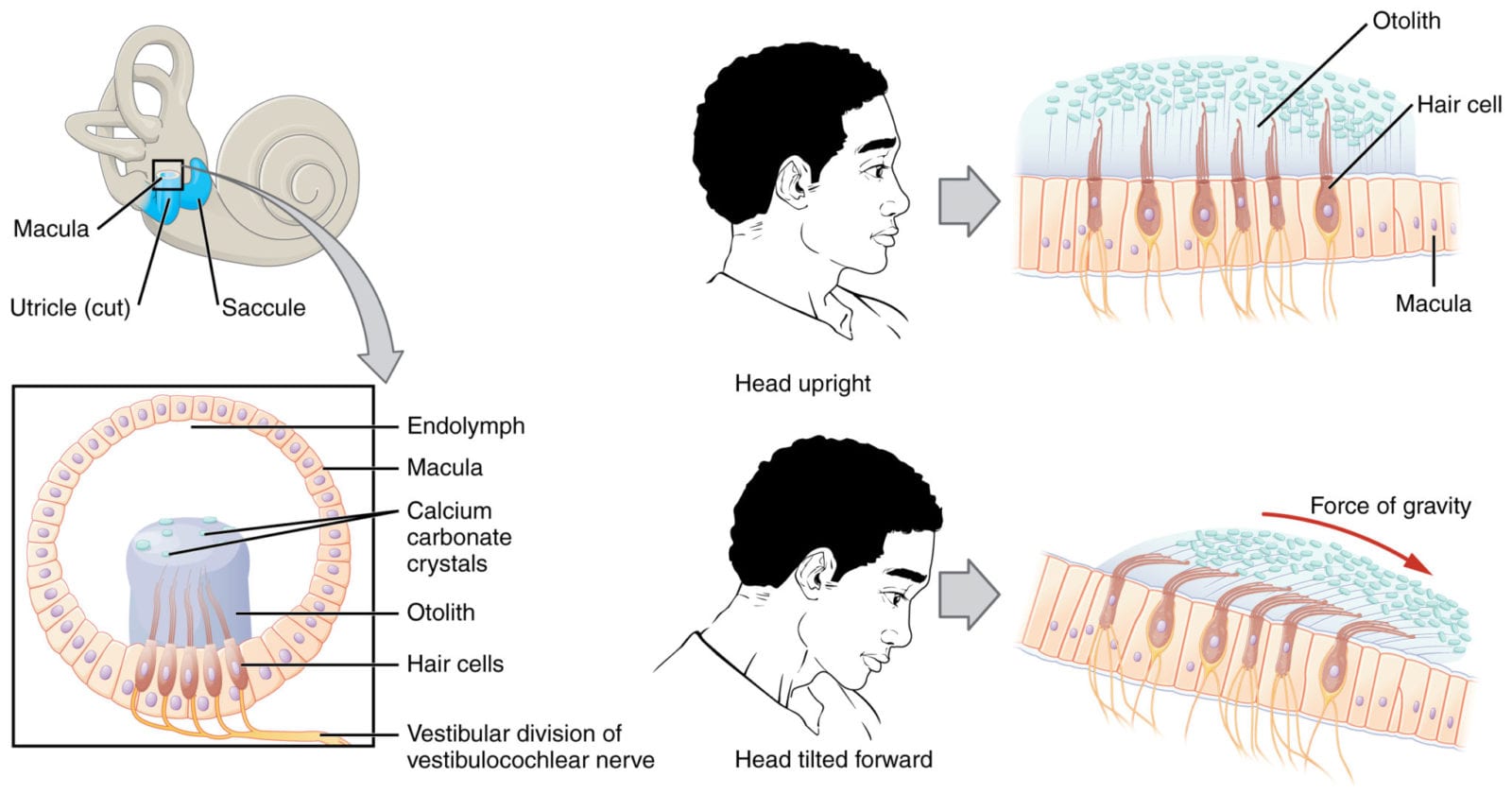
The symptoms are attributed to “ear rocks”, or otoliths, tiny crystals that are normally attached to the tips of hair cells where their inertia helps the inner ear sense gravity and movement. They can get dislodged and accumulate in the semicircular canals where they can trigger false signals of movement.
The treatment
There are four treatment options:
- Maneuvers by a clinician to reposition the otoliths in a “safe” area where they won’t cause symptoms
- Self-treatment with repositioning maneuvers at home
- No treatment (Not recommended; could lead to falls or other problems)
- Surgery (rarely used in severe recalcitrant cases)
The Epley maneuver
The best-known repositioning treatment is the Epley maneuver, which can be performed by clinicians or by patients themselves. It involves a sequence of positions: sitting with head rotated, lowering to a supine position with neck extended, turning head to the other side, rolling onto the shoulder, and returning to an upright position with head still rotated. It was first described by Epley in 1980; he also applied vibration to stir up the otoliths, but this later proved unnecessary. It is highly successful: it works (stops vertigo and nystagmus) in up to 95% of patients, and sometimes only a single treatment is needed.
The Epley maneuver has been extensively tested. Several systematic reviews have found it effective, including this one from 2006. A 2014 Cochrane review evaluated 11 randomized trials (7 of them blinded) with 745 subjects and determined that it was safe and effective. They thought there was a low risk of bias in the trials. The recurrence rate after treatment was 36%, but the treatment can be repeated. Follow-up measures to limit head movement, including sleeping with head elevated for 1-2 days, are commonly recommended; but a 2005 study found it made no significant difference. After a single Epley maneuver, there was clinical improvement in 96% of those who restricted head movements and 94% of those who didn’t.
Further thoughts
If I had heard about the Epley maneuver in 1980, before any of the studies had been published, I would have been very skeptical. The claim that a single set of positional maneuvers could cure a serious condition like BPPV sounds very improbable. It sounds like so many of those bogus “miracle cure” claims. It sounds more like voodoo than like science. Yes, there is a plausible mechanism, but quacks also think they have plausible mechanisms, like the memory of water to explain homeopathy. And there is no good direct objective evidence of otolith repositioning. But the published clinical evidence is very convincing: the Epley maneuver clearly works for BPPV. This is a good example of science at work. Science accepts good evidence of efficacy even in situations where the underlying mechanism is unclear. It rejects homeopathy not because of its implausibility alone, but because clinical trials do not establish efficacy. If homeopathy were as effective as the Epley maneuver or as penicillin, we might need to re-evaluate our conclusions. It isn’t, so we don’t. And please notice, this is a case of conventional mainstream medicine not relying on pills or surgery but using a simple hands-on procedure that costs nothing and won’t keep the patient coming back. A clear case of doing what’s best for the patient, not for the doctor’s finances.
And the story of the Epley maneuver is a cautionary tale. In 1980, skeptics might have written scathing opinions of what seemed to be a very unlikely treatment; and they would have been wrong. Rather than assuming that an untested treatment doesn’t work, good skeptics and good scientists will withhold judgment pending appropriate testing. Rather than being negative, we should limit ourselves to pointing out that without proper testing, we simply have no way of knowing whether a treatment works or not.
Conclusion: Epley maneuver is not voodoo
Science is really cool; it’s full of surprises. Sometimes what sounds like science turns out to be voodoo, as in the N-ray fiasco. Sometimes what sounds like voodoo turns out to be science. We must keep an open mind and wait for the evidence.
Vertigo Voodoo: A Crazy-Sounding Cure That Actually Works
A sequence of positional changes sounds like voodoo, but is actually an effective way to cure benign paroxysmal positional vertigo (BPPV).