
{kind=link}
Ever since the COVID-19 pandemic reared its ugly head in China and then made its way to Europe and the rest of the world, conspiracy theorists have had a field day. Whether it was the idea that the 5G rollout in Wuhan, China somehow sparked or accelerated the COVID-19 outbreaks that evolved into the pandemic, that the influenza vaccine makes you more susceptible to COVID-19, or that COVID-19 was bioengineered in a laboratory and thus the pandemic is really a “plandemic” designed to control and subjugate the population (or even to depopulate the earth by over 90% so that elites, working with aliens—yes, aliens!—could exploit the population and its resources), conspiracy theories have been flowing fast and furious since early this year. Meanwhile, antivaxxers rapidly formed an unholy alliance with antimaskers, COVID-19 pandemic minimizers and deniers, and others opposing public health mandates to control the spread of SARS-CoV-2, the coronavirus that causes COVID-19 (including QAnon believers!) while infusing that movement with antivaccine pseudoscience and conspiracy theories and launching a pre-emptive disinformation war against COVID-19 vaccines. Antivax leader and propagandist Robert F. Kennedy, Jr has gone all-in on COVID-19 minimization/denial, and Del Bigtree, who made the antivaccine propaganda film VAXXED with Andrew Wakefield, has urged his listeners to “catch this cold” in order to build up herd immunity among the “healthy,” because, to him, COVID-19 is not dangerous except to those who deserve to be endangered, specifically those with chronic conditions due to overeating, lack of exercise, excess drink, and the like. It was blaming the victim at its most blatant, very typical of antivaccine activists.
This brings me to the latest propaganda line being promoted by COVID-19 deniers and antivaxxers, that of the “casedemic”.
What is the “casedemic”?
What is a “casedemic”? Last week, über-quack tycoon (worth over $100 million!) Joseph Mercola, DO published an article entitled “Asymptomatic ‘Casedemic’ Is a Perpetuation of Needless Fear“. Amusingly, Mercola prominently lists his article as having been “fact-checked”, to which I can only respond: “Fact-checked? You keep using that word. I do not think it means what you think it means.”
Before I deconstruct Mercola’s claims, let’s take a moment to consider why “casedemic” has been a buzzword among COVID-19 deniers and antivaxxers lately. As of my writing this yesterday, COVID-19 is spreading out of control throughout huge swaths of the US, with the number of (known) cases hitting 12 million and the number of deaths surpassing a quarter of a million. Hospitalizations are climbing, and in large areas of the US, hospitals and the healthcare system are straining under the load of caring for so many COVID-19 patients. The situation is only getting worse, with hospitals in half the states facing massive staffing shortages, especially shortages of ICU nurses. In the face of such empirical numbers, it’s difficult to deny how severe the COVID-19 pandemic currently is in the US; that is, unless you find a way to redefine your terms. Enter the “casedemic”, in which antivaxxers and COVID-19 deniers try to claim that what we are seeing is an epidemic of positive tests, not of real disease, hence the term. Indeed, if you do a search of the term “casedemic”, you’ll find articles from the usual COVID-19 denying suspects arguing that the now-exponential increase in COVID-19 cases is not due to real disease, but rather an artifact of wider testing.
Basically, “casedemic” is just a new name for an old COVID-19 denier trope, that increased testing explains the pandemic and that COVID-19 is not dangerous. Indeed, a Google Trends search shows that the term didn’t show up as Google searches until early August, but I’ve been as yet unable to figure out who coined the word:
The earliest example in which the term “casedemic” was used was this Tweet:
I think that might be the first instance of “casedemic” and that Ivor Cummins might well have been the person who coined the term, but I really don’t know for sure. Ivor Cummins, for those unfamiliar with him, is an engineer who decided he knew more about nutrition and health than actual, you know, nutritionists and physicians and had established himself as a nutrition quack under the title “Fat Emperor” long before COVID-19. Once the pandemic hit, he rapidly pivoted to become a COVID-19 grifter and has become hugely influential among the COVID-19 denial crowd. His shtick has been pretty much this, to claim that COVID-19 numbers are being vastly inflated due to increased testing and that it’s not that dangerous. Cummins rates a post of his own, and I’ve been meaning to do one discussing his pseudoscience about diet and COVID-10, but today is not the day for it.
Here’s where antivaxxers glom on. After all, if COVID-19 is not dangerous, particularly if it’s not more dangerous than the flu, then there’s no need for masking, no need for social distancing, no need for public health interventions such as restricting activities known to be sources of spread (such as indoor dining at restaurants and having those who can work from home do so), and, above all, no need for a vaccine.
Now let’s get back to Mercola. Mercola relies largely on a video by Del Bigtree. (It’s always a bad idea to use such an unreliable source, but if there’s one thing that Bigtree is skilled at, it’s crafting science-denying and antivaccine propaganda that sounds convincing to people who are not well versed in the relevant sciences.) I’m not going to embed it or link to it; it’s in the article if you really want to subject yourself to 23 minutes of Bigtree’s rambling. It also amuses me when someone who knows nothing about PCR pontificates about PCR, the way that Bigtree and Mercola do.
PCR basics
I know PCR, which stands for “polymerase chain reaction” and is a highly sensitive technique to amplify tiny quantities of specific DNA sequences. (I’ve discussed PCR before in the context of its misuse by antivaccine advocates.) Before I drifted away from doing benchwork myself—as lab directors tend to do as time goes on—I had done literally thousands of PCR assays personally in my time as a lab rat, dating back to the 1990s, when PCR was new. I had done thousands of real time quantitative PCR assays as well. Even though it’s been a few years since I’ve personally done PCR, I know PCR. I’ve troubleshot more PCR reactions than I can remember. So, it was with a combination of amusement and disgust that I watched Bigtree and Mercola cherry pick facts about PCR and twist known problems with PCR testing into casting doubt on the reliability of all PCR testing for COVID-19.
This brings us back to Mercola:
As coronavirus testing takes place en masse across the U.S., many are questioning whether the tests are accurate enough to trust, especially in people who are asymptomatic. Positive reverse transcription polymerase chain reaction (RT-PCR) tests have several drawbacks that make mass testing problematic and rife for misleading fearmongering.
For starters, the PCR test is not designed to be used as a diagnostic tool as it cannot distinguish between inactive viruses and “live” or reproductive ones.1 This is a crucial point, since inactive and reproductive viruses are not interchangeable in terms of infectivity. If you have a nonreproductive virus in your body, you will not get sick and you cannot spread it to others.
It really irks me when a quack like Mercola lectures about a fact regarding a medical test or intervention as though scientists and physicians have never thought of it before! Here’s how reverse-transcriptase polymerase chain reaction (RT-PCR) works. Because COVID-19 is an RNA virus, in order to amplify part of its sequence, first the RNA has to be converted to DNA, which is done with an enzyme called reverse transcriptase, which reverse transcribes RNA to DNA. Then that DNA can be amplified using a standard PCR reaction, which uses two primers designed to match specific sequences on the target DNA sequence. Basically, two different primers (short stretches of DNA designed to be complementary to and thus bind to a sequence of interest, each of which are on opposite strands “aimed” at each other are mixed with the sample containing the DNA of interest and then run through different temperature steps. First is the denaturation step at 95° C, which guarantees that all the DNA of interest has been separated into its two complementary strands. Next, the temperature is dropped lower to allow the primers to bind to their complementary sequences (the annealing phase). This temperature can’t be too low, or nonspecific binding of primer to other DNA sequences that don’t exactly match will occur, leading to amplification of DNA other than the intended sequence. It can’t be too high either, or there won’t be enough binding. Next, comes the elongation phase, where the temperature is increased to 72° or thereabouts, which is near the optimal temperature for Taq polymerase to do its thing. Finally comes another denaturation phase, where the temperature is briefly boosted to 95° to separate the strands, after which the temperature is dropped again to the annealing temperature and the cycle begins anew. Because the number of copies of the target DNA sequence roughly doubles every cycle, after 30-40 cycles even single DNA copies can be detected. Here’s what it looks like in schematic form:
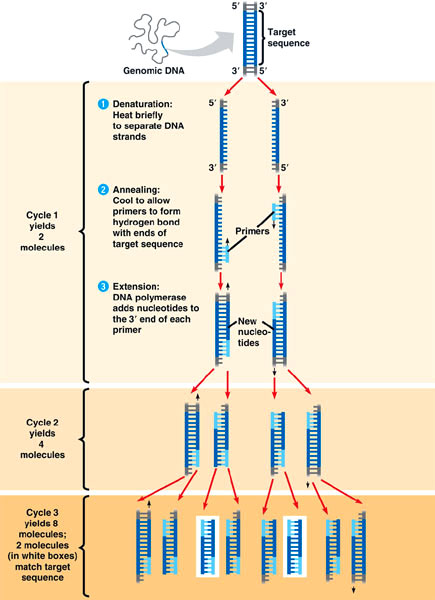
How PCR works
There’s a variant of PCR known as real time quantitative PCR, in which each cycle releases a fluorescent marker, whose signal can be quantified with each cycle. Back in the old days, PCR was basically a yes-no test. You’d run the PCR reaction for a given number of cycles, and you either could or could not see a band on a DNA separation gel. With real time PCR, accurate quantification of the DNA target present is possible. For purposes of my discussion, you really don’t need to know the details other than to know that this is the case.
In any event, the greatest power of PCR also leads to the biggest pitfalls in its application. Basically, PCR is so sensitive that it’s very easy for a PCR reaction to amplify a contaminant or for the primers to anneal to sequences that are similar but not identical and thus amplify DNA other than the sequence of interest. Indeed, I’ve encountered all of these pitfalls and more. That is why controls are of the utmost importance. For example, there has to be a good negative control to let the researcher know that the chosen PCR conditions are not amplifying junk. Moreover, if you’ve designed your primers poorly or if you anneal at too low a temperature, you can get nonspecific binding and amplify sequences that you don’t want to. Overall, PCR can be a very tricky game, and it gets trickier the more cycles you use to amplify and the lower amounts of target sequence you are trying to amplify. PCR is an exponential amplification; small variations in early cycles can have enormous effects in later cycle, producing wide variation in results. Every scientist who’s ever done a significant amount of PCR knows these pitfalls and takes steps to avoid them. Mercola treats them as though no one knows about them and that describing them is some sort of “revelation” or “secret” that scientists are hiding from you.
Back to the “casedemic”.
Joe Mercola: Regurgitating disinformation about COVID-19
So let’s get to the primary claim that falls under the term “casedemic”:
In summary, the PCR swab collects RNA from your nasal cavity. This RNA is then reverse transcribed into DNA. However, because the genetic snippets are so tiny, they must be amplified to become discernible.
Each round of amplification is called a cycle, and the number of amplification cycles used by any given test or lab is called a cycle threshold. Amplification over 35 cycles is considered unreliable and scientifically unjustified. Some experts say nothing above 30 cycles should be used,3 yet Drosten tests and tests recommended by the World Health Organization are set to 45 cycles.4,5,6
When you go above 30 cycles, even insignificant sequences of viral DNA end up being magnified to the point that the test reads positive even if your viral load is extremely low or the virus is inactive and poses no threat to you or anyone else.
Isn’t that last part pretty much what I was saying above? See what I mean about quacks treating well-known problems with a medical test or intervention as a “revelation” of “secret knowledge” that “they” don’t want you to know about.
Yes, it is true that doing PCR on swab tests from the nasopharynx only tells you whether there is detectable SARS-CoV-2 RNA present in the specimen; it does not say whether that RNA comes from infectious virus or is causing a clinical infection. Yes, it is true that PCR picks up many asymptomatic cases, but it is also true that asymptomatic patients can still spread COVID-19, old WHO statements in June notwithstanding, which is why identifying these cases is important. It is also true that there has been a bit of controversy over what the appropriate PCR threshold count should be for COVID-19 testing, as well as that early in the pandemic PCR tests were a lot less reliable. (Just witness the CDC debacle when it tried designing its own PCR test for SARS-CoV-2.) However, now, nearly a year into the global pandemic and nearly ten months after the pandemic hit US shores, we have a lot more experience with these tests. More on that in a moment, but first let’s let Mercola have some more rope to hang himself with, scientifically speaking:
When labs use these excessive cycle thresholds, you end up with a far higher number of positive tests than you would otherwise. At present, and going back a number of months now, what we’re really dealing with is a “casedemic,”7,8 meaning an epidemic of false positives.
Remember, in medical terminology, when used accurately, a “case” refers to someone who has symptoms of a disease. By erroneously reporting positive tests as “cases,” the pandemic appears magnitudes worse than it actually is.
Hilariously, reference #7 is not a scientific paper. It’s an article from PJ Media, the right-wing propaganda “news” network, and is basically a rant against Joe Biden that, amusingly, self-references another article in PJ Media that quotes a New York Times article without actually linking to it. What did the article say? Basically, the NYT looked at a bunch of PCR tests done by one lab, the Wadsworth Center (a New York State lab) and identified 872 positive tests in July, positives that were based on a threshold of 40 cycles. They found that with a cutoff of 35, about 43% of those tests would no longer have qualified as positive and that about 63% would no longer have been judged positive if the cycles were limited to 30. Interestingly, this NYT article was published in late August, but I have yet to see any peer-reviewed publication on it. The only possibly relevant publication I could find from the Wadsworth Center reported its evaluation of the NeuMoDx™ SARS-CoV-2 assay, performed on a NeuMoDx molecular system, a rapid, fully automated, qualitative real-time RT-PCR diagnostic test with throughput of up to 288 tests in an 8 hour shift. The article concluded that this automated system had a similar sensitivity and specificity to the CDC assay. So this does sound rather odd, but in reality way too much is being made of this single survey by a newspaper and not published in the peer-reviewed medical literature.
As for the second “reference”, it’s to an article published on the website of that medical conspiracy theorist group disguised as a medical professional organization, the Association of American Physicians and Surgeons (AAPS), which is known for its antivaccine views, denial of climate science, and all manner of conspiracy theories. (AAPS even published an article by Andrew Wakefield predicting a “mass extinction” due to the MMR vaccine. I kid you not.) Hilariously, even the AAPS acknowledges that “coronavirus is not a pseudo-epidemic” and that “thousands have died”, even as it speculates that the ‘dreaded “second wave” might be a surge of false positive tests that are inevitable in mass screenings of healthy persons’. Of course, AAPS fails to mention that hospitalizations and deaths are also rising rapidly, which would definitely go against the latest COVID-19 wave being a “casedemic”.
Why, though? Why would governments, scientists, physicians, and public health officials who’ve dedicated their lives to combatting infectious disease want to do this? I bet you know where this is going:
“The goal is to keep you scared, isolated and demoralized for a purpose,” says PJ Media.9 “Only a beaten nation would stand for what comes next.” And that next step is a reset of America as you know it, with the UN’s one-world Agenda 2030 at the helm.
Mercola even links to an article of his from three weeks ago called “The Great Reset“, in which he posits that the COVID-19 pandemic is being used as a pretext for the “Great Reset”, whose purpose is to “usher in a tech-driven dystopia free of democratic controls” and create a “new ‘social contract’ that ties you to it through an electronic ID linked to your bank account and health records, and a ‘social credit’ ID that will dictate every facet of your life.” Because of course it is. And, to Mercola and his fellow conspiracy mongers, COVID-19 PCR testing is a primary tool in achieving that end by creating a “casedemic” of illusory COVID-19 cases.
There’s just one problem. Actually, there are several.
The problem with the “casedemic” conspiracy theory
Anyone who’s done PCR knows that cranking up the number of cycles does indeed increase the chances of amplifying a contaminant or a sequence that is similar, but not identical, to the intended target sequence. (Again, it amuses me how cranks like Joe Mercola treat this long known issue with PCR as though it were some sort of astounding revelation that scientists have never thought about much before.) Is it a potential problem that PCR tests might be too sensitive for their intended purpose, namely screening for COVID-19 infection? Yes. However, as is almost always the case in these situations, the COVID-19 denialist cranks and conspiracy theorists have latched on to a problem and amplified it far out of proportion to its significance, all in order to cast doubt on the entire process of COVID-19 screening. Gideon M-K, a.k.a. the Health Nerd, pointed this out a couple of weeks ago, which seems to be when this whole “casedemic” thing started to percolate up onto social media in a way not seen since August:
There is no 'casedemic' – why the idea that COVID-19 cases can rise by deaths will not is simply a myth @MackayIM @CaulfieldTim https://t.co/BxTcTyYhH9
— Health Nerd (@GidMK) November 6, 2020
Here’s what he points out:
As cases of COVID-19 skyrocket across Europe and the United States, a new myth has emerged to add to our ever-increasing list of coronavirus-related nonsense. The idea is that the current massive epidemic in Europe and elsewhere is not an issue, because this is a ‘casedemic’ — an increase in cases without any concomitant increase in sickness or deaths.
Basically, it’s another way of saying that the pandemic is over, from people who’ve been saying that it was over every month since March.
Thing is, this new piece of disinformation is simply factually inaccurate, and is driven by a simple misunderstanding: that the second wave of COVID-19 was dramatically different to the first. In fact, the two waves are much more alike than you’d imagine, because the disease probably hasn’t changed enormously in the last 6 months or so no matter how much we wish that it has.
In other words, while the number of cases that are appearing positive now seems far higher than at the start of the year, in fact what we know is that we missed a huge proportion of cases back in March and actually it’s more than likely that the current wave looks very similar to the first.
This, again, is not a new observation. Early in the pandemic, scientists pointed out that, due to the massive shortage of COVID-19 tests that led to, in essence, rationing in which only those who were hospitalized or had severe symptoms were tested (and sometimes not even they were always tested), huge numbers of milder cases were being missed. Many were the public health officials who predicted that, as more testing became available, the apparent infection fatality rate (IFR, the percent who have the infection and die, whether symptomatic or not) would decline as more mild and asymptomatic cases that weren’t being detected before started being detected.
To demonstrate this, the Health Nerd did a clever back calculation based on the number of deaths per time period, correcting for age, to extrapolate what the IFR would have been early in the pandemic if we were doing as many tests then as we are now and found:
Suddenly, the difference disappears! Indeed, it looks like the first wave might have even been a bit BIGGER than the second. This makes perfect sense when you consider that, at least in the United States, the number of tests being done each week in March was in the hundreds of thousands, and limited mostly to people who were being hospitalized for COVID-19. So we missed almost everyone with a mild infection, and cannot have picked up the millions of cases that almost certainly existed at the time.
He further predicts, based on what’s happened before, that hospitalizations and deaths will increase, because when a lot more people test positive for COVID-19, a lot more people will be hospitalized even if only a relatively small percent of the total infections get that sick, and, eventually, a lot of those people will die, even if the total is “only” less than 1% of the total infection rate. There’s just a lag of several weeks for the virus to do its work, for people to die, and for the deaths to be reported.
Ian Mackay, virologist and adjunct Associate Professor at the University of Queensland had another way of putting it, namely More testing shows more iceberg. Like the Health Nerd, Mackay emphasizes that, early in the pandemic, there was a massive shortage of testing kits:
One thing is pretty clear: laboratories and biotechnology companies worldwide were unprepared for the scale of a pandemic. This wasn’t a slow-moving SARS-CoV or a poorly transmitting MERS-CoV. This was a fast-moving, fully armed, well-equipped, respiratory virus. Labs couldn’t keep pace. And even though test development was super-quick, the fuel to feed and power what those tests needed, quickly became scarce.
Despite the lab challenges posed by Ebola virus epidemics in Africa just a few years ago, and Zika virus epidemics across the world, testing wasn’t ready enough for pandemic 2020. In today’s world, a pandemic was always going to mean using real-time PCR-based tools to detect the virus. These were the most sensitive tests we had. Also, we didn’t have a better tool because no replacement had hit the mainstream. Despite the recurring promise of new platforms pitched during recent outbreaks and epidemics, PCR hasn’t faced a mainstream challenger since its real-time iteration hit the brights [sic] lights in 2009.
The analogy is simple. Early in the pandemic, we were only detecting the “tip of the iceberg” of COVID-19 cases. With more testing, we’re now seeing more of the iceberg, namely the part that lies “below the water,” so to speak, and wasn’t detected in March and April because not enough people were being tested and a lot of cases were going undiagnosed and undetected.
More importantly, though, to counter the claim of a “casedemic”, using PCR to detect a virus is more complicated than someone like Mercola lets on. It depends on so many things, not the least of which is sample collection, which can result in a high degree of variability in detectable RNA in a person’s sample. As cranks ignore that complexity, Mackay shares my amusement at how cranks portray a certain observation as such an amazing revelation:
Look, I fully agree that the later (higher number) the threshold cycle (CT “cycle number”) of the RT-PCR result, the less target RNA is present at the start of the reaction. That RNA is a surrogate marker for the amount of virus but not an actual measure because PCR methods can’t tell you a virus is infectious.
People are very chuffed to have learned this fact in 2020 by the way. You can tell because they say so. A lot. But despite their newfound out-of-context knowledge they actually know very little about what they’re talking about.
See what I mean? Yes, Mr. Bigtree and “Dr.” Mercola, real scientists who do PCR are laughing at you.
In any event, Mackay cites a study from Eurosurveillance that highlights the variability in PCR results, as well as the “gold standard” test of demonstrating the ability of virus from an isolate to be able to infect appropriate cells in cell culture, pointing out, based on the result reported that from among 5/60 (8.3%) of patient samples with a CT greater than 35, infectious virus was still present:
The figure shows that if you were to blindly and ignorantly rely on single CT values to proclaim lack of infectious risk – let’s say 35 or greater – you would miss people who were still shedding infectious virus.
If you surveyed more labs with expertise in cell culture and virus isolation and labs that could get hold of fresh samples and samples from the actual site of virus replication, I’m sure you could find even later CTs. You can also find labs who can’t isolate virus from samples with CTs this late. This biological variability means we need to step back from these stupid single number cut-offs.
Precisely. Setting the threshold count (CT) cutoff on a PCR test is a balancing act, in which you balance the increased sensitivity of using a higher CT and more amplification cycles as your cutoff and the attendant possibility of more false positives associated with that more sensitive cutoff against the possibility of missing a lot more cases of real infection if you use a lower CT. Another way of looking at it is this. If there were so many false positives, then PCR reactions all over the world should be generating them in huge numbers now. But:
Well in the denialist parallel universe, no one ever dies of Covid. They either die "with", or it's a "false positive".
Never mind that largely Covid-free countries like AUS or NZ use the same testing methods and report ~0.1% *total* positives.— Klaus Hentrich 🇺🇦 (@KHInnovation) November 20, 2020
Mackay points to the example of Australia, which currently has no reported local transmission of SARS-CoV-2, noting that “Australia’s COVID-19 cases right now are almost exclusively in quarantine hotels and among Aussies returning, or special-purpose travellers visiting, from a world on fire” and that Australia has “had a few clusters spin out from quarantine but they’ve–so far–been squished dead in weeks to months.” He further notes that Australia’s testing rate hasn’t fallen below 20,000/day since June. He then notes:
All that testing provides a good number of opportunities for those so-called false-positive PCR results to show up in our daily reported numbers. Surely more testing should mean a steady flow of false positives if these conspiracies are correct? And others love to add that it should be even more of a problem in a low prevalence setting. Australia certainly fits that bill. Plus, we’re testing mostly sick people but also asymptomatic and presymptomatic people.
But lo and behold there is no steady stream of false positives. We don’t have an issue because once again, this is an over-oxygenated amateur conspiracy theory and not an actual issue.
Local context also matters. For example, in a situation in which the disease being tested for is present at low prevalence (say, less than 2% of the population), even a test that is very specific and sensitive can produce a lot of false positives compared to “true” positives. I won’t go into the gory details (if you want discussions of sensitivity, specificity, and positive and negative predictive values, go here, here, and here), can lead to a lower positive predictive value (PPV), which is the likelihood, given a positive test, that there really is disease present. To put it simply (but hopefully not simplistically), the lower the prevalence of a disease, the lower the positive predictive value of a test for that disease, even a good one, is likely to be, because even low rates of false positivity will be high (half, equal, or even greater) compared to the actual prevalence of the disease in the population.
Basically, yes, there are false positives on PCR testing, but false positives are not nearly as huge a problem as people like Del Bigtree and Joe Mercola want to lead you to believe, and, contrary to their portrayal of scientists, physicians, and public health officials as oblivious to this problem, all these people working to find science-based methods to slow the spread of COVID-19 and bring the pandemic under control do consider the potential for false positives and seek to find ways to account for them and reduce them. Also, when the PCR testing is done properly in the context of a larger public health effort, the overall process will make sure that the lab results are considered along with the epidemiological and clinical context. Similarly, because the issues with PCR tests are known, other tests are being increasingly used. Rapid antigen tests are less sensitive, but detect the actual proteins made by cells as a result of SARS-CoV-2 infection, something not seen from an inactive virus. Serum antibody tests, which detect antibody to SARS-CoV-2 in the blood made as a result of infection, can tell us who has recovered from infection (or been infected long enough to develop an antibody response).
COVID-19 science denial is basically no different from any other form of medical science denial that we’ve covered here. It uses the same techniques of distraction to produce disinformation. In this case, Bigtree and Mercola are latching on to a legitimate controversy over the minutiae of a lab test and vastly exaggerating the significance of the controversy and magnitude of the problems it causes in order to cast doubt on the very process of testing for the disease itself, which is their real purpose. They are not promoting better and more accurate COVID-19 testing, which is what we all want, especially physicians and scientists on the front lines fighting the pandemic. They are doing their best to deny that COVID-19 is as huge and deadly a problem as it actually is, because if COVID-19 really is that big a problem then it does, contrary to their views, justify massive public health interventions to decrease infection and death rates, and, ultimately, a mass vaccination program.