{kind=link}
Not all cancers affect all populations equally. Liver cancer is the fifth-most common cancer worldwide, but the prevalence varies widely. Liver cancer cases skew heavily to less developed regions of the world, where 83% of cases are found – it’s over six times more common there than in Northern Europe, for example. In Asia, the high rates of liver cancer have been linked to hepatitis B and C, which is widespread, and a proven cause of cancer. And liver cancer continues to strike Asian American and Pacific Islanders more than any other American ethnic group as well, where hepatitis continues to circulate in the population. Now there’s new evidence to suggest that a substance found in some traditional Chinese medicines may also be causing liver cancer. They’re called aristolochic acids, and they illustrate, with a substantial body count, that what’s natural isn’t necessarily healthy or good.
What are Aristolochic acids?
In the early 1990’s a strange cluster of acute, end-stage renal disease appeared in women in Belgium. It was determined that all had been exposed to the chemical aristolochic acid (AA) at a weight loss clinic, due to the consumption of Chinese herbs which contained natural AA. Approximately one third of the more than 300 cases have subsequently required a kidney transplant, and cancers of the urothelial tract in this group have also been widespread. In the Balkans, low level exposure to AA via flour consumption that contains seeds from Aristolochia clematitis is believed to be responsible for what is now called Balkan-endemic nephropathy. Subsequent study that was initiated after the Belgian case identified that that AA is responsible for tumour development and for activating destructive fibrotic changes in the kidney. For over a decade now it has been well established that AA is a nephrotoxin and a powerful carcinogen with a short “latency period”, in that it causes permanently damage, quickly. What’s remarkable is that none of this was known until the 1990s despite “thousands of years” of use as a traditional medicine. As Steven Novella noted in a past post on aristolochic acid and urinary tract cancer:
This example just highlights the fact that widespread use of an herbal product, or any treatment, is not sufficient to ensure that it is safe, or even that it is effective. Common use may be enough to detect immediate or obvious effects, but not increased risk of developing disease over time. That requires careful epidemiology or specific clinical studies. We know about the risks of prescription drugs only because they are studied, and then tracked once they are on the market. Without similar study and tracking there is simply no way to know about the risks of herbal products. Relying upon “generally recognized as safe” is folly.
While herbal remedies that contain AA are now banned in many countries, AA-induced kidney damage and related cancers continues to appear worldwide. As AA’s cancer-causing effects have now been widely studied, the distinct way that they damage cells has been described as a sort of “signature” that is easily identifiable in tumour samples. This brings us to this new study of liver cancers attributed to AA, which have been less closely associated with AA. This study used that unique “signature” to look for AA exposure.
Aristolochic acids and liver cancers
There is good evidence to show that the consumption of AA-containing products in Taiwan has been widespread through the use of prescribed herbal medicines. The paper is entitled “Aristolochic acids and their derivatives are widely implicated in liver cancers in Taiwan and throughout Asia” and it’s from Alvin Ng and associates, published in Science Translational Medicine in October, 2017. This was a retrospective analysis of hepatocellular carcinomas (HCC, liver cancer in lay terms) and patients were included if they (1) had true HCC (2) there was sufficient DNA available from a sample of the tumour. 98 HCCs from Taiwan hospitals were studied based on whole-exome sequencing and mutation identification. They looked for the distinctive way in which AA causes mutations. The researchers subsequently examined 1,400 HCCs from other regions in the world. The final analysis was as follows:
- Taiwan: 78% of tumours had evidence of AA exposure
- China: 47% of tumours had evidence of AA exposure
- Southeast Asia: 29% of tumours had evidence of AA exposure
- Korea: 13% of tumours had evidence of AA exposure
- Japan: 2.7% of tumours had evidence of AA exposure
- North America: 4.8% of tumours (in one hospital, 22% of 87 patients, all of Asian ancestry, had evidence of AA exposure)
- Europe: 1.7% of tumours had evidence of AA exposure
Here is the global breakdown, with the red portion illustrating the proportion of tumours that were linked to AA exposure:
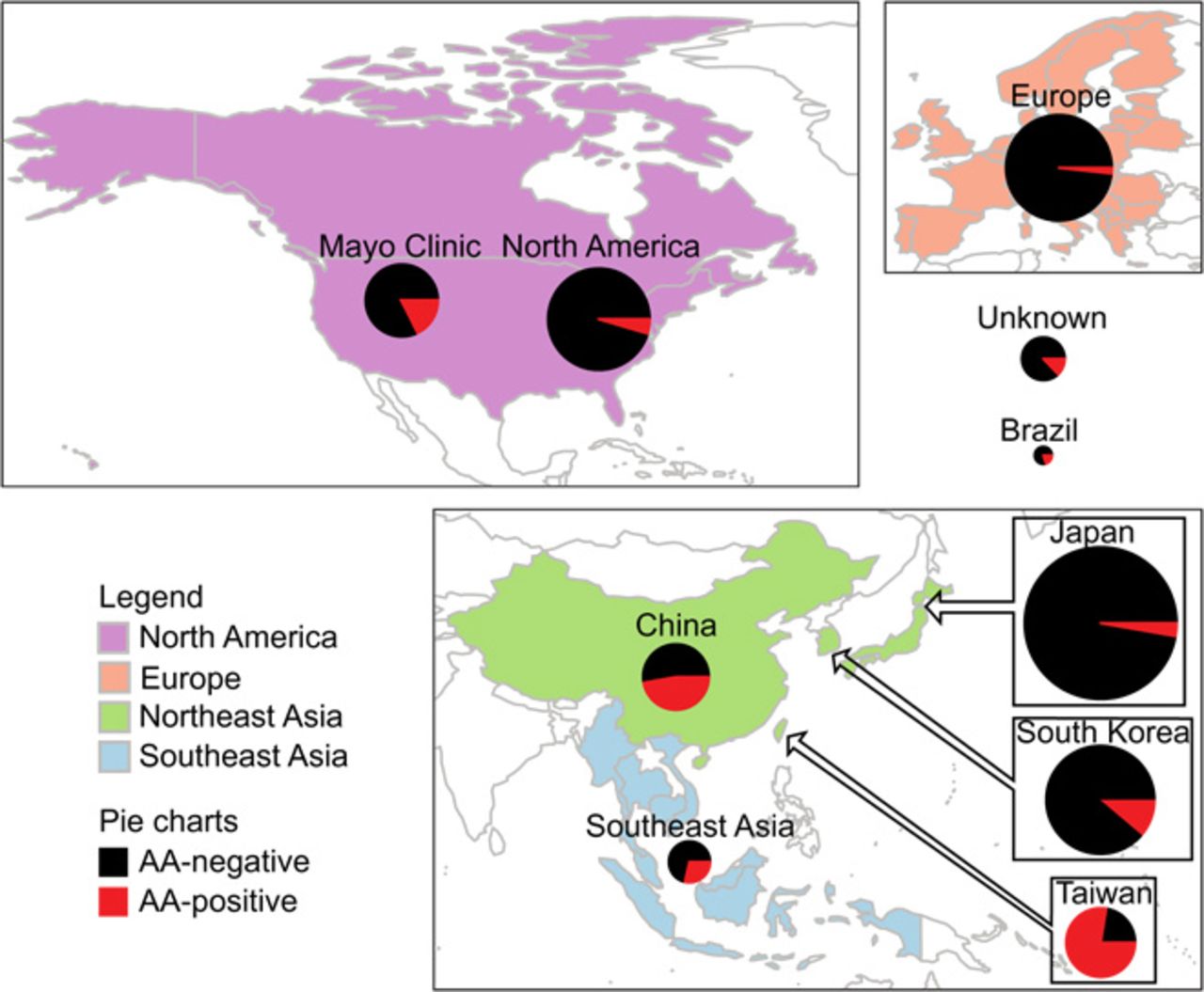
Global distribution of mutagenesis associated with aristolochic acid and derivatives in liver cancer.
Reducing your risk of kidney and liver cancer
Herbal remedies are popular worldwide. In China and other countries in Asia, there is strong support for, and belief in “traditional” Chinese medicine despite the fact that it is neither truly traditional (as it is now promoted), nor particularly effective. This new analysis shows that the use of (or exposure to) AA is widespread in some parts of the world, and appears to be be a cause in a substantial numbers of liver cancers. The authors noted that the presence of AA-associated cancer does not appear to be declining in Taiwan, despite the banning of some AA-containing herbs in 2003. This may be due to a lag effect (like cancer and smoking) but may also be due to continued exposure to, or consumption of, AA-containing products.
If you’re a user of traditional Chinese medicine, avoiding AA is easier said than done, unless you have impeccable knowledge of herbs, their origins, and the supply chains you’re getting your products from. I’ve blogged before about TCM, noting that contamination is common. Mislabelling of products also appears to be widespread, suggesting that rigorous and credible testing of final products may be the only way consumers can be assured they’re avoiding AA in the products they buy. The linkage of AA to kidney damage, and the evolving story of its cancer-causing potential illustrates that even widespread use of a product for hundreds (or thousands) of years give no automatic assurance of safety. If it were not for the Belgian weight loss clinic kidney failure cluster, the widespread toxicity of AA may not even be known today.