
{kind=link}
[Editor’s note: Dr. Gorski has a grant deadline this week (tomorrow, actually). As a result, he’s reposting something from his not-so-super-secret other blog. Actually, he thinks it’s a sufficiently important topic that he regrets not posting it to SBM first. So, even though Dr. Gorski hates it when he has to skip a week posting new material on SBM, he is more than happy to remedy his previous error and post this on SBM. He’s also updated the post and added a bit of material to it. In any case, if you don’t read his not-so-super-secret other blog, it’s new to you, and even if you do this version is beefed up a bit.]
I’ve said many times before that there’s nothing new under the sun when it comes to the antivaccine movement. Basically, every antivax trope, lie, distortion, talking point, and bit of disinformation has been resurrected, dusted off, and repurposed to spread fear, uncertainty, and doubt (FUD) about the COVID-19 vaccines. As they’ve done since I first started, antivaxxers have blamed COVID-19 vaccines for death, infertility, and Alzheimer’s disease, while characterizing them as a sort of toxin-laden “gene therapy” that can “reprogram your DNA“. True, there is one antivax lie that hasn’t (yet) been resurrected for COVID-19, namely the claim that the vaccines cause autism, but that’s only because no COVID-19 vaccine has been approved or mandated for children. (You can bet that the vaccine-autism myth will reappear as soon as we start vaccinating children against COVID-19.) Even so, I now realize that I’m not entirely correct in saying that there is “nothing new under the sun” from antivaxxers about COVID-19 vaccines. Earlier this month, I came across one that I’d never heard before. Have you heard the one about the COVID-19 vaccine, lymph nodes, and mammography? I should have heard of it before, given that my surgical specialty is treating breast cancer, but, oddly enough, I hadn’t.
Before we see how antivaxxers are weaponizing this new observation, let’s start with the sane, sober, reality-based discussion of what I’m talking about, in this case from a CNN news report:
When she found a lump in her left breast during a routine self-check, Boston primary care physician Dr. Devon Quasha knew exactly what to do. She immediately scheduled a diagnostic mammogram and ultrasound at Massachusetts General Hospital for early January.
Then the Moderna vaccine became available to health care professionals in the city. She received her first Covid-19 shot about a week before her scheduled mammogram. Quasha didn’t notice much of a reaction to the vaccine at first, but a couple of days before her appointment her left arm began to hurt.
Tender, swollen lumps developed under her left armpit, along with a large swelling above her collarbone — all areas where there are lymph nodes, the body’s filters for germs. “You have lymph nodes above and below your collarbone,” Quasha said. “You don’t want to feel those. It was scary when I felt it.”
Lymph nodes contain immune cells that help fight invaders. That’s why it made sense to Quasha that the nodes were reacting to the vaccine, building antibodies as they were designed to do. But she couldn’t be sure.
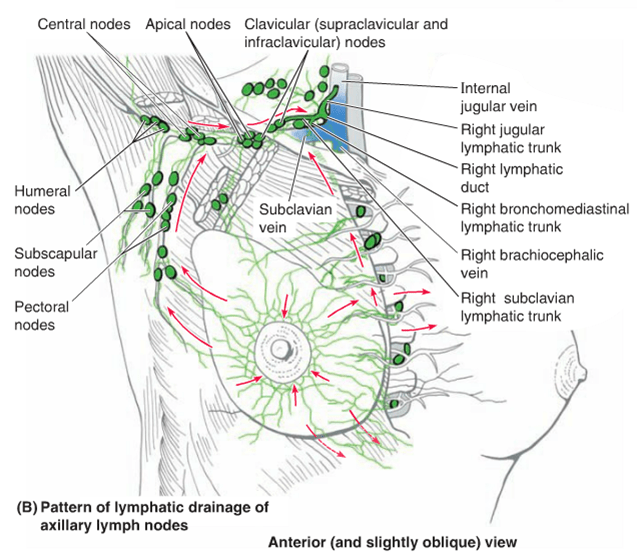
You can see how this might be alarming to women, particularly to a woman who had recently noticed a lump in her breast. To physicians and scientists, it’s no surprise at all that an injection that can cause local inflammation could also cause inflammation of the local lymph nodes, namely the axillary lymph nodes (the lymph nodes under your arm) or the supraclavicular lymph nodes (lymph nodes in your lower neck right above your collarbone). These two lymph node basins are where breast cancer often spreads first, particularly the axillary lymph nodes, which is why they are used in staging breast cancer, with positive lymph nodes imparting a higher cancer stage. Here’s an illustration:
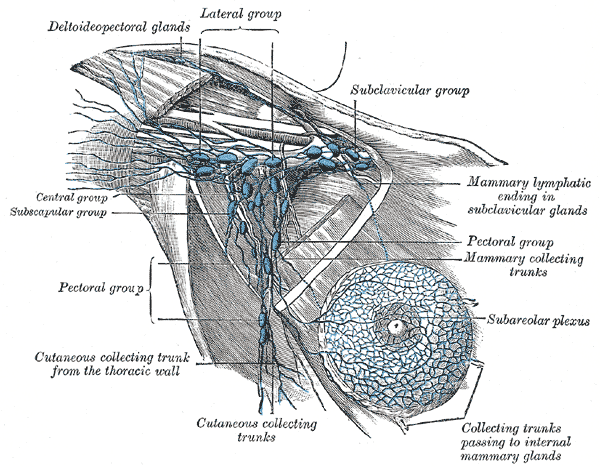
And here’s a more “anatomic” illustration:
Radiologists and breast cancer doctors have already encountered this phenomenon:
After the ultrasound, Quasha’s radiologist was concerned. She told Quasha she considered the lump she had felt in her breast to be of little significance, but the lymph nodes that showed up as white blobs on her mammogram were another matter.
In non-pandemic times, that finding would set off alarm bells, requiring the need for further investigation, even an immediate biopsy. Yet Quasha had just had the vaccine. After talking it over with her, Quasha said her doctor decided not to do a biopsy at that time. Instead she told Quasha to come back for a follow-up ultrasound in six weeks.
And this was the correct thing to do from a clinical standpoint. Other things that can cause lymphadenopathy (swollen lymph nodes) are injuries or infections in the arm, which can lead to an inflammatory reaction in the lymph nodes under that arm. That’s just the lymph nodes doing their job. For example, if bacteria get into the lymph vessels, the lymph nodes are a point at which the immune system can stop the bacteria from spreading further. In addition, any sort of significant (or sometimes even not-so-significant) inflammatory reaction can lead to lymphadenopathy in the lymph node basin draining the area where the inflammation is occurring.
It turns out, though, that axillary and supraclavicular lymphadenopathy on the side of the shoulder in which a woman received a COVID-19 vaccine is turning out to be more common than anticipated:
Similar scenarios had been happening in mammogram centers around the country. As radiologists compared notes with colleagues, word began to spread.
“We all started talking about it, and it was like a wildfire,” said Dr. Connie Lehman, chief of breast imaging in Massachusetts General’s department of radiology.
“I cannot tell you how many women are showing nodes on mammograms and people thought it was going to be not that common,” said Lehman, who is also a professor of radiology at Harvard Medical School.
Tales of unnecessary biopsies spurred the patient care committee of the Society of Breast Imaging (SBI) to put out an advisory in January: Ask your patients about their Covid-19 status, and record the date and which arm received the vaccine. Consider that before automatically scheduling a biopsy.
“We wanted to advocate that women don’t always need to have a biopsy,” said Dr. Lars Grimm, associate professor of radiology at Duke University School of Medicine and one of the authors of the SBI advisory. “Because oftentimes the default if you see swollen lymph nodes in a patient would actually be to recommend doing a biopsy.”
In a story in the Washington Post on Friday:
After vaccination, a swollen lymph node may appear as a lump in the armpit. These glands are hotbeds of immune activity, filtering pathogens and storing germ-fighting cells. If you’ve had a sore throat or a cold, there’s a chance you’ve felt a swollen node in your neck. The post-vaccine node may be palpable, too.
This side effect appears to be more common after the Moderna and Pfizer shots than after the Johnson & Johnson vaccine. In Moderna’s trials, about 1 in 6 recipients reported swelling or tenderness in armpit lymph nodes, often on the same side as the shot, after a second dose.
In the context of breast imaging, abnormally enlarged lymph nodes observed on mammography or axillary ultrasound are frequently of concern. Most commonly, they do not represent breast cancer, but they can. Depending on how suspicious the enlarged lymph nodes are, a core needle biopsy, guided by ultrasound, might be ordered. One can see how this sort of side effect of COVID-19 vaccines could wreak havoc with mammographic screening.
It’s also not as though vaccination by an intramuscular injection in the shoulder didn’t sometimes result in enlarged axillary lymph nodes before COVID-19. Anything that causes an inflammatory reaction in an upper extremity can lead to enlargement of the lymph nodes on that side of the body, and vaccination is no different. The difference with the COVID-19 vaccine is that there is a mass vaccination program going on, with tens of millions of women who are older (and thus undergoing routine screening mammography) receiving the shots. The law of large numbers thus dictates that, in that setting, radiologists are going to see a lot of women whose mammograms and/or breast and axillary ultrasounds detect enlarged lymph nodes after a COVID-19 vaccine. Before the COVID-19 mass vaccination program, the numbers of women who received a vaccine of any kind soon before undergoing mammography was much smaller than it is now. After all, the main vaccines adults over 50 receive include the shingles vaccine, a yearly influenza vaccine that many adults don’t bother with, maybe a Tdap if they haven’t received a tetanus vaccine in over ten years, and a vaccine against pneumococcal pneumonia recommended for those 65 and older.
Indeed, since I first started seeing this warning late last month, we’ve had several cases of women with enlarged axillary lymph nodes seen on mammography after COVID-19 vaccination right at my cancer center’s own breast center. We’ve even seen at least one in the context of a newly diagnosed cancer on the same side, a situation in which seeing enlarged lymph nodes is particularly concerning because, absent vaccination, such a finding can mean that the cancer is not stage I (no positive lymph nodes), but rather stage II or above, depending on the number of suspicious lymph nodes detected. This left the difficult question of whether to wait 4-6 weeks and repeat the ultrasound or to biopsy the lymph node(s) now.
So the SBI advisory to do mammograms either before receiving the COVID-19 vaccine or 4-6 weeks after the second dose of the vaccine is both a reasonable and practical response to this observation. So is the suggestion that axillary lymphadenopathy observed on mammography and/or ultrasound may not necessarily be immediately biopsied but instead followed up with repeat imaging in 4-12 weeks to make sure that the lymphadenopathy has resolved. Doctors involved in screening mammography and the evaluation of women for breast cancer (such as yours truly) make these sorts of clinical judgments all the time. COVID-19 vaccinations complicate these sorts of judgments, but, when you come right down to it, not by very much.
Indeed, some radiologists and breast cancer doctors have gone a step further, saying:
At Mass General, Lehman and her team have gone a step further. They are screening all women regardless of vaccine status, but telling those with no history of cancer that any swelling in the lymph nodes that might be connected to a Covid-19 vaccine is benign — meaning not cancerous.
“This follows the American College of Radiology recommendations that if you have a known inflammatory cause you can say it’s benign,” said Lehman, who recently published a paper on the hospital’s procedures.”
If their concern is a swelling or tenderness after the vaccine in their armpit, we suggest that they wait four to six weeks, talk to their doctor, and if it persists, then we have them come in to do an evaluation of it,” she said.
But how common is supraclavicular or axillary lymphadenopathy after COVID-19 vaccination? Going back to the SBI advisory:
For patients receiving the Moderna COVID-19 vaccine, axillary swelling or tenderness (i.e., lymphadenopathy) was a solicited adverse event reported in 11.6% of patients (vs 5.0% for placebo) following dose 1 and 16.0% of patients (vs 4.3% for placebo) following dose 2.(9) Furthermore, lymphadenopathy was also reported as an unsolicited adverse event in 1.1% of persons in the vaccine group (vs 0.6% in the placebo group). Lymphadenopathy occurred in the arm and neck 2-4 days following vaccination with a median duration of 1-2 days.
For patients receiving the Pfizer-BioNTech COVID-19 vaccine, lymphadenopathy was only reported as an unsolicited adverse event with 58 more cases in the vaccine group than the placebo group (64 vs 6 respectively).(10) Lymphadenopathy occurred in the arm and neck within 2-4 days of vaccination and lasted for a mean of 10 days. As lymphadenopathy was only reported as an unsolicited adverse event, the true incidence rate is likely higher. Reported rates and duration of adenopathy in both trials were based on clinical assessment (i.e., physical examination), and therefore rates and duration of subclinical adenopathy appreciable on mammography are likely greater. Anecdotally, mammographically detectable axillary adenopathy following COVID-19 vaccinations has been unilateral.
So basically the Moderna vaccine produced a significant incidence of axillary lymphadenopathy on the same side as vaccination in its phase 3 clinical trial, while the same adverse reaction was reported much less frequently after the Pfizer/BioNTech vaccine in its phase 3 clinical trial. No doubt the recommendations will change as we learn more.
So what are antivaxxers doing with this? (I did, after all, point out at the beginning of the post that antivaxxers were going wild with this.) Well, let’s head on over to that factory of unhinged conspiracy theories, antivaccine quackery, and quackery in general, Natural News:

Yes and no. As I explained above, yes, axillary lymphadenopathy can be a symptom of breast cancer. It can also be a symptom of lymphoma, lung cancer, and other cancers, or it can be a symptom of infection or inflammation. Of course, Mike Adams’ minion Lance D. Johnson can’t resist going on about “inflammation”. (I sometimes wonder if these other “authors” for Adams’ site are just pen names for the man orchestrating the nonsense, but on the other hand not even Mike Adams could churn out the sheer quantity of conspiracy mongering and quackery on his site all by himself.) Here’s what I mean:
The vaccines are not only causing an inflammatory response in the arm of recipients, as seen with most vaccines, but the shots are also causing systemic inflammation throughout women’s breast tissue. The doctors are concerned because the inflammation goes up with each vaccine dose. After the first dose of the Moderna vaccine, women, on average, have 11 percent swollen lymph nodes in their breast tissue. After the second dose, the inflammation increases to 16% of their lymph nodes in breast tissue. The Moderna vaccine is built on the experimental mRNA platform that metaphorically terraforms human cells so they can support foreign virus replication. The mRNA platform alters cellular processes, causing unpredictable inflammation as the immune cells respond to these newly developed virus properties.
Um, no. Axillary lymph nodes are not in breast tissue. In fact, there’s even a membrane/fascia separating the breast tissue from the axillary fat and lymph nodes. Indeed, when I’m operating, I know I’m in the axilla when I divide that membrane and the different-appearing axillary fat starts to pouch out. Yes, there are a few lymph nodes in the breast itself. We encounter them during surgery sometimes and sometimes they are noted on pathology reports after breast surgery, but that’s not what radiologists have been reporting. Also, the COVID-19 vaccine is “terraforming human cells”? That’s a new antivax metaphor. I’ve heard the bogus claims that these mRNA-based vaccines are “gene therapy, not vaccines” (they are vaccines), and that they “reprogram your DNA” (they don’t), but “terraforming human cells”? That’s one seriously overblown metaphor there, truly next-level antivax nonsense! Also, mRNA vaccines do not alter cells to “support foreign virus replication”. They do one thing. They provide the template for the cells into which the mRNA enters to make a single protein (the spike protein) from SARS-CoV-2, the coronavirus that causes COVID-19. That’s it. The immune system does the rest.
Of course, to Adams, it’s all a conspiracy, because, well, everything is:
In order to conceal the evidence of this widespread vaccine injury, the doctors are changing mammogram guidelines and refusing to screen the breast tissue of women who were recently vaccinated for covid-19. The doctors now advise all women patients to reschedule their yearly mammograms, either before the first dose or four weeks after the second dose. “We don’t want these patients to get a false positive to have this sort of alarm,” Parkinson said.
And:
The doctors pride themselves in “saving lives” through early detection of breast cancer, but when it comes to vaccine injury, the doctors turn a blind eye and delay the screening process. Obviously, women and the rest of society are being deceived about the origins of cancer and chronic disease. Women are being misled about the underlying causes of inflammation that create the conditions for breast cancer to develop. Vaccination initiates an inflammatory process. The experimental mRNA vaccines are designed to reprogram cellular functions, to create spike proteins that will create even more inflammation throughout the body. The fact that the doctors are willing to forgo breast cancer detection after a woman is vaccinated, shows just how far the medical establishment will go to cover up vaccine injury and the true origins of cancer.
No, it just goes to show that anything that confounds the results of a screening test is not a good thing. Moreover, delaying screening mammography a few weeks is unlikely to be harmful in the vast majority of women, while unnecessary biopsies of lymph nodes can be harmful. Of course, leave it to antivaxxers to come up with a way to link the observation that COVID-19 vaccination can cause enlarged lymph nodes under the arm to the common antivax trope that vaccines cause systemic inflammation that leads to autoimmune diseases, cancer, and neuroinflammatory diseases.
I was surprised to see someone push back against this nonsense in the comments, a commenter by the name Dr. Stan:
Dr Stan here, Ive been an Emergency Physician for 28 years. Spent 18 years in the US Navy as a Corpsman and Medical Corps Officer. Joshua, you are a moron. Concerning the vaccines causing breast inflammation, this is pure bullshit. Concerning immunizations in general, they have saved millions of lives world-wide. The number of childhood deaths are way down thanks to the HIB and meningitis vaccines alone. The Covid virus is concerning because it seems to kill healthy people for no good reason. The new vaccines may help, probably won’t hurt. All the reports of weird untoward reactions are mostly journalistic hype, anything to get people to read your articles. So Mike, I think you should stop scaring your viewers with your bullshit comments about the vaccines.
I would quibble with Dr. Stan when he says that the new COVID-19 vaccines only “may help.” No, they will definitely help. He is, however, correct about vaccines in general and that the claim that the COVID-19 vaccine causes “breast inflammation” is BS; it causes local inflammation that can result in enlargement of the local lymph node basis, where lymph nodes do what lymph nodes, being part of the immune system, do when they encounter lymph drainage from an area of inflammation. They enlarge and get ready to combat potential threats. In any event, the rest of the comments (e.g., “oncologists are merchants of death”) are what you would expect in the comment section of Natural News.
The bottom line is that, practically speaking, the observation that a vaccine injected into the shoulder can cause inflammation of local lymph nodes, such as lymph nodes under the arm or above the clavicle, is a big nothing burger. Doctors have noted the phenomenon and changed breast imaging guidelines in a cautious and reasonable manner to compensate. It is indeed very important to reassure women by explaining this phenomenon clearly, but that’s not what antivaxxers are out to do. They want to frighten women into thinking that this observed adverse event means that the vaccine is causing some sort of inflammation that is causing breast cancer. Unfortunately, I fully expect that, sooner or later, antivaxxers will start finding anecdotes of women who developed enlarged lymph nodes after COVID-19 vaccination and were found to have breast cancer.
It’s coming, just as the claim that COVID-19 vaccines cause autism will be coming, just as soon as a COVID-19—any COVID-19 vaccine—is approved for children and babies. That’s how antivaxxers roll, and always have rolled.