{kind=link}
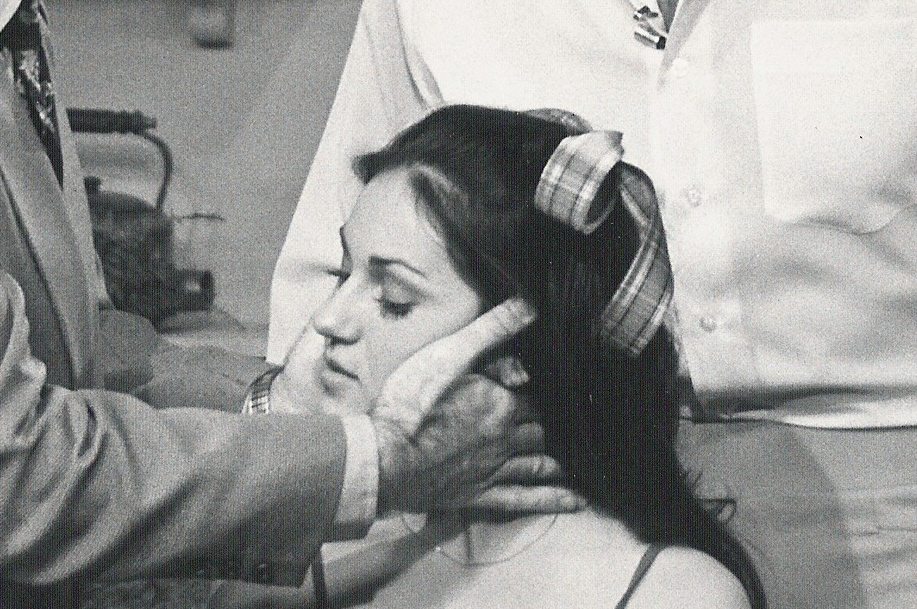
Photo by Sam Homola. Model: Alexis Alexander
The subject of neck manipulation as a possible cause of stroke has been discussed many times on Science-Based Medicine. With increasing use of neck manipulation as a form of manual therapy, and the proliferation of articles for and against use of such treatment, it is essential to continue reviewing different perspectives on this subject in order to make an informed choice when considering use of neck manipulation.
When RAND published its review of the appropriateness of manipulation and mobilization of the cervical spine in 1996 (reporting limited benefits as a treatment for neck pain and tension headache), only 11.1 percent of all reported indications for use of cervical manipulation were considered to be appropriate. Serious complications arising from manipulation of the cervical spine were estimated to be 1.46 per one million manipulations. The vast majority of the complications were reported to be “vertebrobasilar accidents”.
In a 2003 study, a team of neurologists who reviewed the medical records of patients under 60 years of age who had suffered cervical artery dissection and ischemic stroke concluded that spinal manipulative therapy is independently associated with vertebral artery dissection.
In 2014, the American Heart Association and the American Stroke Association issued a joint statement supporting studies that had found an association between cervical manipulative therapy and vertebral artery dissection stroke in young patients.
Diversity of views and opinions
Today, despite repeated warnings that neck manipulation might be a cause of stroke, neck pain and headache are commonly treated by manipulating the cervical spine. Downplaying the possibility of harm from such treatment, some manual therapists argue that the statistical association between visits to chiropractors and vertebral artery dissection can be explained as being the result of patients undergoing manipulation for neck pain that was an early symptom of a stroke in progress. This argument does not excuse the neglect of manipulating the neck of a patient who has symptoms of vertebral artery dissection (thus exacerbating the dissection), and it fails to consider that stroke symptoms which develop during or immediately following neck manipulation may be the result of trauma that injures a healthy vertebral artery.
Studies reporting that the occurrence of stroke is no greater in patients under chiropractic care than in patients under primary careare often presented as evidence defending use of neck manipulation. Most persons suffering from obvious symptoms of stroke will see a primary care physician rather than a chiropractor. For this reason, one would normally expect that the number of strokes occurring in patients under primary care would be greater than the number of strokes occurring in patients under chiropractic care. Strokes occurring among chiropractic patients who may be routinely subjected to neck manipulation as a preventive or treatment measure for a variety of health problems (per subluxation theory) should raise concerns that such strokes might be caused by neck manipulation, as opposed to strokes occurring among patents who visit a primary care physician seeking treatment for symptoms of stroke.
A 2014 article in The Journal of Stroke and Cerebrovascular Disease reported that the Cassidy study and others like it underestimated the strength of the association of spinal manipulation with cervical arterial dissection, concluding that:
Prior studies grossly misclassified cases of cervical dissection and mistakenly dismissed a causal association with manipulation. Our study indicates that the OR [odds ratio] for spinal manipulation exposure in cervical artery dissection is higher than previously reported.
Often-quoted studies done by physical therapists, chiropractors, and osteopaths have reported that head position and upper neck manipulation do not significantly affect blood flow in vertebral arteries. Other studies have demonstrated that the stretch of upper cervical end-range rotary mobilization and manipulative techniques can reduce blood flow in the vertebral artery on the side opposite the direction of rotation.
Vertebral arteries are most commonly injured by stretching of the arterial walls. Such injury can cause dissection or separation of the intimal layer of the artery from the medial layer of the artery (forming an aneurysm-like hematoma that might occlude the artery) or the formation of an intimal blood clot that may break loose days or weeks later to block blood flow to the posterior portion of the brain. Although there may be risk of stroke with a single neck manipulation, the risk may be greater with multiple manipulations. Stretching of a vertebral artery by manipulating the upper cervical spine may not significantly interfere with blood flow until dissection occurs as a result of repetitive stress injury or until a clot or an atherosclerotic plaque is released ─ a rare but deadly accident.
A Cochrane review of the literature dealing with use of manipulation or mobilization in the treatment of acute/sub-acute/chronic neck pain warned that “the risk of rare but serious adverse events for manipulation exists,” offering this conclusion:
Multiple cervical manipulation sessions may provide better relief and functional improvement than certain medications at immediate/intermediate/long-term follow-up. Since the risk of rare but serious adverse events for manipulation exists, further high-priority research focusing on mobilization and comparing mobilization or manipulation versus other treatment options is needed to guide clinicians in their treatment choices.
A review by Church et al concluded that “there is no convincing evidence to support a causal link between chiropractic manipulation and CAD [cervical artery dissection]”. However, some case reports describe strokes that have occurred during or immediately following neck manipulation, with a disproportional number of such strokes occurring in young, healthy persons (most under the age of 45). Some of these injuries have been confirmed by imaging studies that show dissection of healthy cervical arteries due to trauma.
The American Heart Association and the American Stroke Association (AHA/ASA), after reviewing all relevant literature, reported that population controlled studies found an association between cervical manipulative therapy and vertebral artery dissection in young patients, offering this precautionary advice [Italics added]:
CD [cervical artery dissection] is an important cause of ischemic stroke in young and middle-aged patients. CD is most prevalent in the upper cervical spine and can involve the internal carotid artery or vertebral artery. Although current biomedical evidence is insufficient to establish the claim that CMT [cervical manipulative therapy] causes CD, clinical reports suggest that mechanical forces play a role in a considerable number of CDs and most population controlled studies have found an association between CMT and VAD [vertebral artery dissection] stroke in young patients. Although the incidence of CMT-associated CD in patients who have previously received CMT is not well established, and probably low, practitioners should strongly consider the possibility of CD as a presenting symptom, and patients should be informed of the statistical association between CD and CMT prior to undergoing manipulation of the cervical spine.
The above Scientific Statement by the AHA/ASA was endorsed by the American Association of Neurological Surgeons and the Congress of Neurological Surgeons, providing powerful support for reports suggesting that neck manipulation can be an independent factor in the development of a vertebrobasilar stroke.
Manipulation-related stroke: An apparent reality
Heeding warnings that spinal manipulation may be independently associated with vertebral artery dissection, most health-care professionals now generally accept the assumption that neck manipulation can be a cause of stroke. While there may be no conclusive proof that neck manipulation can injure a cervical artery, the totality of evidence indicates that such injuries do occur. Providers of neck manipulation should warn any patient about to undergo neck manipulation that there is a risk of stroke caused by injury to a cervical artery, always weighing risk vs. benefit as compared with other treatment options.
Although carotid arteries, including internal carotid arteries, may be injured by neck manipulation, stroke attributed to trauma caused by neck manipulation is usually the result of vertebral artery dissection that occurs in the atlanto-axial area of the cervical spine. Undetected disease in vertebral or carotid arteries, or malformation in the network of vertebral and internal carotid arteries in the base of the skull (Circle of Willis supplying blood flow to both posterior and anterior portions of the brain), may increase risk of injury caused by upper neck manipulation ─ providing good reason to avoid or question use of any neck manipulation that might involve extreme rotation of the head or the upper cervical vertebrae.
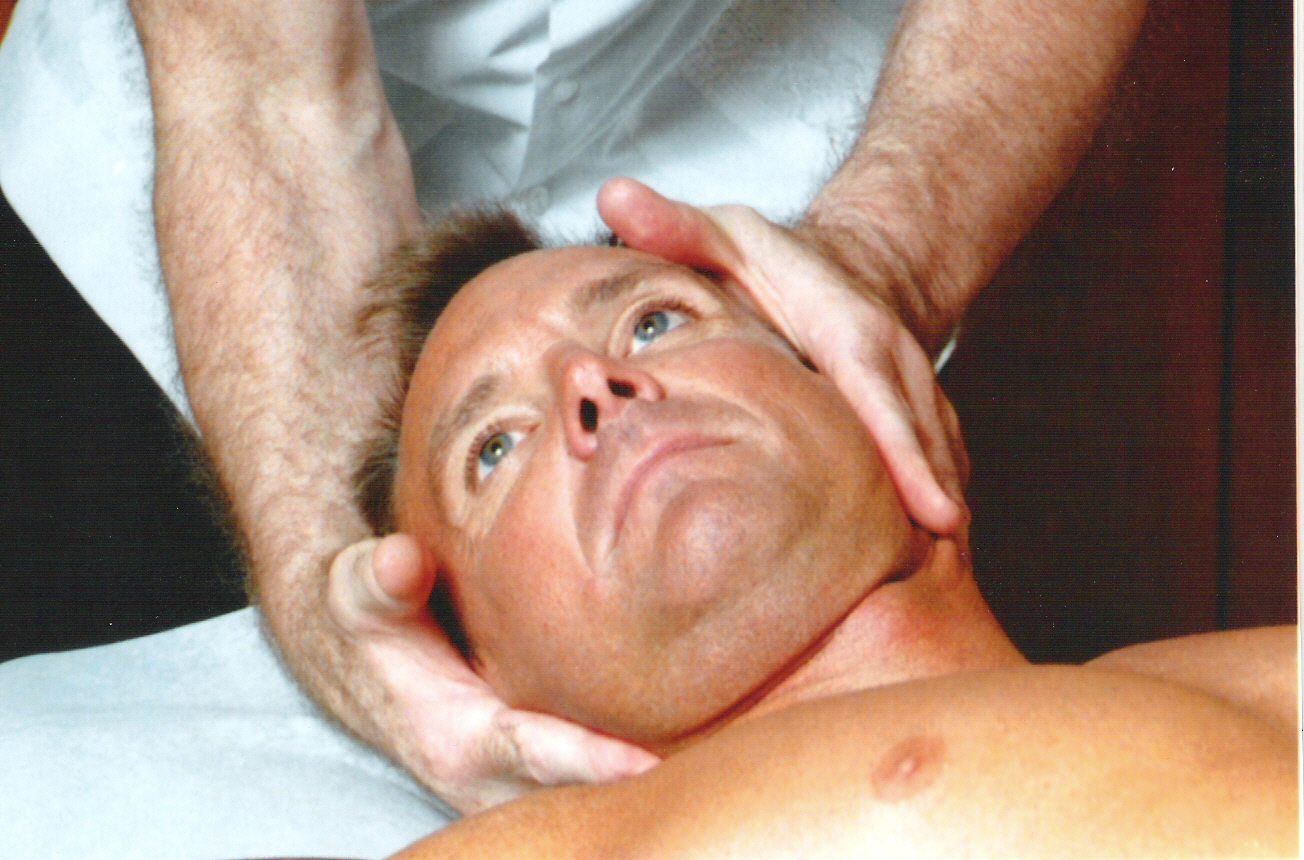
Head rotation that forces extreme rotation of the occipital-atlanto-axial joints stretches vertebral and internal carotid arteries. (Photo by Homola. Model: George Fleming.)
Stroke believed to be caused by neck manipulation is largely unrecognized and under reported. Estimates of the incidence of vertebrobasilar stroke associated with neck manipulation vary greatly. Since there is no system in place that identifies and registers reports associating neck manipulation with stroke, the true incidence of this injury is not known. Until chiropractors, physicians, physical therapists, and insurance carriers are required to report manipulation-related stroke data to an independently operated data base, it will not be possible to determine how many strokes might be caused by neck manipulation.
Upper cervical anatomy: A review worth repeating
The anatomy and the configuration of the atlanto-axial structures that provide an osseous pathway for vertebral arteries clearly indicate that extreme rotation of the upper cervical spine has the potential to damage vertebral arteries that supply blood to the posterior portion of the brain. The degree of risk depends largely upon the degree of rotation of the atlas on the axis ─ a risk that may be compounded by diseased vertebral arteries, connective tissue disorders, or structural abnormalities that are not often apparent, such as a retrolenticular vertebral artery ring or a bow hunter’s band.
The greatest amount of rotation in the cervical spine occurs in the atlanto-axial joints (which can rotate independently up to 50 degrees right and left) in the upper cervical spine where vertebral arteries are most often injured. There are no interlocking joint surfaces and no intervertebral disc to limit rotation of the atlas on the axis, which is restrained primarily by ligaments. When rotation of the atlas exceeds 45 or 50 degrees, vertebral arteries threading through transverse processes on each side of the axis and atlas (making a double U-turn to enter the foramen magnum in the base of the skull) are stretched, risking stroke caused by vertebral artery dissection or clot formation.
Since vertebral arteries on each side of the neck thread up through transverse processes from the sixth cervical vertebra to the first cervical vertebra, they are not exempt from stress at any level in the cervical spine during neck manipulation and may be vulnerable to injury if they are atherosclerotic or diseased. There is also a possibility that stroke might occur if neck manipulation releases an atherosclerotic plaque in a carotid artery.
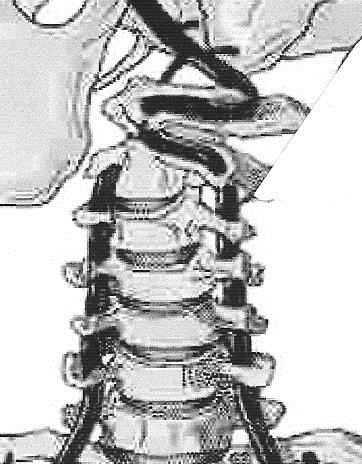
Vertebral arteries passing through foramina in the cervical vertebrae are subject to stress when head and neck rotation is extreme, especially in the upper cervical area where vertebral arteries take a tortuous route to enter the base of the skull.
Making an informed choice
There are many published studies dealing with the role of neck manipulation as a possible cause of stroke. Some of these studies, mixing science with pseudoscience, deny that neck manipulation can be a cause of stroke. Most of us prefer to rely upon scientifically oriented systematic reviews (such as Cochrane) and studies prepared by mainstream groups such as the American Stroke Association for credible conclusions. “Cherry picking” in a search for science-based articles on the subject of neck manipulation and stroke will invariably reveal that the preponderance of evidence strongly suggests that neck manipulation can be a factor in the development of vertebrobasilar stroke.
There is evidence to indicate that neck manipulation can be an effective treatment for some neck-related problems, such as cervicogenic headache. But when you consider reviews providing evidence that neck manipulation can be a cause of stroke, it appears that the safest and most logical course to take would be to avoid use of neck manipulation and turn to safer, equally effective methods of conservative care. An intractable neck-related problem (such as loss of mobility) that might benefit from neck manipulation should be subjected to a multidisciplinary risk-versus-benefit review to determine if use of manipulation is warranted and if the manipulative technique is appropriate. The technique used should not force extreme rotation in the atlanto-axial joints.
There are certain obvious signs and symptoms that preclude use of neck manipulation, such as carotid bruits or symptoms of vascular insufficiency on rotation or extension of the cervical spine. But there is no reliable way to determine that neck manipulation is a safe procedure, especially upper neck manipulation. Persons with no apparent risk factors or symptoms may have undetected vascular or structural abnormalities that predispose them to stroke caused by manipulating the cervical spine. Good health does not offer protection from injury to a cervical artery – as discussed above, neck manipulation is the leading cause of stroke in young (and therefore likely healthy) patients.
The neck pain problem
Neck pain has been ranked as the 4th leading cause of disability. Although mechanical-type neck pain is commonly treated by manipulating the cervical spine, questions remain about the effectiveness and the danger of such treatment. Neck pain (when not mechanical in nature) can be a symptom of spontaneous vertebral artery dissection ─ an obvious red flag when accompanied by any one of a number of neurological signs and symptoms.
Some studies have reported that spinal manipulative therapy for relief of mechanical-type neck pain is more effective than no treatment or sham treatment and more effective than medication but no more effective than exercise. While many people seem to benefit from manipulation or mobilization that provides short-term relief for neck pain or tension-related symptoms, the risk of stroke would certainly outweigh such benefit. Persons who may find it difficult to give up neck manipulation as a treatment for chronic neck pain should at least try other treatment options such as massage, traction, hydrotherapy, exercise, and so on.
According to a 2015 Cochrane systematic review, no high quality evidence has been found to remove uncertainty about the effectiveness of mobilization or manipulation as a treatment for neck pain. This observation supports contentions that neck manipulation as a treatment for neck pain has no proven benefit that outweighs the risk of stroke ─ as suggested by a team of physicians 14 years ago:
In the absence of randomized controlled trial evidence demonstrating the effectiveness of cervical manipulation, the best current evidence suggests that the small risk of dissection and stroke outweighs the benefit of this treatment modality for patients with acute neck pain.
Conclusion: Informed consent requires information
Although controversy continues to surround the use of cervical spine manipulation and its potential to cause stroke by injuring a vertebral or internal carotid artery, there appears to be no doubt that neck manipulation can be a cause of stroke. As suggested by the American Stroke Association, informed consent should be a prerequisite for neck manipulation. Some manual therapists choose to avoid the “fear factor” by not asking for informed consent when providing neck manipulation if the patient appears to be healthy ─ an approach that fails to consider that some patients may have undetected vascular or structural abnormalities that predispose them to manipulation-related injury. Besides, in many cases, strokes that have occurred in young people following neck manipulation have been shown to be the result of injury to a healthy vertebral artery.
Stroke caused by manipulating the cervical spine is a rare but devastating event. When there is any doubt about the need or the safety of neck manipulation, it is always best to forego such treatment and to consider other treatment options ─ a decision requiring that the patient as well as the provider be well informed about the risk involved.