{kind=link}
There are many harms attributable to the antivaccine movement and its promotion of antivaccine beliefs. Certainly, the harm those of us who have been combatting antivaccine misinformation fear is the return of vaccine-preventable diseases, which is something we’ve seen in the form of outbreaks, such as the Disneyland measles outbreak two years ago and, in my own state, pertussis outbreaks. The Disneyland outbreak was a wake-up call to California legislators, who in its wake passed SB 277, a law that eliminated personal belief exemptions (PBEs) to school vaccine requirements. Now, only medical exemptions are permitted, and so far the law has worked well. In Michigan, we’re still struggling. The Michigan Department of Health and Human Services issued a new rule that requires parents seeking a PBE to attend an education and counseling session at a local county health office before the PBE is issued. Not surprisingly, local antivaxers are not happy and have managed, by painting this rule as a horrific affront to “freedom” and “parental rights,” to persuade legislators to try to pass a law that would not only revoke the rule and explicitly bar MDHHS from issuing similar rules in the future, but it would prevent local health officers from barring unvaccinated children from school during an outbreak. The law failed to pass the first time it was introduced, but Michigan legislators are nothing if not extremely persistent in pursuing harmful policies, and a new version of the same old bill is again under consideration. It matters not one whit to our stupid legislators that the rule change is starting to work to increase vaccine uptake. Unfortunately, we have a fair number of antivaccine and antivaccine-sympathetic legislators.
Although the antivaccine movement in the US has classically been associated with upper middle class and affluent white people, they are not the ones who are likely to suffer the most when herd immunity breaks down. I’ve written extensively here about how the newest (and perhaps most pernicious) antivaccine conspiracy theory, the so-called “CDC whistleblower” conspiracy theory promoted by Del Bigtree and Andrew Wakefield’s propaganda film disguised as a documentary VAXXED, explicitly targets the African-American community, complete with promotional visits featuring the Nation of Islam going to speak in Compton and being involved in protests outside the CDC. Wakefield, as you recall, is the British gastroenterologist who in 1998 published a case series in The Lancet linking MMR to autism. It has since been retracted and shown to have been fraudulent, and Wakefield has had his UK medical license stripped from him. Unfortunately, that only makes him more of a hero to the antivaccine movement, and he’s spent the last 19 years playing that role to the hilt.
The “CDC whistleblower” conspiracy theory is based on the story of CDC scientist William Thompson, who in 2013 apparently contacted biochemical engineer turned incompetent antivaccine epidemiologist Brian Hooker to vent about a study he co-authored in 2004 that examined whether there was a correlation between vaccination with MMR and subsequent risk of autism. Not surprisingly, the study failed to find a correlation. However, there was one subgroup, African-American boys, in which the unadjusted data showed a 3.4-fold increased risk of autism. (I’m simplifying for space considerations in providing background, obviously; if you want the gory details, read here and here for a contemporaneous account of the origin of a new conspiracy theory, as well as my review of the book Vaccine Whistleblower and Andrew Wakefield’s fraudumentary VAXXED.) Thompson had had disagreements with how the data were presented and how he thought the CDC has “suppressed” the unadjusted data. Unfortunately for him, Thompson didn’t realize that Hooker was recording their conversations, and Andrew Wakefield found out about it. Thus, he became the “CDC whistleblower” who seemingly validated what I like to call the central conspiracy theory of the antivaccine movement, specifically that the CDC “knows” that vaccines cause autism but covered it up. It didn’t matter one whit that the correlation was found only in a small subgroup (African-American boys), but it did matter because African-Americans already have reason to distrust the medical community based on history. The “CDC whistleblower” myth feeds into that sad history, which is why Wakefield loves to invoke the Tuskegee syphilis experiment.
This is also not the first time Andrew Wakefield has targeted people of color with his pseudoscience. By any objective measure, for the most part the CDC whistleblower conspiracy theory and VAXXED have not had much resonance in the African-American community other than in the Nation of Islam and among a handful of parents like Sheila Ealey who really believe vaccines caused their children’s autism. The first time around, unfortunately, Wakefield was much more successful. Now, nearly a decade after he first started targeting the community, they are continuing to suffer measles outbreaks. I will begin with the story as it stands now and then go back and look at how it got to this point. The story takes place among a seemingly unlikely group of people in an unexpected location. It’s also a story that I can’t believe I’ve never blogged about before, given how long it’s been going on.
Measles outbreaks among Somali immigrants in Minnesota
Before I first encountered this story several years ago, I had no idea that there was a large community of Somali immigrants in Hennepin County in Minnesota, but there is. In fact, it’s the largest community of Somali immigrants in the US that began forming over a quarter of a century ago and now numbers in the several tens of thousands. Right now, the community is the center of a new measles outbreak, which is just the latest. From the Friday StarTribune:
As a registered nurse and a consultant to the Minnesota Department of Health, Asli Ashkir has spent nearly a decade talking with Somali parents about autism, vaccines and the importance of getting their children immunized.
Last week she redoubled her efforts. A measles outbreak in Hennepin County has sickened 12 children — all of them unvaccinated and all of them from Somali families, according to the department — throwing a spotlight on low immunization rates among Somali children.
Now state and county public health workers are doing their best to contact Somali parents and underscore the value of immunization. “I know when parents have facts, they do the best they can to make the right decision,” Ashkir said.
The story shows why the Somali community in the Twin Cities area is so susceptible to measles outbreak. All you have to do is to look at this graph of MMR vaccine uptake by year:
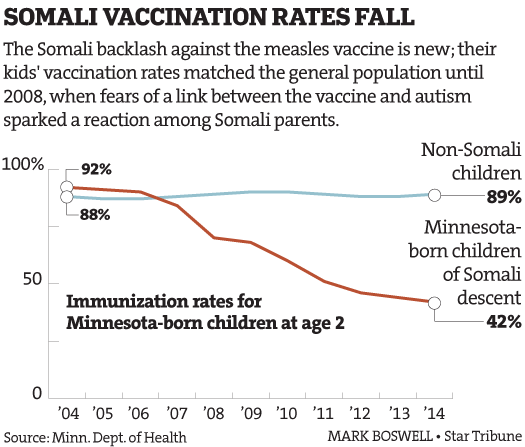
MMR uptake among Somali immigrants in Minnesota: This is the effect of nearly a decade of antivaccine propaganda.
The graph above shows what can only be described as a catastrophic plunge over the course of just one decade in MMR uptake among American-born children of Somali descent, from 92% to 42%. There is, for all intents and purposes, no herd immunity in this community. The interesting thing here, though, is that this plunge is very specific. It’s noted in the story that there is not a fear of vaccination in general among the Somali immigrant population. Rather, it’s fear of just one shot: the MMR. It is a fear that antivaxers stoked, beginning sometime around 2008, and they have unfortunately been wildly successful in inculcating fear of the MMR in Somalis in Minnesota. Indeed, a 2014 study examined attitudes towards the MMR vaccine in Somali and non-Somali children in Minnesota and found:
Somali parents were more likely than non-Somali parents to have refused the MMR vaccine for their child (odds ratio, 4.6; 95% confidence interval, 1.2–18.0). Most of them refused vaccines because they had heard of adverse effects associated with the vaccine or personally knew someone who suffered an adverse effect. Somali parents were significantly more likely to believe that autism is caused by vaccines (35% vs. 8% of non-Somali parents). Somalis were also more likely to be uncomfortable with administering multiple vaccines at one visit (odds ratio, 4.0; 95% confidence interval, 1.4–11.9) and more likely to believe that children receive too many vaccines.
It was a small survey, but it was the only one I found in the peer-reviewed medical literature thus far. Its results are not surprising, however, to anyone directly involved with the Somali community, particularly public health officials. There haven’t (yet) been studies published about this latest measles outbreak, but there was a study about the 2011 measles outbreak in Minnesota, which, to that point, was the largest such outbreak in 20 years, with 21 cases identified. Its conclusions were also unsurprising. The source was found to be a 30-month-old US-born child of Somali descent infected while visiting Kenya and then spread to the Somali and non-Somali population primarily through the unvaccinated:
Three case-patients had unknown vaccination status, 1 was vaccinated before the recommended age (11 months), and 1 was a health care worker who was thought to be immune (IgG-positive documented >10 years previously). Sixteen of 21 (76%) were unvaccinated; 7 of 16 (44%) were too young for routine vaccination. Nine (56%) children were age-eligible for routine vaccination but unvaccinated, 7 because of safety concerns owing to the misinformation that MMR vaccine causes autism; 6 of these children were of Somali descent. Two other children did not refuse but were behind on immunizations.
This is how the outbreak spread:
This outbreak began with an unvaccinated US-born child who was exposed to measles in an endemic region of Africa and developed disease on return to the United States. Low vaccination rates in the local Somali community, and subsequent exposures among susceptible homeless shelter residents, fueled ongoing transmission of measles. Delay of the source case-patient’s measles diagnosis also may have contributed to transmission before public health interventions. Although post-exposure prophylaxis, vaccination, and voluntary isolation and quarantine were implemented after the first known case, there was ongoing transmission in 1 of the 2 affected shelters. This transmission was attributable to several factors, including exposures that occurred before the first identified case, an exposure of an infant too young for MMR vaccine according to the routine schedule, as well as exposure of an infant who was too young for the early MMR vaccine outbreak recommendation. Other contributing factors were caused by the challenges of quickly assessing and documenting immune status in a large group of individuals living in a temporary, communal setting. These challenges allowed transmission to individuals who initially were assumed to be immune, but who lacked documentation. After ongoing transmission was seen, immune status testing was implemented for those who lacked documentation.
Notably, two-thirds of the cases in this outbreak were hospitalized, and many of these were hospitalized for respiratory complications in addition to dehydration, highlighting that measles is a severe infection even in well-resourced countries.
If measles is as harmless as antivaxers claim that it is, then why were two-thirds of the people stricken with measles in this outbreak hospitalized for complications? That’s a rhetorical question for antivaxers, obviously.
The first question that faces Minnesota public health officials is, of course: How did we get here? The second is: What can be done to combat MMR fear-mongering? I can’t help but note that the fear of the MMR that is so prevalent among Somali immigrants in Minnesota, while primarily about the MMR, is bleeding over to other vaccines. Some Somali immigrants are starting to show susceptibility to the “too many too soon” myth and, as a result, spacing out the remaining vaccines other than the MMR that they are willing to administer to their children, believing that early vaccination can “damage an infant’s language skills.” Basically, if you live in Minnesota, combatting antivaccine and anti-MMR views in the Somali immigrant community is imperative. Even if you don’t live there, given that the Twin Cities area is a hub of national and international transportation, measles could be as short as a quick plane flight to where you live.
So let’s look at how we got here. Andrew Wakefield has his fingerprints all over this, but it didn’t start with him. As is his usual MO, he opportunistically took advantage of a situation, as he did when he discovered that Brian Hooker had been recording telephone conversations with a disgruntled CDC scientist.
2008: Autism in the Somali immigrant community
The story of how the myth that MMR causes autism became so firmly entrenched among Somalis living in Minnesota began sometime around 2008, with a cluster of autism cases among the community and a news story, as described by Bahta et al. in Minnesota Medicine:
Parents in Minnesota’s Somali community have voiced concern that their children are disproportionately affected by autism spectrum disorder (ASD) compared with children of other ethnicities. Many in the community blame the MMR vaccine. In an August 2008 news story on WCCO-TV, one parent was quoted as saying, “It’s the vaccines.”
Shortly after the story aired, the Minnesota Department of Health reached out to members of the Somali community to gather more information. Health department staff attended meetings with Somali parents, many of whom were unfamiliar with ASD. Repeatedly, they stated that they don’t even have a word for autism in their language. In telling her story, one mother reported that in their attempt to understand ASD, she and others discovered groups that supported the claim that vaccines, particularly MMR, cause autism. Misinformation can spread rapidly in the Somali community, which has a rich oral tradition of passing information to one another. It is now widely accepted among Somali Minnesotans that MMR is to blame for autism.
The antivaccine movement was all over this story in 2008. For example, David Kirby, author of the book Evidence of Harm: Mercury in Vaccines and the Autism Epidemic: A Medical Controversy, which was one of the early works using pseudoscience to link thimerosal in vaccines to autism was writing articles like ‘Autism May Be Caused By “Chemical Exposures”‘ specifically about the Somali community in Minnesota, with a “wink, wink, nudge, nudge” that the “idea that ‘chemical exposures’ (vaccine related or otherwise) might cause autism still brings virtual apoplexia to certain scientific circles.” He had previously hammered the same theme on the antivaccine blog Age of Autism, noting from the data presented that “rate of autism among Somali children in the public schools had been reported at 1 in 28 kids” and that the “80 or so Somali parents who attended were disappointed, by all accounts, that Dr. Punyko had no way to tell them if autism among their children was, as they strongly suspect, more common than among non-Somalis the same age.”
But was autism more than twice as common among the American-born children of Somali immigrants, as the data linked to above suggest? In early 2009, the Minnesota Department of Health released a study of autism among Somali immigrants. It is a substantial read. Here are a couple of key findings, which, as is often the case in studies of autism compared to parental perception of autism prevalence, are not as clear as the prevalent belief among the Somali community in Minnesota or as the antivaccine movement latched onto:
- The administrative prevalence for three and four year old Somali children was significantly higher than for non-Somali children. This is consistent with the perceptions of the community that a larger number of Somali children were participating in ASD programs. Because of the study’s limitations, it is not proof that more Somali children have autism than other children; however, it does raise an important question about why Somali children are participating in this program more than other children.
- The relative difference between Somali and non-Somali administrative prevalence decreased markedly over the three years covered by the study. It is unclear if this is an identification issue, a change in parental awareness for the need for developmental screening or some other issue.
- Administrative prevalence rates for the Asian and Native American groups were found to be “strikingly low.” The reasons for these low rates are unknown, but they could be important to understanding whether the rate of ASD is higher among Somali children or underestimated among other children. In other words, the seemingly low prevalence rate among Asian and Native American children may artificially boost the comparative rate among Somali children, distorting a true understanding of all groups involved.
So, yes, administrative prevalence of autism was higher among Somali-Americans in Minnesota, but there were a lot of issues that made it difficult to use these data to determine for sure whether actual autism prevalence was higher, not the least of which was that as was noted in Left Brain, Right Brain, Department of Education data are not reliable for tracking autism. Jim Laidler made the same point in a publication in Pediatrics in 2005. Indeed, the most recent study of autism in the Somali-American community in Minneapolis was published in 2016 and found that Somali children were as likely to be identified with an autism spectrum disorder (ASD) as white children but that Somali children with ASD were significantly more likely to have an intellectual disability than children with ASD in all other racial and ethnic groups. Meanwhile, Steve Novella examined the cluster and proposed other potential causes for it, if even there was a cluster, such as vitamin D deficiency or a founder effect. Of course, as I pointed out above, it appears that children born to Somali immigrants are no more likely to be diagnosed with autism than white children; so there wasn’t even a cluster there. Unfortunately, it took eight years to figure that out.
By long before then, the damage had been done and the seed of distrust in the MMR and other vaccines had been planted by antivaxers. Over the next several years, as you will see, antivaxers nurtured that seed until it blossomed in the form of measles outbreaks.
Enter Andrew Wakefield
It’s not clear exactly when Andrew Wakefield first made contact with the Minnesota Somali community, but I do know that Age of Autism was on the case as early as August 2008 and that the founder of the antivaccine group Generation Rescue J.B. Handley published “An Open Letter to the Somali Parents of Minnesota” in which he told them it was the vaccines and that they can’t trust the local health authorities. He even went so far as to urge them to declare a “state of emergency within your community and create a new vaccine schedule for your kids.” Meanwhile, also as early as August 2008, David Kirby had been writing stories like ‘Is Autism an “American Disease?” Somali Immigrants Reportedly Have High Rates.’
I do know for sure from media accounts and triumphant blog posts in Age of Autism that he met multiple times with the community and its leaders between 2010 and 2011 and that he appears to be still intermittently in contact. For instance, here is one contemporaneous account in local media from 2010. It was a time when he proposed as “study” of autism in Somali immigrants and promised to raise funds for it, something he appears never to have done. At the same time he sold the study this way:
Minnesota Somalis worried about autism rates among their children recently invited controversial British researcher Andrew Wakefield to Minneapolis to talk to their community.
At a Somali community meeting in Minneapolis, Wakefield asked his audience to participate in a study. He told about a hundred people gathered at a Somali-owned restaurant that they could help find the cause of autism.
“It is solvable, it has a cause, it had a beginning and it must have an end,” Wakefield said. “We cannot accept the damage that is being done to all of these children. It is completely unacceptable and the suffering you’re going through.”
At the same talk, Wakefield claimed that there were no known cases of autism in Somalia, characterized in the story as an “anecdotal observation many Somalis confirm.” It staggers the mind that Wakefield would make such a claim (OK, actually, it doesn’t, given how big a liar Wakefield is), but it does not stagger the mind that Minnesota Somalis would find such a claim credible. Somalia is a poor country, and it does not stretch the imagination to speculate that most people living there are unfamiliar with autism. Nor does it bend credibility too much to observe that a Third World country is unlikely to have the same sort of screening and support programs for autism that we have in the US and other developed countries and that in such countries most cases of autism other than the most severe would go undiagnosed. Indeed, even the severe cases might well be diagnosed as mental retardation rather than autism.
Be that as it may, the cluster of autism in 2008 led to perceptions like this one:
She recalled a Somali mother who spoke at a public health meeting at the Brian Coyle Community Center some years ago. She had given birth to several healthy children in Africa, but her first child in the United States showed autism symptoms at an early age.
Wakefield visited Minneapolis again right in the middle of the 2011 measles outbreak to give a talk at a Somali restaurant. It was noted at the time that there were “a number of vocal pediatricians and doctors of Somali descent trying to speak out about this” but that distrust of health authorities was very high and local antivaccine groups like the Vaccine Safety Council of Minnesota were actively influencing Somalis. They still are. In 2016, for instance, the VSCM board member Patti Carroll published a warning to Somali parents that the Minnesota Department of Health “schools professionals to persuade Somali parents to give their children the MMR vaccine, despite clear opposition.”
Gee, you say that as though it were a bad thing.
That’s the problem, of course. Antivaxers are opportunistic in the extreme. If they see a population who are vulnerable to their disease-promoting message, they will pounce, and it’s always about the vaccines. They saw a story of a possible autism cluster among the children of Somali immigrants in Minnesota. Where scientists see such a story and ask “Is the cluster real and not spurious?” and “If it’s real, what might be causing it?” antivaxers see such a story and assume it absolutely, positively must be the vaccines. In this particular case, they took advantage of a newly arrived immigrant community’s lack of knowledge about autism and vaccines, its tradition in which information is primarily transmitted orally, and the distrust some of its members had for the local health authorities. The results are still playing out in catastrophically low MMR uptake and measles outbreaks.
What can be done?
As every source I’ve read over the years about the Minnesota Somali community and vaccines has stated, suspicion and fear of the MMR vaccine are now very much entrenched and will be very difficult to reverse. Indeed, it’s been pointed out:
Minnesota Department of Health staff found that fear of autism was often the reason for parents’ refusal to have their children vaccinated. Highly educated Somali Minnesotans are not exempt from this fear. As one Somali educator admitted, “My children did not get the MMR; my evidence is the Somali children I see who have autism.”
Parents who cited fear of autism as the reason for their vaccine hesitancy told health department staff that they received their information mostly from other Somali Minnesotans. Being told that MMR does not cause autism was not satisfactory for many parents because no one could tell them what does cause autism. Yet, when asked whom they would trust for health information, nearly all said they trusted their health care provider. And a significant number who refused vaccinations said they would reconsider their decision if they were given more information.
Parents of children diagnosed with ASD were articulate about their belief in an association between MMR and autism and sometimes also implicated receipt of multiple vaccines as the cause of their child’s autism. Some Somali parents have come to realize that autism and vaccines are unrelated, but they are in the minority.
Vaccine hesitant Somali parents thus resemble our own native-grown antivaxers and vaccine hesitant parents in many ways. Many are highly intelligent and educated. They get their misinformation about vaccines and autism from their peers more than from medical authorities. Also, it is the parents who have children diagnosed with ASD who are the most passionate and persuasive in arguing that vaccines are linked with autism, and, because of the low rate of measles (thanks to the MMR) many Somali parents view autism as a greater threat to their children than the measles and base their decisions about vaccines on that misperception. One difference is that, unlike many of our native antivaxers, Somali immigrants generally hold the medical profession in high esteem and are thus more open to being influenced by physicians and other clinicians. Actually, I should be a bit more clear. American antivaxers generally distrust the medical profession, while American parents who are vaccine-hesitant tend to hold the medical profession in higher esteem.
Be that as it may the Minnesota Department of Health has been trying to meet the challenge of reaching Somali parents through outreach programs in the schools and day care centers aimed at increasing awareness of Somali children’s growing vulnerability to vaccine-preventable diseases. Bahta et al note:
Finding ways to leverage the respect Somalis have for doctors and other health care professionals is challenging. In studies examining how clinicians can provide effective care to Somali patients, building trust has been identified as important. Two things that contribute to trust that are repeatedly cited in the literature are the availability of a competent interpreter and not feeling rushed by the clinician. Clinic policies such as ensuring that a professional interpreter is available, adding time to appointments when interpreters are needed, and consistently scheduling families with the same clinician can support efforts to build trusting relationships with Somali patients.
At their heart, strategies like these are no different than techniques used with the vaccine-hesitant of any race or nationality, adapted to Somali parents by including an interpreter. There’s one area where the Minnesota Somali community might be a bit different, though:
They also want clear direction from their physicians. Providing parents with options may confuse them. A statement such as, “We can give your child the vaccine today, or if you want, we can wait,” may be perceived by the parent as meaning that the clinician also has reservations about vaccines or thinks that either choice is acceptable. One Somali interpreter described an interaction this way: “When the mother told the doctor that she did not want her child to get the triple-letter vaccine, the doctor said, ‘OK.’” The interpreter was worried that the parent thought the doctor agreed that the MMR vaccine wasn’t needed or that he, too, was worried about its effects.
This is different from American parents, who tend to resent being told too firmly what to do and want to make their own decisions. Again, what this shows is the importance of flexibility in dealing with vaccine hesitant parents and how strategies and messaging, although generally sharing the same broad themes, have to be adapted to the specific population being targeted. It’s also important to remember that Minnesota Somalis are not monolithic. Although anti-MMR views predominate and antivaccine views have become common, there have been (and still are) members of the community who are joining forces with Minnesota health officials to push back.
Unfortunately, progress is likely to be slow, as changing entrenched beliefs is difficult and requires a sustained, targeted effort. In the meantime, the children of the Minnesota Somali community will remain vulnerable to measles and potentially other vaccine-preventable diseases and are likely to serve as the nidus for further outbreaks until the MMR uptake rate can be raised back to what it was in 2004. Remember, it took the UK many years to lift its MMR uptake level back to somewhere near where it was before Wakefield, aided and abetted by the tabloid press, caused the MMR panic. There’s no reason to expect that a similar recovery will take any less time in Minnesota.
Sadly, measles is the gift that keeps on giving, and nobody is better than giving it than Andrew Wakefield. The Somali immigrant community in Minnesota is now finding that out.