
{kind=link}
Last week, I thought that I might have been “scooped” by one of my fellow Science-Based Medicine bloggers when Scott Gavura wrote about DNA-based “personalized nutrition” advice. Before that, I had been seeing ads for such products, most commonly a company selling DNA test-based dietary recommendations known as GenoPalate, popping up in my Facebook feed. The ads and claims looked pretty dubious, and I made a mental note to look into the product. Then I saw Scott Gavura’s post. Fortunately, though, it was more of an overview of the sorts of products promising “personalized” diet recommendations based on genomic testing similar to that provided by companies like 23andMe and Ancestry.com. As such it was very useful, but I still had a lot of questions, and the more I looked the more I concluded that “direct-to-consumer” nutritional genomics (sometimes called nutrigenetics) testing currently has more in common with astrology than it does with science.
When examining a health product or treatment, I usually start by perusing the company website in order to see what the company is selling, the claims it’s making for its product or treatment, and the science (if any) used to support the claims made. So I wandered over to GenoPalate’s website. I was greeted with a splash page featuring a pretty young woman with an apple and the blurb, “Test your DNA to optimize your nutrition. Discover the best foods for your genes to eat healthier in 2020.” Here’s a screenshot:
Lower on the page:
Use your genes to find the best foods for you.
- Unlock the secret to healthy eating with a plan that’s personalized for you, based on your genetic profile.
- Discover your body’s ideal intake of carbohydrates, protein, fats, vitamins and minerals.
- Get a comprehensive list of the exact foods that match best with your genetic-based nutrition recommendations.
The company offers four products:
- Analysis of an existing 23andMe or AncestryDNA gene profile for $69 (on sale for $39 when I looked)
- Analysis of an existing 23andMe or AncestryDNA gene profile plus 5 recipes for $109 (on sale for $79)
- A DNA kit for $189 (on sale for $149)
- A DNA kit plus five recipes for $229 (on sale for $189)
The company claims for the full test and recipes:
- DNA Analysis in CLIA-certified lab
- Genetic needs for 23 nutrients
- The 85+ best foods for you
- Alcohol & caffeine metabolism rate
- Lactose & gluten sensitivity likelihood
- Delicious recipes based on your genes
- Mix and match breakfast, lunch, and dinner recipes
According to the company, the results of its test will lead to:
- “Enhanced Decision Making. Make smarter decisions at the grocery story, at your favorite restaurant, and while cooking meals for your family. Your GenoPalate Report empowers you with knowledge about how and what to eat based on your genes.”
- “Better Health.” Your path to health is unique.Understanding your genes and identifying the best way for you to eat helps you to make the healthiest choices for a strong and healthy body.”
- “Optimized Lifestyle. Everything you do is easier when you feel healthy. By personalizing your foods and eating habits you’ll have more energy, spend less time agonizing over which foods are right for you, and be more equipped to live a healthy lifestyle.”
Let’s dig in, because, as you can imagine, these claims are more marketing than science. I’ll use GenoPalate as the template because it happened to be the company whose ads keep annoying me by popping up in my Facebook and Twitter feeds. (Why, I have no idea. WTF, Twitter and Facebook?). Then I’ll conclude by looking more generally at direct-to-consumer (DTC) genetic tests that test various single nucleotide polymorphisms (SNPs) and use the results of published genome-wide association studies (GWAS) to make nutritional recommendations. There are a lot of these companies now, mainly because sequencing and SNP studies have become so inexpensive.
SNPS are the most common class of genetic variants and are represented by a single nucleotide change with respect to the reference sequence; i.e., the sequence as published by the Human Genome Project. For example, a cytosine (C) might be replaced by a thymine (T) at a given position in the genome. More than 600 million SNPs have been identified thus far in human populations around the world. Insertions and deletions (INDELs) are the second most common class of genetic variations. INDEL means that a person’s DNA sequence at a given position of the genome has more (insertions) or less (deletions) nucleotides with respect to the reference sequence. SNPs and INDELs, both clinically relevant as well as neutral genetic variants, are registered in a free public archive, the Single Nucleotide Polymorphism Database (dbSNP), while a specialized subset of dbSNP entries is collected in ClinVar, a freely available public archive of human genetic variants with proven or suspected clinical relevance. There are also GWAS databases, such as the GWAS Catalog (https://www.ebi.ac.uk/gwas/), which contains nearly 4,500 publications and over 177,000 associations.
Companies like GenoPalate use databases like these and combine them with published genome-wide association studies (GWAS) to construct models to use to calculate risk based on the genotype as determined by SNPs and INDELs. GWAS can identify genetic variants and, consequently, genes associated with disease risk and human quantitative traits, such as body mass index or blood levels of a metabolite, by finding associations between specific SNPs and INDELs and such traits. Such studies have a number of pitfalls, as I’ll discuss later.
Testimonials, testimonials, testimonials!
Let’s start with GenoPalate. You can imagine that my skeptical antennae started twitching fiercely as I read the claims quoted above. After every claim, all I could think of was: What’s the evidence? Not surprisingly, there was a page full of glowing testimonials about how GenoPalate supposedly helped various people eat healthier. Just like the case for alternative medicine clinics, when I see a company relying so heavily on testimonials to market a health-related product, I become extra skeptical. (The same is true for claims by pharmaceutical companies, in case you’re wondering.)
Particularly telling is this testimonial from a woman identified only as Debi, who has idiopathic hypertrophic subaortic stenosis (also known as hypertrophic obstructive cardiomyopathy), an inherited disease of the heart that causes thickening of the heart muscle and other changes to the heart that significantly impair its function. Apparently, in April last year, Debi was pretty sick. Her daughter had purchased a GenoPalate DNA test for her and her results arrived April 23, after which, as related by Debi, this happened:
I figured I just had to suck it up and deal with whatever was going on. I began my GenoPalate “substitution” program, but I didn’t put the entire plan into operation. I was also ignoring the parts about being genetically predisposed to type 2 diabetes. I was losing weight for the first time in decades, so I figured that I didn’t need the rest of the Report…I’d just keep substituting.Lone [sic] and behold, the month of May rolls around and all my doctors (mostly specialists) gave me a clean bill of health and yet, I was sick all of the time. As I was dealing with shortness of breath, I developed thrush (which is horrible). I’d just been put on a new inhaler to help the breathing and I thought that it gave me thrush. I stopped it immediately and, as it turns out, I do not have asthma.Everything that I was going through, except the IHSS, was food related. Here is how we found out:I tried to treat the thrush homeopathically. It would go away for a bit, but then come raging in. As I was trying to make up my mind if I should go to a doctor, my vision blurred to the point that I could barely see. I went to the eye doctor and she saw two clouds over my eyes and she thought they were my cataracts. I scheduled cataract surgery. The thrush kept getting worse so I went to my primary doctor and in no time at all, he is having a glucose test done on me and shooting me up with insulin. At 68 years old, I am learning that I have type 2 diabetes and the doctor is giving me all of these scripts. All I can think of is that at 68, my grandmother was diagnosed with type 2 diabetes and she died from complications after years of insulin. She had no life. She had nurses visit twice everyday to administer insulin to her. I want better than that for the remainder of my life. My uncle died of diabetes and my mother is suffering from diabetes related problems. Those are the thoughts going through my head.And then, I remember my GenoPalate Report. I planned to use the foods as my guidelines until I met with the nutritionist. I opened it and with fresh eyes, I saw all the warnings. I should have been eating the percentages that the Report recommended and I wasn’t, I was just substituting foods.Now, except that I eat chicken, which is not one of my “foods”, but fits in better for diabetic nutrition, I pretty much eat only what is in my GenoPalate Report. The food I don’t like, I just don’t eat it. With the Report and my nutritionists guidelines, I do believe that I can get my A1C down to an acceptable level and not need any kind of medications. About type 2, inflammation is a major cause. GenoPalate pointed out that I may have an intolerance to dairy and wheat. They were correct, I am allergic to both and have always eaten them because I was never “feeling” any side effects. I was so wrong. The side effects were internal inflammation, a contributing factor to weight gain and type 2 diabetes. Now I am dairy, wheat, and corn free….I do not miss them, at all.The long and the short of it and I guess the point that I am trying to make is: TAKE THE REPORT SERIOUSLY. Read it all! Don’t think about weight loss, think about healing your body from the inside and I do believe the weight will come off. I lost weight because the diabetes was trying to kill me, but I’ve keep it all of and maybe a pound or two more because I only eat what is in the GenoPalate recommendations (except for chicken).Your report is helping me…no joke.
Did the report help her, or did the nutritionist? Debi is apparently losing weight, and that can certainly help type II diabetics get keep their sugars under control and get their A1C down. A DNA test is not likely to tell anyone if they are allergic to dairy. For that, an allergist and skin testing is required. It’s also highly unlikely that Debi has either dairy allergy or lactose intolerance, given that she reports above never having felt any symptoms. Ditto wheat, which I presume is the test telling her that she might be allergic to gluten. Of course, there is such a thing, namely celiac disease, which is usually diagnosed with a blood test that measures the level of specific antibodies in the blood. A DNA test won’t diagnose it. Also, in the absence of gastrointestinal symptoms, it’s highly unlikely that Debi has celiac disease. As for non-celiac gluten sensitivity, as we’ve written many times before, it’s a condition that probably doesn’t exist (at the very least, it’s controversial whether it’s a real syndrome), although it’s a catch-all diagnosis that alternative medicine (and all too many “holistic”) practitioners love to invoke, and going “gluten-free” is not without potential harms.
As you can see, Debi’s testimonial, as is true for most testimonials for medical products, tells us little about whether GenoPalate has any value or can do what its manufacturer claims. The same is true of testimonials like this one by Amanda, who praises GenoPalate but has been going to an Orangetheory gym 5-6 days a week for a year and a half. No wonder she’s getting healthier. Did GenoPalate contribute? I suppose it might have if its recommendations are anything like the ones I encountered online, which are pretty generic.
Many of the recommendations that come from GenoPalate’s test are pretty unremarkable. For instance, in this testimonial video on the GenoPalate website, a man named Mike tells us that his GenoPalate profile suggested that he consume more foods high in complex carbohydrates and lower in fat and sugar. It also tells him that he should consume more dairy and chicken breast. With the possible exception of the recommendation to consume more dairy, these recommendations are not out of line with what a nutritionist would recommend; that is, unless Mike, who is obese, has type II diabetes, in which case a diet low in carbohydrates would be recommended:
Some of the recommendations get downright bizarre. For instance, the GenoPalate test recommended liverwurst specifically. It also recommended eel. Both of these were characterized as the foods that Mike’s body most needs. Mike, although puzzled by the specificity, loves it and automatically believes his report “because it’s from my genes.” Hey! If it’s your genes, it must be science, right? I mean, if a DNA test tells you that you should be eating elk and passion fruit, it’s got to be science, right?
Not so fast there, pardner.
A sample GenoPalate report
Curious what one of these reports looks like, I used a throwaway email address to sign up to download a sample report. It claims:
We analyzed your genetic variants (SNPs) that impact your nutrition. Below you will see the genes that these SNPs are located on, along with their associated genotype and prevalence. Your Genotype is your unique set of nucleotides that determines your nutrition recommendation. The Prevalence is the percentage of the population that has this genotype.
Your recommended macro- and micronutrient levels are based on the analysis of the most impactful nutrition SNPs. On the following pages, you will see examples of some of the SNPs we analyzed.
Your Recommendations are derived from research showing positive health outcomes associated with your genotype.
If you are recommended a high intake for a nutrient, we are suggesting you will benefit from consuming foods higher in that nutrient. If given a low recommendation, we are suggesting that you don’t need to consume as many foods that are high in that nutrient.
Basically, there is a huge assumption here, and the devil is in the details. That doesn’t stop GenoPalate from including strangely specific food recommendations in its sample report:
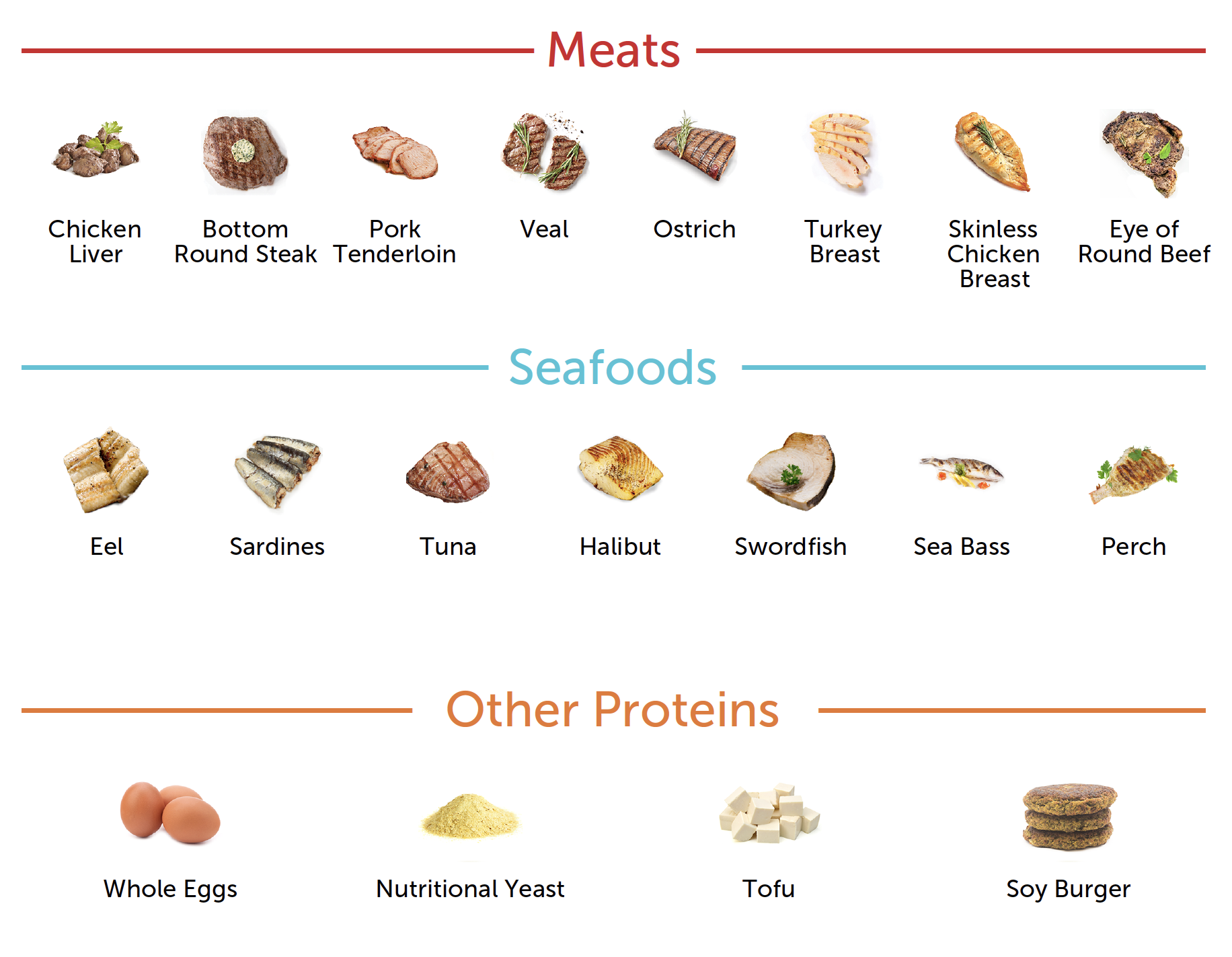
There’s the eel again!
The explanation:
Your top Meats were chosen based on your recommendations to consume High Folate, High Vitamin B6, High Vitamin A, and Low Sodium.
Your top Seafoods were chosen based on your recommendations to consume High Monounsaturated Fatty Acids, High Vitamin A, High Vitamin E, and High Zinc.
Your top Other Proteins were chosen based on your recommendations to consume High Vitamin D, High Monounsaturated Fatty Acids, High Folate, and High Vitamin A.
Well, OK.
What GenoPalate appears to be doing is what so many “cutting edge” consumer products based on genomics do. It’s extrapolating from existing research linking sets of single nucleotide polymorphisms (SNPs) in genome-wide association studies (GWAS) to various conditions. Of course, as we all know, the problems with existing research linking genetic markers to, well, almost any condition is conflicting. The results have been plagued with conflicting results, bias, and a lack of reproducibility, particularly for genetic epidemiological studies, which are in particular prone to false positives. Just ask John Ioannidis. Recommendations based on genotypes determined by analysis of SNPs are not reliable, at least not yet, and even interpreting the better studies can be fraught with difficulties. One example that comes to mind was described in this review article:
From an analysis of such data for an individual with Crohn’s disease, one might conclude that a deficiency of wheat products, dairy foods, red wine, corn, mushrooms, soy milk and yoghurt has led to the development of the disease. However, the actual picture is likely to be the complete converse of this. The observation is that, when he or she actually eats these dietary items, disease symptoms develop, and thus the individuals learn to avoid foods that trigger symptoms. This means that it is the presence rather than the absence of these items that actually led to the establishment of symptoms of the disease. This is the complete converse of traditional dietary interpretation, and may lead the way to different thinking about dietary studies in association with GWAS.
In another study, Ng et al noted that, although the agreement of the raw data is high in DTC genetic testing, the predictions vary depending on the company. Specifically, the investigators compared the predictions made by two different companies, 23andMe and Navigenics:
Even after we removed the average population risk variable we still found that only two-thirds of relative risk predictions qualitatively agree between 23andMe and Navigenics when averaged across our five individuals (see Table 1). Certain diseases have better prediction agreement than others. For four diseases, the prA major contributor to the discrepancies in disease-risk predictions is the set of markers that each service chooses to use in calculating relative risk. Risk markers are determined from genome-wide association studies, which survey hundreds of thousands or millions of markers across control and disease patients7. Each marker has different possible alleles. Alleles that occur more frequently in disease patients are designated as risk alleles and have odds ratios greater than 1. For example, in Alzheimer’s disease patients, 38% of ApoE alleles are the ApoE4 risk allele; this allele’s frequency is only 14% in normal controls8. The odds ratio for the ApoE4 risk allele is 3.7 (odds of exposure in cases, divided by odds of exposure in controls is (0.38/0.62)/(0.14/0.86)). The greater the frequency disparity between disease patients and normal controls, the higher the odds ratio associated with the allele. Conversely, alleles conferring protection against disease are observed less frequently in disease patients and have odds ratios less than 1.edictions between the two companies completely agree for all individuals. In contrast, for seven diseases, 50% or less of the predictions agree between the two companies across the individuals.
Basically, different DTC companies look at the published literature and choose which markers to include in their risk assessment profiles, and different companies choose different sets of markers. They will likely all include the strongest markers, the ones with the highest or lowest odds ratios, indicating strong or weak associations, respectively, but when they get into the weeds of markers that might not be so strong, often companies will choose different thresholds to denote a significant association. In fairness, Ng et al found high concordance with the risk of celiac disease, because there are known genetic associations with celiac disease. I would, of course, argue that a high risk of celiac disease is not a reason to avoid gluten, although it is a reason to seek a workup for celiac disease if symptoms consistent with it start to appear. Debi’s eliminating wheat from her diet, even if her GenoPalate test showed her at high risk for celiac disease, was not necessary and might have been potentially harmful in the absence of clinically diagnosed celiac disease.
Then, of course, there are a lot of markers for which there is a great deal of uncertainty in the odds ratios:
Another concern is the use of markers that have uncertain odds ratios estimates. A marker for type 2 diabetes that Navigenics uses has the highest odds ratio among all of Navigenics’ type 2 diabetes markers as reported in the literature. It therefore makes the strongest contribution to the overall disease prediction. However, Navigenics warns that the marker’s effect is statistically insignificant and may not contribute to disease. The average consumer is unlikely to appreciate the significance, or lack thereof, of this result.
In the end, Ng et al urged DTC companies to be transparent about which markers they were using, as well as about which studies they use to construct the models they use to calculate risk and traits. Nutrition and the various conditions and metabolic pathways impacted by it, are not simple monogenetic (one gene) traits, for which genotype analysis can often provide pretty good estimates of risk. They are very complex genetic traits, and it is for complex genetic traits that SNP analysis is most prone to being an unreliable predictor.
Those of you who clicked on the link have likely noticed that the paper by Ng et al is over ten years old. Its issues still resonate. Let’s look at more recent evidence, specifically a 2020 review by Floris et al of nutritional genomics and DTC companies.
Nutritional genomics: The current state of the industry
As I said before, there are a lot of these companies, their proliferation likely being due to the plummeting cost of DNA sequencing, SNP analysis, and genotyping, but also by the availability of a wealth of human genetic variation data. Add to this the Human Genome Project, carried out by the National Institutes of Health and the US Department of Energy provided researchers with the full sequence of the human genome, known as the “reference genome sequence.” Since 2003, this has allowed researchers to define and study differences in DNA sequence among individuals and what the functional consequences of those differences might be. The vast majority of these genetic differences are referred to as “neutral”, meaning that they have no detectable consequence or effect on health or risk of disease.
In the introduction, Floris et al note the problems with GWAS (alleles are different copies of the same gene, and I’ve added links to relevant explanations for genetic terms that you might not be familiar with):
Large sample sizes are required to accurately estimate the allelic frequencies and, consequently, to obtain a statistically robust finding. When a large number of genetic markers are tested in the same experiment, the results need to be corrected for multiple testing; for GWAS in particular, results are considered reliable when associations achieve an accepted genome-wide statistical significance threshold, conventionally represented by a p-value < 5 × 10−8. Despite the success of GWAS in identifying variant–trait associations and their application to clinical analysis, several limitations need to be taken into account when interpreting the results. One of the most relevant limitations is that, in each genetic region, multiple variants can be correlated (they are in “linkage disequilibrium”): on one hand, this facilitates the identification of the association but, on the other hand, makes it difficult to identify the “causal” variant(s), i.e., the variant effectively responsible for the signal. This means that the effective biological effect is unknown. Also, several studies have demonstrated that not only allele frequencies but also biological effects can be different in populations of distinct ancestries: this implies a further level of complexity in identifying the underlying biological mechanisms, which can be different for example in Europeans with respect to Asians or Africans [14].
More importantly:
When traits and diseases are highly heritable (i.e., monogenic traits and disorders determined by one or a few variants), genetic testing will be accurate and very predictive. In contrast, when traits and diseases are only partially influenced by genetic factors and the heritability is low, the predictive ability of tests that consider only a single genetic variant will never be very accurate [24,25]. Simply put, in case of complex traits and diseases, having a genetic variant will not mean developing a certain phenotype.
The complexity of these concepts means that a generic user does not have the tools to understand the truthfulness and reliability of these tests, unless direct-to-consumer genetic-testing (DTC-GT) companies declare in a transparent way the origin of the predictors used and the reliability of their advice.
Even then, only a scientist, particularly a geneticist or a scientist specializing in GWAS studies, would be likely to have the knowledge base to assess the reliability of the interpretation of a given genotype made by the DTC nutrigenomics company. None of that has stopped the industry from growing rapidly. Indeed, as Floris et al note, it’s estimated that the DTC nutrigenomics industry will grow to over $1 billion this year and reach $6 billion by 2028.
Floris et al, using various search strategies, identified 45 companies that offer DTC genetic testing in nutrigenetics, with 19 companies in North America, 21 companies in Europe, and the rest scattered over Asia, Australia, New Zealand, Central America, and Southern Africa. Four of the five companies are multinational, with multiple locations. Of these, 41 sold a DNA kit, either by online purchase or phone order. These companies claim to test for a wide variety of traits, including sensitivities to salt, alcohol, caffeine, sulfites, and various foods; lipid, carbohydrate, and protein metabolism; metabolism of various vitamins; and the like. The authors also found a wide variation in how the results were reported:
Reports provided by the companies are heterogeneous about content and representation of results. Most of the example documents (82%) are presented as personalized reports with name, surname and sample ID. Twelve companies (55%) provide information about genes and SNPs. Only four companies cite GWAS and polygenic score risk. Overall, results are first represented in a summary of all traits studied and of the genetic results (73%) followed by trait-by-trait sections, where consumers are provided with information about traits analyzed (77%), gene names and variants (82%) and a graphical representation of the genetic results (59%) indicating whether the genotype is favorable or not, along with the increased, low, moderate or typical risk. Genetic results are clearly explained (82%) with one or more sentences that explain the significance, followed by recommendations (86%). Only 10 companies provide a bibliography to support the reported information. Eleven companies state a disclaimer sentence, indicating that the information provided is not for diagnostic or clinical use, and suggest consulting with a healthcare professional before making any major changes to diet (Figure 3).
That last bit is what we in the biz call a quack Miranda warning, a term originally coined by a former contributor to SBM, Dr. Peter Lipson. It’s basically a dodge to get around the fact that the test is not approved by the FDA and a red flag that the results of a test are of unknown or low validity. Unsurprisingly, the GenoPalate sample report has just such a statement at the end:
The laboratory genetic testing was performed by GenoPalate, Inc. or one of its contracted labs. The information provided in this report is prepared by GenoPalate, Inc., and is based in part on publicly available databases. Neither the test nor the organization of this information have been cleared or approved by the FDA or any other government authority. Neither the test nor the information provided in any report are intended to diagnose any disease, and they are not intended to tell you anything about your current state of health or used to make medical decisions.
Nice. Why, then, would anyone want to bother to send GenoPalate up to $229 to have the company run its test and send food recommendations and possibly even recipes supposedly personally “tailored” to your genetic profile? More importantly, why does that statement not jibe with so many of the claims made on the website?
DTC nutrigenomics: Not ready for prime time
It’s very clear that DTC nutritional genomics of the sort of tests sold by GenoPalate and so many other companies is not yet ready for prime time, much less to use as a guide to make major changes in one’s diet. They’re not totally useless. For instance, as Floris et al note, they can pick up lactose intolerance and caffeine sensitivity, which are monogenic food-associated diseases, meaning that such tests are more reliable in predicting the phenotype based on the gene variations detected. The rest, however, are complex polygenic traits, for which predictions based on SNPs are much less reliable. Worse, even a scientist with the relevant expertise can’t necessarily assess the likely reliability of the company’s interpretations. The reason is this, according to Fortis et al:
However, the most outstanding fact is that only 16 companies out of 45 (about one third of the total) state which genes or which genetic variants are employed for nutrigenetic predictions. Moreover, only for 50% of the declared variants is an unambiguous code (in particular the dbSNP identifier) used. For this reason, for most companies it is difficult to understand exactly which genetic variants have been used to make predictions, and as a consequence it is very hard to interpret the reports and evaluate their scientific reliability.
In addition, of the 64 variants with the dbSNP identifier, only half of them are significantly associated at the genome-wide level with at least one trait of nutritional interest. This means that on average about 50% of genetic variants used for predictions show weak evidence of association with nutritional traits, and the chance that these variants might represent false signals of association is very high.
An interesting aspect is that predictions concerning traits for which dozens or hundreds of genetic associations (as in the case of body weight) are known, are made on the basis of few genetic variants.
I note that the sample GenoPalate report does list the genes used in its predictions, but I could not find dbSNP numbers. They way the report lists the “genotype” is simply to list the nucleotide substitution and the percentage of the population that has that particular genotype. That’s not nearly enough to assess the scientific reliability of its report.
These companies also use simplistic models:
Moreover, none of the companies exploit the use of powerful statistical tools such as polygenic risk scores (PRS, also known as risk profile scoring, genetic scoring, and genetic risk scoring). PRS combine multiple associated variants into a unique score by weighting their frequency in the population with their estimated impact on a trait [38]; they can be constructed for any complex genetic phenotype for which appropriate GWAS (or other robust association) results are available. PRS for susceptibility are promising tools to identify individuals at high risk who may be eligible for protective interventions, and their application could lead to more reliable information for consumers [24,25].
It’s much simpler just to look at individual SNPs and genes, rather than to go through the time and expense of constructing a PRS for each complex trait being assessed and predicted.
The bottom line is simple. DTC nutrigenomic profiling is just not ready for prime time, not as a prescription service and certainly not as a DTC service. Examples abound of how often the results are, to put it bluntly, wrong, such as when a DTC test predicted a peanut allergy in a woman who describes peanut butter as “one of the true loves of my life.” The test also stated that she was “less easily depressed.” Guess what? This woman had been diagnosed with clinical depression and treated for it. Basically, these tests promise information from your DNA with a granularity that is not possible based on our current knowledge of genomics. It’s not for nothing that scientists basically dismiss these tests as being in essence no better than horoscope readings. That’s an observation that applies to all DTC genomic profiling tests, some of which claim to be able to predict traits such as sexual orientation, “loneliness,” and “social communication problems,” not just to GenoPlate and the many similar DTC nutrigenomic profiling tests offered by competitors. Save your money, and if you need dietary recommendations seek out a registered dietician.