
{kind=link}
As I sat down to write this post over the weekend, I was reminded of a scene from a 40 year old Arnold Schwarzenegger movie, Commando. You might remember that it was one of those 1980s hyperviolent movies (but, fortunately, mostly with cartoon violence) in which an impossibly strong and indestructible hero dispatches hordes of baddies in the service of, well, in this case rescuing his daughter from terrorist kidnappers. I don’t believe in spoiler alerts for movies that came out four decades ago, but let’s just say that the plot can be summarized thusly. Terrorists kidnap the daughter (Alyssa Milano) of John Matrix (Arnold Schwarzenegger), a retired Special Forces Colonel, in order to blackmail him into assassinating the leader of a South American country as part of a military coup by the former dictator whom Matrix had ousted. Matrix manages to escape, arm himself, and find his way to the island where the terrorists are holding his daughter, as many violent hijinks ensue. There, he single-handedly kills every terrorist and rescues his daughter. End of movie.
What reminded me of Commando as I sat down to write this was this scene, in which Matrix caught up with Sully, one of the former dictator’s henchmen who had put him on a plane to South America from which he escaped. Here, contrast what Matrix said to Sully early in the movie to what he said later:
“Remember how I promised I wasn’t going to write about ACIP or RFK Jr. again? I lied.”
You see, these two scenes remind me of my frequent promises to write about something other than vaccines, our Secretary of Health and Human Services Robert F. Kennedy Jr., or the destruction of the Centers for Disease Control and Prevention, Food & Drug Administration, and National Institutes of Health, most recently last week. Did I lie last week (again) about wanting to write about something else? No. I truly did (and do) want to write about something different. (Maybe a nice dubious homeopathy study, to cleanse the palate?) Unfortunately, the unending clown car that ACIP has become did not allow me to write about anything else. The truth is probably less that I lied when I said that and more that I probably deluded myself into thinking that nothing horrible would happen this week that would tempt or force me to break that pledge, even as I knew last week that the September meeting of the CDC Advisory Committee on Immunization Practices (ACIP) would occur on Thursday and Friday.
In retrospect, I was clearly deluding myself when I thought I could let this cup pass. Before I discuss the meeting in more detail, first I will say that the results of the meeting were not as bad as I had feared. For example, before the meeting started, I was convinced that the birth dose of the hepatitis B vaccine was going away; I had even predicted as much in last week’s post. Although the intent was clearly there to get rid of the routine birth dose of the vaccine and limit it just to infants born of mothers who test positive for hepatitis B, a combination of rank incompetence and buffoonery forced ACIP to put the vote on the vaccine recommendations off until the next meeting, as basically admitted by RFK Jr.’s allies. (Seriously, there was a discrepancy between ACIP recommendations not to recommend MMRV for children under four and continuing to recommend it for the Vaccines for Children program, attributed to a “technical error.” Sometimes, I think that ACIP’s being a clown car is the only thing stopping or slowing down RFK Jr.’s quest to rid America of all vaccines and wonder if he’s pissed off at how this meeting ended.)
Speaking of the rank buffoonery and incompetence of ACIP, here’s a reminder of who its members are:

I think the mood of ACIP was best summed up by this screenshot that I took from the beginning of the second day of the meeting during the roll call.
Another notable issue that I observed was how all the ACIP members declared that they had no conflicts of interest, even though Malone, Kulldorff, Pebsworth, etc. have financial and/or ideological conflicts of interest from their spreading antivax disinformation, Malone through his Substack, Pebsworth through being a board member for RFK Jr.’s old antivax organization Children’s Health Defense, and Kulldorff through his expert witness work for plaintiffs suing vaccine manufacturers.
Finally before I dig in, let me just say right up front that this will not be a comprehensive discussion of the most recent ACIP meeting. I was working both Thursday and Friday and unable to listen to the meeting live, even as background in my office or lab while I did other work. Finding 13 hours to listen to the entire thing this weekend was just not feasible. That is why I’m only going to concentrate mainly on one presentation as being the “best” of the bunch (and not very good) in order to give you an idea of the sort of questionable and dubious science that is being used to justify ACIP recommendations, even as I discuss more generally what happened and how it demonstrated rank incompetence. Concentrating on this one presentation also allows me to revisit an observation about how scientists who really should know better can be sucked into MAHA (“make America healthy again”) narratives and misinformation.
A familiar figure presents on COVID-19 vaccine safety
I’m going to start with COVID-19 vaccines, even though this discussion took up day two, mainly because of what I saw on social media on Saturday morning, posts from someone about whom I’ve written before, specifically his disappointing susceptibility to some bad antivax “science”:
Yes, it’s Prof. Wafik El-Deiry, whom we have met before in the context of his having demonstrated too little skepticism of work claiming that contaminating DNA from mRNA-based COVID-19 vaccines could integrate into genomic DNA and cause “turbo cancers,” to overinterpreting and overextrapolating results that his lab published linking binding of the spike protein to p53 (the granddaddy of tumor suppressor genes) to possible cancer development, to being willing to let his good name as a respected cancer researcher and director of a major cancer center be weaponized against vaccines by being interviewed by an antivax “journalist.” I’ve expressed my disappointment in Dr. El-Deiry on a number of occasions, as well as my admiration for his pre-COVID vaccine work, especially his groundbreaking work from the 1990s on another tumor suppressor, p21, which I cited often in my graduate work. I also found his responses to criticism to be…rather thin-skinned:
I’ll deal with this claim in a moment, but, really, Dr. El-Deiry is sadly…histrionic in this exchange:
and, incredibly, FBI Director Kash Patel!
In actuality, I thought I was being pretty reasonable and only just mildly snarky. But enough of Prof. El-Deiry’s intemperate statements on social media. Let’s get to his presentation. The video is here:
The PowerPoint slides for the presentation by Prof. El-Deiry and Dr. Charlotte Kuperwasser can be found here. (PowerPoint slides for all the presentations can be found here, if you’re interested.) Unfortunately, this presentation represents an official report of the results of the COVID-19 vaccine working group, of which Profs. El-Deiry and Kuperwasser are members. That is what is depressing. I expect antivax-sympathetic spin from the antivaxxers on the committee, like Levi Retsef. I don’t expect it from a cancer researcher whose work I had admired for many years before he went rogue.
Let’s just say that El-Deiry and Kuperwasser’s first slide didn’t fill me with optimism that this would be a rigorous science-based discussion:
I immediately recognized all four as common antivax tropes even before I watched the presentation. Now, let’s be clear that I’m not an immunologist, which is why I haven’t really discussed #1 very much and won’t discuss it that much here. (Unlike Profs. El-Deiry and Wasserman, I know my limitations. As a result, I try not to comment on areas that far outside my expertise and to be very clear about my limitations when discussing areas at the fringes of my expertise.
Even so, I do have to point out that the classic antivax misrepresenting of IgG4 class switching with repeated doses of COVID-19 vaccines is there, and I’ll refer you to an article like this one and note that the German man who got 200 COVID boosters in one year did not show evidence of excessive IgG4 activation or a damaged immune system.
#2 is an old one that I’ve discussed before but will discuss again here briefly.
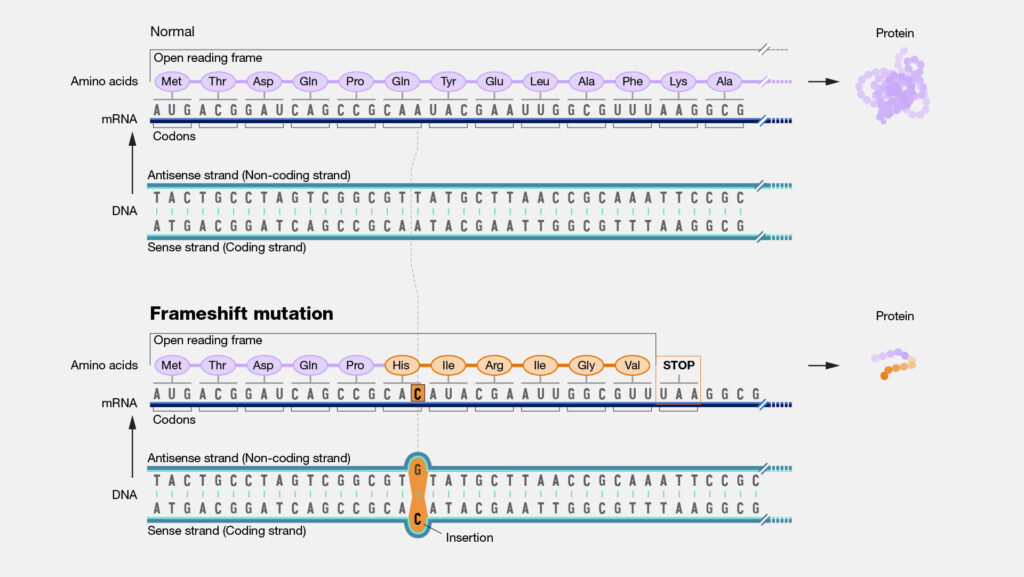
#3, the claim that there is so much more frameshifting due to the synthetically modified nature of the mRNA used in the vaccine is one that I’ve discussed in detail a couple of times dating back to 2023. You can refer to those posts linked right before this for (a lot) more detail. The CliffsNotes version is that the increased frameshifting due to the mRNA used results in a lot of “nonsense proteins” that stimulate the immune system and cause an off-target immune response resulting in autoimmunity or even cause the formation of prions. (Yes, seriously, prions.) Frame-shifting, in case you don’t remember, is an instance where the “frame” of three-nucleotide codons that the ribosome reads is shifted, usually as a result of an insertion or deletion mutation, although other things can cause a frameshift. Again, I discussed the concept in a lot of detail in the links. I also discussed how the claim that this increased frame shifting is somehow creating prions or “junk proteins” that stimulate the immune system and cause autoimmunity is utter nonsense. Prof. El-Deiry, a far better published molecular biologist than I, should have recognized it as nonsense, too, but for some reason did not.
Moving on, #4, of course, is the idea that DNA contamination, particularly with the dreaded SV40 enhancer sequence, results in plasmid DNA somehow getting into the nucleus and “integrating” with the genomic DNA there to cause cancer—or even “turbo cancer,” a meaningless term invented by antivaxxers, probably sometime in early 2022. Turbo cancer and the supposed “dangerous” DNA contamination is a topic that I’ve discussed more times than I can remember now (e.g., here and here). Little in this presentation is new, and none of it is compelling, as (I hope) you will see. Unsurprisingly, #4 took up more time than any of the other bullet points, because of course it did.
I’ve discussed the biodistribution studies before because, as you might recall, a Japanese bio distribution study was weaponized by antivaxxers less than six months after the vaccines had started to become widely available. During the committee, ACIP member Retsef Levi, chair of the COVID-19 vaccine working group, brought up this issue. You probably won’t be surprised to learn that the claim that there have been inadequate biodistribution studies or that existing biodistribution studies show that there is widespread distribution of the mRNA from the vaccine and persistent production of spike protein rely on studies in animals that inject massive amounts of mRNA relative to a vaccine-level dose. No less a scientist than Dr. Drew Weissman, co-recipient with Katalin Karikó of the 2023 Nobel Prize in Physiology and Medicine for their discoveries that enabled the creation of mRNA-based Covid-19 vaccines, was interviewed by STAT News and said:
What these people do, is that they search, they find one paper or two papers that make an outlandish claim based on bad data that hundreds or thousands or tens of thousands of other papers refute, they don’t mention everything that refutes it. They only mention, oh, look, I found a paper that says spike is around for nine months! It’s just not true.
Many good studies have not seen that. The RNA is gone in days. It doesn’t go to the brain. It doesn’t go to the eyes. What those studies did is they put huge doses of RNA into a mouse and used very sensitive assays, and that’s where it went. It goes everywhere. If you put a vaccine equivalent dose, you see it in the muscle, you see it in the draining lymph node, and that’s about it.
And:
I know it’s not distributed widely. I mean, we showed that back in 2017 at vaccine doses. We’ve looked at mice, we’ve looked at macaques, we’ve looked at rabbits, and we’ve done as much as we could on humans at a vaccine dose. You don’t see RNA circulating in the placenta, in the testes, in the heart, in the eye, in the brain, all the places that they list. We and many others have looked and we just don’t see it.
One of the papers cited, a preprint from Akiko Iwasaki’s group, is worth looking at. Weissman criticized it for using a supersensitive assay that isn’t that specific, and, if you look at the graphs, in particular Figure 5A, you’ll see that we are looking at femtomolar concentrations of spike protein—yes, femtomolar. To give you an idea of how tiny that is, that is one femtomole (10-15 mole) per liter. Much more typical protein concentrations with physiological significance are on the order of nanomolar (10-9 mole/L) to maybe picomolar (10-12 mole/L), in other words, several orders of magnitude more concentrated. In fairness, there are proteins active at femtomolar concentrations, and in COVID-19 infection spike can be detected at concentrations of around 50 pg/ml (picogram/milliliter), which translates to approximately 0.65 pM (picomolar), which would be 650 fM. Is what Isawaki detecting real? Is it biologically relevant? Let’s see.
One also notes that the preprint states:
Hence, we next sought to investigate whether the S1 subunit of the SARS-CoV-2 S protein could be detected in the plasma. For this, we used an anti-S1 Successive Proximity Extension Amplification Reaction (SPEAR) immunoassay. This method can detect S1 levels as low as 5.64 fM.
OK, that sounds like the lower limit of detectability. I note that this is how the authors used the assay:
Standard curves were generated from a stock solution S1 spike protein spanning from 0.0625 – 100,000 fM. Results from standard curves were used to generate sigmoidal four parameter logistic (4PL) fits in GraphPad Prism (v 10) software. Sample concentration results were calculated from run specific 4PL fit, multiplied by dilution factor. Lower limit of detection (LLoD) was calculated as the concentration corresponding to 2.5 standard deviation + mean zero in signal (18 replicates per run). Lower limit of quantification (LLoQ) was derived from the sample precision profile [measured concentration vs. concentration coefficient of variation (CV)] as the measured concentration at which a sample precision fit intersects at 20% concentration CV. The LLoQ and the LLoD values were calculated to be 20.5 fM and 5.64 fM as a mean of 6 runs. Values below LLoQ were replaced by the assay LLoD value and all values below LLoD were imputed as zero. The values were then transformed using the natural logarithm (ln(x + 1)) for comparisons. Analysis between groups was performed through a generalized regression model for zero inflation distribution (ZI Poisson) applying Tukey’s HSD to each pair.
So, basically, the authors found (if you believe them) that the lower limit of detection is 5.64 fM but that the lower limit of qualification (the lower limit for reliable quantification) was nearly four times that value. Yet, if you look at Figure 5, you’ll see lots of measurements that appear to fall at or near those values. I tend to be with Weissman here. Iwasaki is working near the limit of detection of the assay, as he pointed out a bit more bluntly:
What they reported was in the unknown area where it could just be noise in the assay versus real spike. Many other assays using good experiments, using good assays, don’t find spike protein circulating.
In fairness, Iwasaki’s study was part of the Yale LISTEN study of long COVID, which tends to pre-select for patients who have persistent symptoms after COVID-19 or COVID-19 vaccination, and the subject population was small (42 with “post vaccination syndrome” and 22 normal controls). Another thing that makes me wonder about this paper is that, seven months after it was published, it’s still a preprint and hasn’t been published in a peer-reviewed journal. Long delays between posting as a preprint and publication in a real journal always make me a bit suspicious about the quality of the science in the study, particularly when it comes from a well-funded lab with the resources to quickly address reviewer concerns with new experiments when called for. Basically, such delays make me wonder if the authors had tried to get this published in multiple journals, only to be rejected by each one.
The other favorite paper cited by El-Deiry is one that I hadn’t seen yet, as it was only recently published. It’s a paper by David Speicher, Jessica Rose, and Kevin McKernan. Regular readers will likely recognize at least two out of these three names, as both Jessica Rose and Kevin McKernan have garnered posts dedicated to them to discuss the specific COVID misinformation they spread, David Speicher less so. On first glance, this study appears to have most of the same problems that the first study by McKernan and Speicher that I discussed last year did, specifically that they used fluorometry instead of PCR to detect the DNA plasmid contamination:
Using fluorometry, total DNA in all vials tested exceeded the regulatory limit for residual DNA set by the Us Food & Drug administration (FDA) and the World Health Authorization (sic) (WHO) by 36–153-fold for Pfizer and 112–627-fold for Moderna after accounting for nonspecific binding to modRNA. When tested by qPCR, all Moderna vials were within the regulatory limit, but 2/6 Pfizer lots (3 vials) exceeded the regulatory limit for the sV40 promoter-enhancer-ori by 2-fold.
I discussed the problems with the fluorometry (Qubit fluorometry) the last time I discussed McKernan’s work. When the assay is used correctly, depending upon the specific fluorophore used, a scientist can distinguish between double-stranded DNA (like plasmid DNA), single-stranded DNA, and RNA. (mRNA is single-stranded.) This time around, Speicher et al looked at 32 vials representing 16 unique vaccine lots, as opposed to the last study, which looked at about the same number of vials, 27 vials over 12 lots, but they used basically the same methods. One thing that struck me is that this paper looked very similar to their last paper, with some of the same verbiage reused in the methods. If you look at Table 1, you’ll also see that 12/32 vials were expired and 4/32 were unsealed. Again, as I did last time, I have to wonder how many of these vials suffered mRNA degradation. Remember, DNA is a lot hardier than RNA. It degrades much more slowly in aqueous solution. In any event, in fairness, the authors did do what I ranted about their not doing in their last study and treated the specimens with RNase, which degrades RNA, presumably to leave only DNA. However, if there’s one thing I learned doing this sort of work, it’s that if there is a lot more RNA than DNA, even RNase-treated specimens will show a lot of RNA-associated fluorescents from the RNA fragments left after RNAse treatment.
I could go on and on, but let’s see the “money” figure:
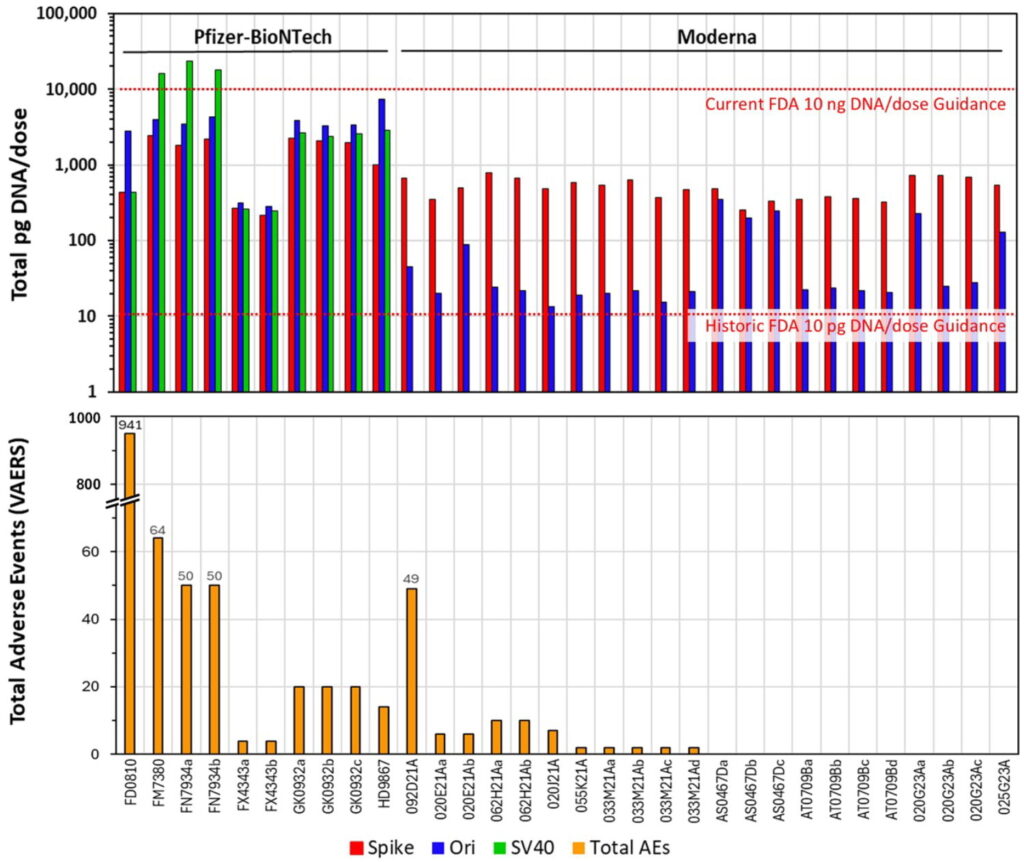
This graph made me laugh. First, it only shows three specimens that are supposedly over the WHO-recommended safety limit. Second, it’s graphed in log scale, which makes all the lower concentrations look a lot higher. 24 of the samples have DNA quantities less than one-tenth the WHO guideline. Moreover, notice Speicher et al pulling their same schtick of trying to correlate the DNA amount found in one vial from each lot to all the adverse events reported in the Vaccine Adverse Events Reporting System (VAERS). As a commenter on PubPeer noted:
Looking at the qPCR data in Table 3, there were 96 individual measurements made across 32 vials (three DNA targets per vial). Only 3 of those 96 measurements were above the 10 ng/dose limit, all from two Pfizer lots. Doesn’t this suggest that most vials were within the regulatory standards, and that the exceedances were limited cases?
And:
So the authors have presented the “<15% serious” description as though it were a regulatory upper limit for expected rates, when the VAERS guide itself warns that incidence or expected values cannot be calculated from VAERS data.
How can the authors justify treating a descriptive statistic (“less than 15%”) as a threshold for judging vaccine lots, given the clear VAERS guidance that the system does not support incidence or expected rate calculations? Ignoring these widely-known limitations of the VAERS database makes the analysis very dubious.
I’m not surprised to see this given the authors’ past publications, but I am surprised that a Taylor & Francis journal would still let this slip through in a paper in 2025.
Personally, I would go further. I would totally question the model validity of simply comparing DNA levels measured in one or two vials in a lot and trying to correlate it to the rates of adverse events reported in VAERS, given the potential of sampling error plus the fact that VAERS is a passive reporting system into which anyone can report anything, but that’s just me. The same commenter started going through the citations and references and—surprise! surprise!—found that many of them did not support the arguments being put forth. Meanwhile, another commenter noted (excuse the jargon, I’ll try to translate):
First, the manuscript misapplies the historical 10 ng/dose residual-DNA benchmark to Qubit fluorometry performed in an RNA-rich matrix. That benchmark was devised for validated DNA-specific assays on extracted material (e.g., qPCR/ddPCR within a process-validated control strategy), not for bulk fluorometry that is vulnerable to RNA carryover, RNA–DNA hybrids, and fragment-size–dependent bias—even after RNase. The headline claim in the abstract (“36–627× above the limit”) is therefore methodologically inapposite and regulatorily non-actionable. By contrast, the qPCR data—the only appropriate basis for that benchmark—show 96 measurements (32 vials × 3 targets) with only 3/96 exceeding 10 ng/dose, all for the SV40 promoter–enhancer–ori target in two Pfizer lots (≈ 16.06, 18.10, and 23.72 ng/dose), while all Moderna vials are SV40-negative and spike/ori remain below the threshold (Table 3). Elevating Qubit to a compliance arbiter while downplaying qPCR creates a specious impression of generalized non-conformity.
In other words, fluorometry can pick up residual degraded RNA even after treatment with RNase. I do like the last sentence, though, which, while dense, should be understandable by an educated layperson. The same commenter offers other technical criticisms that I find very compelling, but I will leave that as an exercise for the interested viewer with sufficient background in molecular biology to understand the criticisms. Sadly, a couple of weeks ago, Prof. El-Deiry seemed oblivious to this paper’s many flaws:
View on Threads
Susceptibility to antivax misinformation can blind even the best scientist, I guess. Note that this paper is being considered for retraction and now has a warning on the publisher’s website. Finally, let’s look at this particular slide:
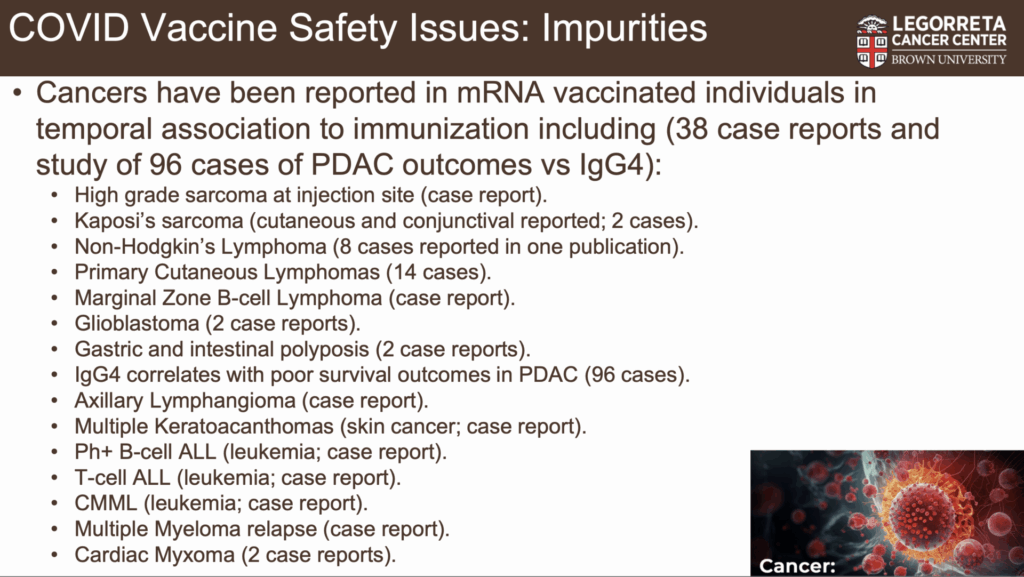
Now, Prof. El-Deiry’s talking! This is what I, as a surgical oncologist, have long wanted, the best evidence that can be presented for “turbo cancers.” Let’s just look at biological plausibility from long-known science about cancer and carcinogenesis. First of all, we know that the mRNA from the vaccine stays mainly in the injection site, although it can travel to the lymph nodes to which the injection site drains, in this case usually the axillary lymph nodes (under the arm). You might remember way back when the vaccines rolled out that enlarged lymph nodes after vaccination led to callbacks and sometimes lymph node biopsies after vaccinated women underwent mammography because the enlarged lymph nodes could look very similar to enlarged lymph nodes suspicious for metastatic breast cancer. What that should tell us is that, if the vaccine could truly cause cancer through integration of plasmid DNA contamination with the genomic DNA of human cells, then the vast majority of such cancers should be at the injection site, with the second most (a distant second) common arising from the axillary lymph nodes. Even if we concede that the vaccine components go elsewhere in the body, as a proportion of the total vaccine the amount depositing in other organs should be vanishingly small, making any cancers that might arise elsewhere vanishingly rare compared to at the vaccination site and (maybe) the regional draining lymph nodes. That doesn’t even count the observation that I’ve cited many times before that even strong carcinogens like ionizing radiation from the Hiroshima bomb takes a least a couple of years to produce blood cancers and a decade to produce other cancers, like colon cancer.
Now, look at the numbers and note that these are all case reports, not any sort of decent epidemiological study. Also note that there’s only one injection site sarcoma out of billions of doses of vaccine administered. Even if the vaccine did cause that sarcoma (unlikely) that would make the risk vanishingly small, one in many billions. Even if every single cancer (48 case reports, not 96, as Prof. El-Deiry mentions in his talk) in the list above could plausibly be deemed to have been caused by the vaccine (and the vast majority of them—if not all of them—cannot), it would still represent an incredibly tiny risk from the vaccine. Moreover, we know that cancer rates have not increased detectably since the rollout of the vaccine nearly five years ago. One might argue that, based on biology, it’s too early to see much of an increase, but, remember, antivaxxers claim that the cancers supposedly caused by the vaccine are a particularly nasty, aggressive lot, hence the made-up name “turbo cancers.” Also remember that Prof. El-Deiry once seemed quite receptive to the concept of vaccine-induced “turbo cancers.”
Let’s put it this way. If any of these cancers were shown to have arisen as the result of DNA coding for spike protein or SV40 promoter sequence integrating in genomic DNA in a location that could result in activation of an oncogene or the turning off of a tumor suppressor, you know that antivaxxers would be trumpeting it to high heaven and that Prof. El-Deiry would have included it prominently in his talk. I have yet to see a convincing example of a cancer in which an integration event from vaccine-associated plasmid DNA could be plausibly hypothesized to be the cause. And, yes, I’m aware of the preprint from antivaxxer Peter McCollough that claims to have found a perfect match between a genomic sequence taken from a highly aggressive bladder cancer in a 31-year-old woman and a 20 base pair stretch of the Pfizer vaccine nucleotide sequence coding for spike protein. My first reaction was: 20 bp? This is the best match anyone could come up with? Then I read further and saw that the woman was vaccinated with the Moderna vaccine, not Pfizer, and the discrepancy was handwaved away by saying that the “apparent paradox is best explained by shared Spike ORF sequences within the expression cassette across both vaccine platforms; because Moderna’s proprietary plasmid sequence has not been deposited in NCBI, BLAST defaults to Pfizer’s published reference as the nearest available match.”
If you believe the study, there’s only a one in 1012 chance of such a match, “making this alignment statistically compelling and highly unlikely to be an incidental artifact”; that is, if you believe the study, which I don’t. There were a few on X, the hellsite formerly known as Twitter, pushing back, too:
I would also say this. The description of the methodology in the paper is so lacking in detail that I wasn’t even entirely sure what these guys did. I did, however, notice that they didn’t appear to have controlled for multiple comparisons, a rookie mistake. Or maybe it was intentional and not rookie. Who knows? Actually, I can’t tell what the hell they did or what statistical test they used to come up with that figure of 10-12. Part of the reason I’m quoting al this was because, next up OdieuxEtVulgaire asked Grok. Now, I’m normally not a fan of relying on any sort of AI, especially Grok, for anything, but when even Grok slaps you down, well, it’s not good:
when Grok agrees that it is crap.
Seriously, Dr. McCullough. Hire a bioinformatics specialist or a statistician skilled in the methodology necessary to analyze big genomic datasets. Seriously, even I, a dumb surgeon with a PhD, know that a 20 bp match isn’t all that uncommon.
More than a day later, Prof. El-Deiry was still quite unhappy:
Note whom he is tagging: HHS Secretary RFK Jr., Robert Malone (who’s on ACIP), NIH Director Jay Bhattacharya, and FDA Commissioner Marty Makary. But that’s not all. He’s also tagging the antivax account JikkyLeaks, antivax “journalist” Maryanne Demasi (who interviewed him a couple of years ago about “turbo cancer”), and ScienceGuardians, which, if you look at its social media feeds, appears to be very much aligned with COVID contrarians.
He’s also very unhappy at criticism from Angela Rasmussen in her roundup of the ACIP meeting, which she labeled the Advisory Committee for Immunization Propaganda. Here he is:
Once again, he tagged many of the same people, including Levi Retsef, Robert Malone, RFK Jr., Marty Makary, and Jay Bhattacharya. (Seriously, his love of snitch-tagging MAHA leaders and antivaxxers has gotten really old.) In any event, you’ll note that Prof. El-Deiry is all-in on the “informed consent” trope that antivaxxers like to wield, which, as I like to say, boils down to misinformed refusal. When you harp on rare or likely nonexistent risks, using cherry-picked studies and studies by antivaxxers to do it, I’m sorry, you are promoting an antivax narrative, no matter how much you try to delude yourself that you are not. I would like to hope that Prof. El-Deiry is unaware of what he is doing, but he is copying a well-worn old antivax tactic of cloaking misinformation about vaccines in the rhetoric of “transparency” and “openness,” presenting himself as just an honest naïf who wants nothing more than to get at the “truth” by investigating further, even though much of what he is casting doubt upon has already been investigated to death.
You might ask why I spent so much time on just one presentation, when this meeting was such a—shall we say?—target-rich environment for someone like me. I suspect that it has something to do with just how disappointed that I am in Prof. El-Deiry. His transformation from a paragon of science research to a useful idiot for the antivaccine crowd has been truly eye-opening to me, to the point where I keep wondering if something could ever induce me to go down the same road. The worst part, however, is that, as bad as it was, Prof. El-Deiry’s presentation was was one of the least bad presentations at ACIP.
And all the rest…incompetence reigns
I said at the outset that before the meeting I was convinced that the birth dose of the hepatitis B vaccine would be going away. I was pleasantly surprised to be wrong about that, at least for now, although I am under no illusion that this was due to anything other than rank incompetence rather than lack of intent. Despite RFK Jr.’s having mentioned him in the foreword of his book on Anthony Fauci and chosen him to be on ACIP, Dr. Cody Meissner stood strong for the birth dose of hepatitis B vaccine, as described by Angela Rasmussen:
I do owe ACIP members Cody Meissner and Joseph Hibbeln an apology for characterizing them as anti-vaxxers in the past, when it is clear from yesterday’s meeting that they are not. While both have been anti-vax curious in the past, both asked very important questions during the discussion of HBV vaccines and pushed back against the absurd statement that trust should take precedence over evidence, which is clear for HBV: the universal birth dose of the vaccine has almost eliminated HBV from the US and 40 years of safety data shows that the rate of severe adverse effects is almost infinitesimally low. Meissner also provided critically important clinical context about the actual long-term risk of febrile seizures as well as key facts about pediatric HBV infection to completely destroy the notion that transmission is only sexual.
Also:
McMahon also told me that he sent a large data package to ACIP for consideration and has not received a response. This is consistent with the refusal of the current ACIP to assess vaccine safety and effectiveness using an evidence-based framework. Hibbeln seemed incredulous yesterday that the evidence for the HBV vaccine was being ignored, since anyone viewing the evidence in good faith cannot argue that the vaccine isn’t safe or effective.
Brian McMahon is Dr. Rasmussen’s uncle and a retired officer in the Public Health Service who still works part time treating patients in Alaska and researching hepatitis B, as he has done for 40. In addition:
In reality, Hibbeln’s entirely correct comments about how scientific processes should be carried out were ignored by most of the ACIP. Kulldorff sourly thanked him for his opinion and moved on, much as he did when expert liaisons repeatedly demanded that ACIP return to using its evidence-based framework for analyzing data and making recommendations. The CDC’s choice to share this quote outside of that context only serves to create the illusion that ACIP is using a scientifically-driven process rather than one motivated and serving ideological goals.
This ended up in ACIP voting to recommend that all pregnant mothers about to give birth be tested for hepatitis B, which is something the CDC has long recommended anyway. Then, the committee voted to table the vote on whether to delay the hepatitis B vaccine to one month. Reason prevailed, but from my perspective it was mainly because the antivax side couldn’t get its act together. When it came to this vote, you’ll see what I mean:
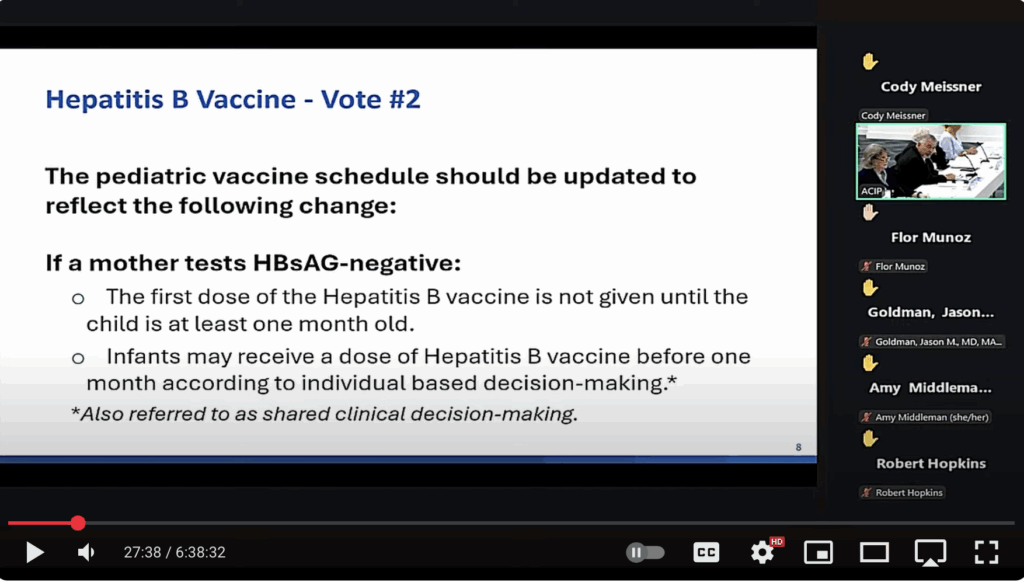
This is where Dr. Meissner put the kibosh on these incompetents. He pointed out that there is an inconsistency in the wording here:
I’m a strong advocate in clinical decisionmaking and I think that needs to be supported and in order to support that I believe that we need to clear up the question which as I read it has a logical inconsistency. The first part is that um it says the dose should not be given till the child is at one month old. And if that’s an absolute that it should not be given, then there’s no opportunity for clinical decision making. The second part says that there should be clinical decision- making. You can’t have it both ways. You can’t say it can’t be given and then say it can be given if there’s clinical decision making…It just it as it’s written now it’s a logical inconsistency. can’t say don’t give it and then give an opportunity to give it. So I think it should have some modification um is not given except except for the case of clinical decision-making.
The end result was that Dr. Meissner made a motion to postpone the vote indefinitely on the basis that a vote on Friday would be premature, and, to my surprise, he prevailed on that vote. Seriously, if the antivaxxers on ACIP had known what they were doing, they wouldn’t have produced recommendations to vote on that wouldn’t have been so ambiguous.
In another triumph for ACIP, the committee discovered something that’s been known for many years, that the MMRV (measles-mumps-rubella-varicella) vaccine results in an increased risk of febrile seizures compared to vaccination with MMR alone, something that’s been known for over two decades and something that ACIP has included in its reviews of the MMRV vaccine in 2005, in 2008, and in 2010. This led to a truly confusing set of votes. The first vote on whether the pediatric vaccine schedule should be updated so that it doesn’t recommend the MMRV vaccine for children under age 4 passed 7-4, with Malone abstaining because of his participation as an expert witness in a lawsuit against Merck. The second vote was on eligibility under the Vaccines for Children program (VFC), which covers the cost of vaccines for uninsured and underinsured children, to change the eligible group for the MMRV vaccine to children ages 4-12, which was rejected, with eight no votes, one in favor, and three abstentions.
Amid significant confusion expressed by some members of ACIP, who said they were not provided with the full text of what they were asked to vote on, the vote to approve the VFC proposal to change the eligible groups for the MMRV vaccine to children ages 4-12, was rejected, with 8 members voting no, one in favor, and three abstentions. Then, it got more confusing. As Politico reported,
The committee voted on Thursday to recommend that parents not vaccinate children younger than four with the combined measles, mumps, rubella and chickenpox vaccine, instead advising young children to get two separate shots: the MMR vaccine and an immunization for chickenpox.
But on Friday, the group reconsidered its Thursday vote that the combined MMRV shot for young children continue to be included in the Vaccines for Children program, a federal program that covers the cost of vaccines for millions of uninsured or underinsured children. The panel voted on Friday to overturn that decision in order to align the VFC guidelines with its recommendation that young kids get two separate vaccines for MMR and chickenpox.
Several members of the ACIP panel expressed confusion about the meaning of the initial VFC vote on Thursday.
Truly, the gang that couldn’t shoot straight. Also, Nature, which noted that the CDC had recommended that the V be separated from the MMRV for the first dose of MMR and V for a long time, observed:
Under the old guidelines, families could still opt for the single MMRV shot — for example, if they wanted to reduce the number of medical visits for their child. But the panel’s recommendation means that families will no longer have that choice, assuming the panel’s recommendations are approved by the acting CDC director.
ACIP member Cody Meissner, a paediatrics researcher at the Dartmouth Geisel School of Medicine in Lebanon, New Hampshire, opposed the decision. “What we’re saying is we don’t trust parents to make a decision,” he said. “Some parents don’t want to administer two doses of a vaccine if they can receive one and get the same degree of coverage. And I prefer that families have the option to make a selection.”
Remember, for antivaxxers, it’s choice for me but not for thee (if you are provaccine). To them “informed consent” and “shared decision-making” are only good if they result in not vaccinating.
Finally, what did ACIP decide about COVID-19 vaccines. This one had worried me too, given that there had been news reports that ACIP was considering restricting the vaccines to people 75 and older. Interestingly, the panel voted against advising states to require a prescription for COVID vaccines, the vote resulting in a tie broken by the chair, Martin Kulldorff. Of course, ACIP has no power over whether states require a prescription for the vaccine, but that didn’t stop them. Fortunately, this time, they fell short.
Their recommendations regarding the vaccine itself were also confusing. For instance, here are votes #3 and #4:
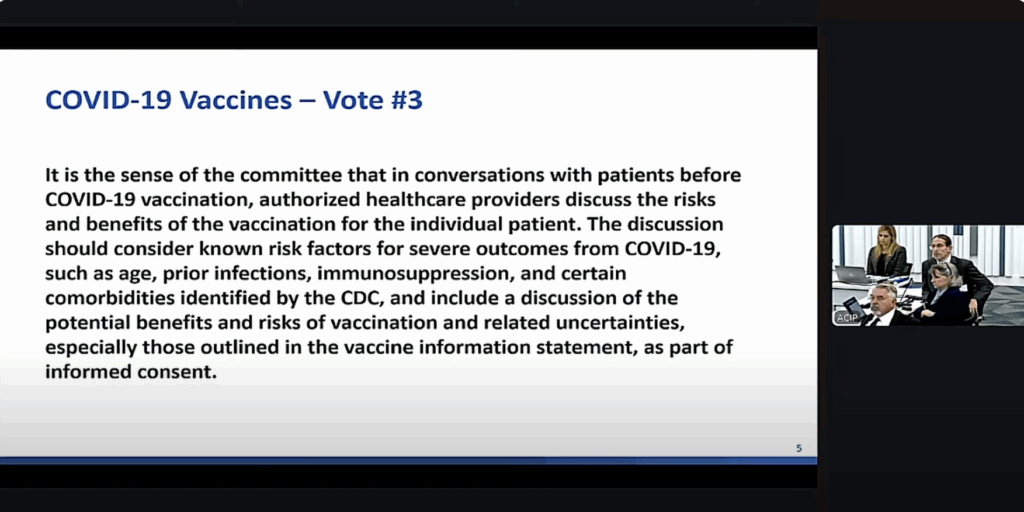
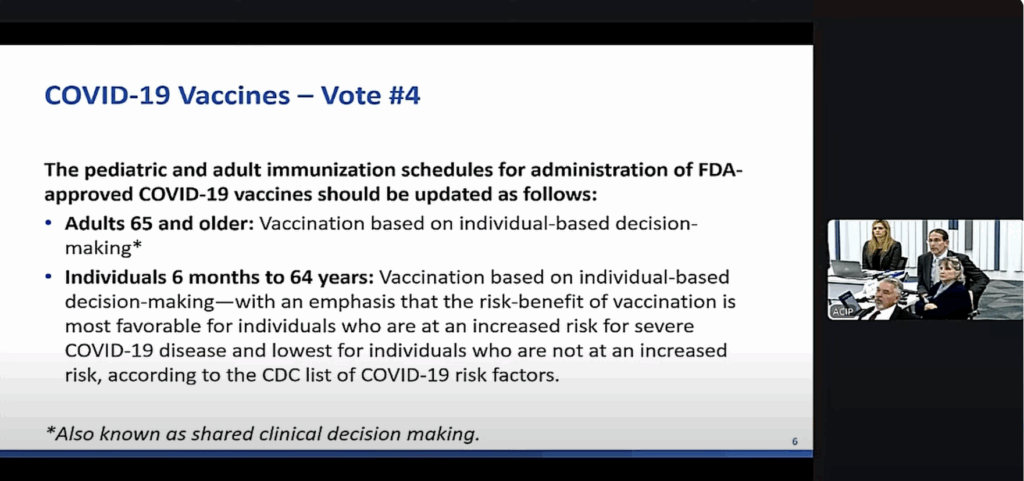
Both votes passed. Vote #3 tells doctors to do what they already do anyway, and one notes that patients receive a full vaccine information sheet that discusses these very things. Great going, there! Vote #4 means…I don’t know. Basically, it’s shifting from a broad recommendation that everyone over 65 should get the vaccine to saying something akin to telling seniors, “I guess you can get it if you want it and your doctor wants you to get it.” As for the rest of us under 65, it’s saying, in essence: “I guess you can get it if you want it and your doctor agrees, but you really don’t need it unless you’re really sick according to the CDC list of risk factors, and we really wish that you wouldn’t.”
Fortunately for me (and my fellow Michiganders), our public health leaders knew what to do. On September 19, our Chief Medical Executive was having none of ACIP’s nonsense and issued a standing recommendation:
Any person over the age of six months without contraindication who has not received a dose of a Food and Drug Administration (FDA)-approved or -authorized 2025-2026 COVID-19 vaccine may be considered to have an underlying condition that puts them at high risk for severe outcomes from COVID-19 and is thus eligible to receive an age-appropriate dose.
Sometimes, my state gets it right. Other states should follow suit.
Seriously, these guys are clueless newbies, and it showed. Indeed, at the introduction of the second day, Committee Chair Martin Kulldorff opined:
I think it was obvious to everybody who was listening that this committee has enormous depth and knowledge about vaccines about science uh about clinical experience taking care of patients uh about public health. There is one thing though in which we are rookies and, with one exception, this was either our first ACIP meeting or our second, and there are many technical issues that we might not grasp as of yet and after yesterday’s meeting I was approached by one of the members about the second vote we had yesterday about the VFC resolution on the MMRV vaccine that maybe we who thought that maybe didn’t quite understand what was going on.
Ya think? I was also highly amused by Kulldorff’s challenge near the beginning of the first day of deliberations to “debate me bro!” issued to the former CDC directors who had criticized RFK Jr. and the current ACIP. Sorry, dude. This isn’t one of your buddies’ podcasts, and the “challenge” was just plain cringeworthy. Other than Prof. El-Deiry’s presentation, I didn’t go into depth about any of the others, but I do feel that I should praise the career CDC staff who did presentations and tried so very hard to present a science-based perspective on the evidence to a clearly hostile committee. I also note that there was a lot more of the same and worse than Prof. El-Deiry, such as the presentation on COVID vaccine-induced myocarditis, which Angela Rasmussen correctly described as sharing “slide after slide of bullshit about myocarditis: falsely claiming with cherry-picked VAERS reports that myocarditis is much more common and dangerous than it is, presenting underpowered studies linking genetic variants to myocarditis, and eliding the fact that the myocarditis risk from mRNA vaccines is very small relative to the risk from having actual COVID-19.” I also loved how she described Cory Meissner’s takedown of Malone at one point:
He decided to pronounce that there is no such thing as a correlate of protection for COVID vaccines because T cells. Correlates of protection are essentially markers, like neutralizing antibody titers, that can be measured to assess whether a vaccine is protective or not.
I grabbed the popcorn when Meissner immediately went camera on and demanded Kulldorff allow him to respond. Meissner proceeded to eat Malone’s entire lunch in front of God and everyone, noting that while he agreed with Malone that correlates of protection are complex, some have been defined and cited this New England Journal of Medicine paper from 3 years ago. Embarrassing that the self-proclaimed inventor of mRNA vaccine technology (not true) didn’t bother to PubMed “correlates of protection COVID” while he was cashing in on his supposed vaccine expertise on the medical freedom influencer circuit! That didn’t stop him from also demanding that, in order to declare COVID vaccines truly safe, they’d have to prove a negative.
You get the idea of the chaos, and I haven’t even told you about the discussion segments.
In a post for Ars Technica entitled Bonkers CDC vaccine meeting ends with vote to keep COVID shot access (and it’s never good when reporters and commentators are referring to a CDC meeting as “bonkers), Beth Mole confirms that several liaisons from mainstream medical organizations stated that the ACIP committee needs to ditch such anecdotal nonsense and unvetted data and return to the high quality evidence-based framework that ACIP always used; that is, before RFK Jr. purged the committee and stacked it with antivaxxers. She also noted:
Retsef Levi, who works on operations management and has publicly said that COVID-19 vaccines should be removed from the market, responded by falsely claiming that there are no high-quality clinical trials to show vaccine safety, so calls to return to methodological rigor for policy making are hypocritical. “With all due respect, I just encourage all of us to be a little bit more humble,” Levi, who was the head of the ACIP’s COVID-19 working group, said.
During his response, a hot mic picked up someone saying, “You’re an idiot.” It’s unclear who the speaker was—or how many other people they were speaking for.
So say we all.
Fortunately, the end result of this ACIP meeting wasn’t as bad as I’d feared. True, there’s less choice regarding the MMRV, but the clowns in this clown car were too disorganized and incompetent to do what they had been expected to do and get rid of the birth dose of the hepatitis B vaccine. True, they downplayed the usefulness of COVID-19 vaccines, but they don’t appear to have decreased access further than they already have. Again, their recommendations are so vague and unlike what ACIP has recommended before that it isn’t even clear what they mean, and even multiple committee members stated that about some of the things they were asked to vote on. Meanwhile, remaining CDC career staff heroically tried to present actual scientific evidence to
Unfortunately, this was just one battle. Although the utter cluelessness of the clowns in the antivax clown car that ACIP has become, the war is far from over. For one thing, the recommendations have to be approved by the acting CDC Director and could easily be overruled or changed by the HHS Secretary. For another thing, I imagine that RFK Jr. is really embarrassed and pissed off by the spectacle of disorganization and incompetence that was this ACIP meeting. It changed nearly nothing and made close to zero progress towards his goal of eliminating all vaccines. It wouldn’t surprise me if he called up Kulldorff after the meeting and said, “WTF, Martin?” before tearing him a new one. That’s why I will conclude by warning that there will be another ACIP meeting near the end of October, and I fully expect Kulldorff, like the killer who appears to be killed at the end of a slasher movie, to return from the dead in the next installment to kill more teenagers. Unfortunately, he has slasher friends, and the teenagers are all of us.