
{kind=link}
A (seemingly) long time ago in a galaxy (seemingly) far, far away, a Johns Hopkins cardiologist named Dr. Joseph Marine wrote a(n) (in)famous post for the inaptly named Sensible Medicine blog entitled Why Doctors Should Learn to Stop Worrying and Love MAHA. MAHA, for those who haven’t been paying attention, stands for “make America healthy again,” a slogan co-opted by our current Secretary of Health and Human Services Robert F. Kennedy Jr. in 2024 after he had suspended his Presidential campaign and bent the knee to Donald Trump in return for a promise of power, should Trump win the election and become President again. Unfortunately for medicine, public health, and science, Donald Trump did win again, and RFK Jr. soon became what I described at the time as an extinction-level threat to public health. Nothing that has happened since I first described the threat posed by this administration to science and public health as “extinction-level” has led me to believe that I was exaggerating or being histrionic at the time; quite the contrary, in fact. If anything, I lacked the imagination in 2024 to see just how far this administration would go in dismantling everything good about US federal science programs, such as, for example, the National Institutes of Health, where Lysenkoism 2.0 is about to be codified into federal regulations.
So, given the dismantling of peer review at the NIH in favor of political control of grantmaking decisions (with some MAHA advocates even calling for “abolishing the NIH“), the systematic attack on US vaccination programs at the Centers for Disease Control and Prevention and the Food and Drug Administration, and the wholesale assault on evidence-based policy, it’s natural to wonder, as SBM contributor Dr. Jonathan Howard has, whether Dr. Marine is still supportive of MAHA or can continue to defend his original post, given what has happened since Trump became President again, which led to this conversation on X, the platform formerly (and better) known as Twitter:
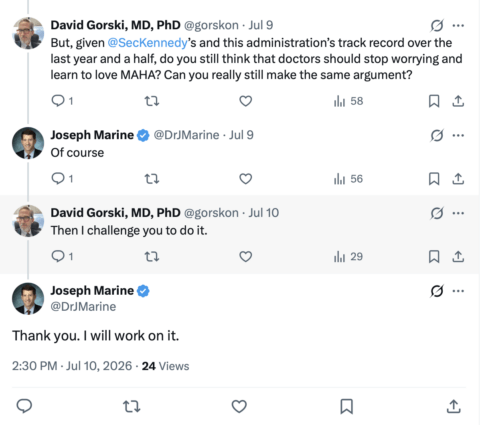
Unfortunately, as of yesterday he had not produced his arguments. However, that doesn’t mean that, while we’re waiting, I can’t look at something that Dr. Marine did write last week for the Brownstone Institute, which rose to prominence during the pandemic as a far right wing anti-public health project of one Jeffrey Tucker that has become one of the primary propaganda wings of the populist, anti-expertise wing of the “make America great again” (MAGA) movement, entitled How to Make the CDC Great Again. Besides, I’m sure that Dr. Howard will be able to handle whatever apologia that Dr. Marine ultimately comes up with for MAHA. In the meantime, as the title of this blog post implies, I’m suffering whiplash between the Dr. Marine of 2024 chastising doctors (like me and the rest of the SBM crew) for worrying about what MAHA would do with Donald Trump and RFK Jr. in power to now proposing how to make the CDC great again, as I said on X:
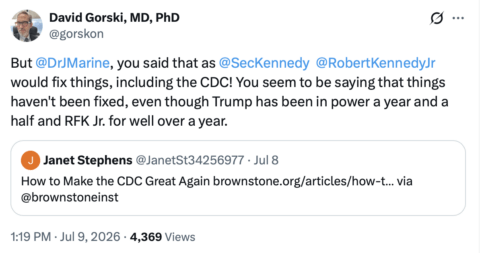
See what I mean? Dr. Marine is saying that we need to make the CDC great again (whatever that means), but Trump has been in power a year and a half? Why isn’t the CDC great again, or at least clearly making progress towards being great again? Even if “making CDC great again” is a long-term project, you’d think that a year and a half would be enough time to get at least a decent start on it, wouldn’t you? (I would.)
My whiplash aside, I think it’s instructive to look at what Dr. Marine actually wrote, to compare it with what’s actually happened since January 20, 2025, and then with what Dr. Marine wrote about MAHA in 2024, to see how it all squares up.
Ethics, censorship, and a MAHA apologist
Dr. Marine begins his article by letting the reader know that he is a Very Important Person Indeed and, in fact, was under serious consideration to be the Director of the CDC. To a science-based physician like myself, that admission tells me just how bad the situation is at CDC, as Dr. Marine is a cardiologist. Indeed, he subspecializes even more than cardiology; he’s an electrophysiologist, which is the branch of cardiology concerned with heart rhythm disorders, such as atrial fibrillation. There is nothing in his biography or background that suggests that he is the least bit qualified to be CDC Director. He does, however, have an impressive number of publications listed on PubMed. I’ll give him credit for that; he has five times the number of publications that I do, and he’s considerably younger than I am. Unfortunately, none of his publications seem to indicate expertise in public health, vaccinology, or infectious disease, although he did get a comment published in the New England Journal of Medicine in 2023 about a study looking at universal masking of children in school that showed an association between lifting mask mandates in schools in Boston with increased incidence of COVID-19 among students and staff. Naturally, Dr. Marine blamed unaccounted-for confounding.
In any event, let’s see how Dr. Marine leads off:
A few months ago, I was one of several candidates under consideration for Director of the Centers for Disease Control and Prevention (CDC). While I did not make the final cut, I was honored to be considered for such an important position. The administration has nominated a highly qualified team to lead the CDC and I wish them well. The experience gave me the opportunity to reflect on what reforms I would like to see at the CDC as it faces a pivot point in the history of medicine and public health. Here are six themes that I see as most important and urgent.
Again, that the administration would even consider Dr. Marine for CDC Director tells me just how little subject-specific expertise is valued by this administration. That makes the ultimate choice of the administration to be CDC Director all the more surprising, and in an actually pleasant way. Indeed, in this one case the administration did choose a much better—and, shockingly, more conventional—candidate to run the CDC, Dr. Erica Schwartz:
Schwartz holds multiple academic credentials, including both medical and law degrees. Her career has largely been spent in military uniform, including in a leadership position at the U.S. Coast Guard where she oversaw the organization’s system of 41 clinics and 150 sick bays.
She later served as deputy surgeon general, where she helped lead uniformed medical and health professionals posted at the CDC and government health agencies that serve the general public.
It almost makes me wonder if RFK Jr. had anything to do with this selection, given that Dr. Schwartz has relevant experience and is not a crank. Indeed, it amused me to see that everyone’s favorite antivax lawyer, Aaron Siri, was most displeased when Dr. Schwartz’s nomination was announced:
But Aaron Siri, a lawyer and ally of Kennedy in attacking vaccines and pharmaceutical companies, criticized Schwartz’s selection. In a social media post, Siri lambasted Schwartz’s past promotion of vaccinations and said “she lacks the basic ethics and morals to lead the CDC.”
I don’t know a lot about Dr. Schwartz, but if Siri doesn’t like her, the worst that can be said about her is that she isn’t all bad, while the best is that she is a real public health official and expert and, equally important, not an antivax crank.
But back to what Dr. Marine thinks to be required to “make CDC great again.” I’m going to take the liberty of jumping to one specific issue that he brings up, because it is the most egregiously out of touch with reality. It is the one that shows either his utter obliviousness to what has happened the last year and a half or his utter disingenuousness. (Take your pick.) This item comes as a bullet point under the first “theme” that Dr. Marine advocates. That theme states:
Develop a new ethical framework for public health practice. Too often during the pandemic, policies were justified by the intended effects with little attention paid to the means used to reach those ends. The Hippocratic Oath and its modern derivatives have served as that ethical framework for medical practice for over 2,000 years and they have made the health professions (until recently) one of the most trusted institutions in our society. Public health practice needs its own version and should adopt many of its principles…
I rolled my eyes at this, as you might imagine. Public health is a branch of medicine. Many of the people who administer public health are physicians who have taken the Hippocratic oath or one of its updated modern variants. Moreover, at this point, Dr. Marine is just regurgitating standard COVID contrarian talking points that falsely claim that public health officials never considered the consequences of the means they used to try to contain COVID-19. I’ll get back to that in a minute, but let me jump down to the eighth bullet point under this theme:
Renounce and combat censorship. For the public to trust statements of public health officials, they must believe that contrary viewpoints can be publicly expressed and debated in the marketplace of ideas. Suppression of those viewpoints by government actors may feed public mistrust and may suggest that they are receiving an illusory consensus and propaganda rather than the best available information. A previous administration embraced the dubious idea that “misinformation” was a “public health threat” and a “leading cause of death.” The new public health framework must treat contrary viewpoints with respect and encourage open dialogue.
We can all agree that censorship is generally a bad thing in a democracy. On the other hand, accepting that principle doesn’t mean that spreading misinformation is or should be without consequences. After all, misinformation spreaders take advantage of the freedom of speech that our constitution ostensibly grants citizens in order to promote their pseudoscience, conspiracy theories, and disinformation as having equal purchase in the public dialogue with science-based facts, policies, and opinions, all while proclaiming themselves as victims of “censorship” if they face any sort of pushback or consequences for exercising their freedom of speech to spread misinformation. When Dr. Marine calls for treating “contrary viewpoints with respect and encourage open dialogue,” I like to ask him what contrary viewpoints he’d treat with “respect” in his specialty. For instance, does he think homeopathy can effectively treat atrial fibrillation? Should the viewpoint making that claim be treated with “respect,” particularly when the person making that claim is selling homeopathic products to treat atrial fibrillation? After all, homeopathy is basically water, and using it to treat atrial fibrillation is the same as not treating the atrial fibrillation at all. People could have strokes and even die as a result of untreated atrial fibrillation. I don’t want to harp on this point too much, as I’ve discussed it more times than I can remember. This call for “respect” and “open dialogue” is almost never anything more than a call to treat pseudoscience, conspiracy theories, and misinformation as worthy of being “debated” on the same plane as science-based medicine.
Instead, I want to point out something that Dr. Marine doesn’t mention at all and, as far as I know, has not mentioned anywhere, namely: If he’s so much against “censorship,” then why is he so chill with MAHA, given that the Trump administration has done more than any previous administration to silence scientists and punish those it doesn’t like, either by firing or making it impossible for them to obtain research grants? Let’s start with a topic that dominated my blog posts in June: what the current administration is doing at NIH. First of all, does Dr. Marine approve of the new rules proposed by OMB Director Russell Vought that would, in essence, relegate scientific peer review to an entirely advisory role in decisions over which research grant applications to fund while giving the power to fund or veto research grants entirely to political appointees, who have to be “aligned” with administration interests? (There’s still time for public comment, by the way, but you’ll have to act fast. The deadline is today.)
How about another example? Nature recently reported on how political screening is holding up the disbursement of NIH research grants, and what’s happening is really egregious and scary, as I discussed a couple of weeks ago. Does Dr. Marine consider this “censorship” by the government? If not, why not? Does he approve of political control of the research grant funding process? Before answering that question, he should remember that, even if he likes this particular administration’s politics, no administration lasts forever, and it is (still) quite possible that a Democrat will be elected in 2028—or even a Republican whose politics he doesn’t like. Does he feel comfortable given political appointees such granular control over what science gets funded?
That’s not all, though. Some of the new proposed rules would require federally funded scientists to seek permission to publish their results, suggesting that the administration could bar them from publishing results that it doesn’t like. Ditto if a scientist wants to present the findings of federally funded research at a scientific conference. Yes, these rules will require preauthorization by the government to present findings at a scientific conference. How are these two policies not censorship of scientists? If these rules pass, the power of the government to censor scientists and scientific findings will be permanently codified in the federal register and very difficult to change! I don’t see Dr. Marine being the least bit troubled by these issues; at least, if he is, I’ve seen no indication in his writings or social media posts that he’s the least bit troubled by this obvious government censorship. One wonders whether he’s fine with it because it’s his side doing the censoring, one does. Or maybe he just doesn’t know. What is the old saying? Oh, yes: There are none so blind as those who will not see, and, yes, this is happening now. For instance, Dr. Bhattacharya blocked the publication of a study from the CDC that showed that COVID-19 vaccines were effective and safe during the 2025-2026 winter respiratory virus season.
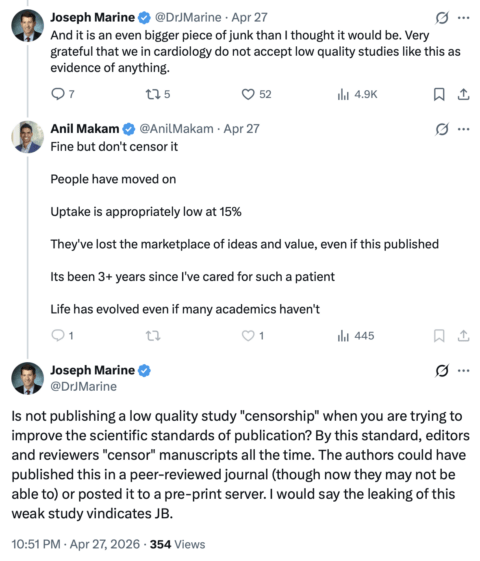
Of course, Dr. Marine was untroubled. Hilariously, in this thread on X, he basically dismissed the study as “a bigger piece of junk than I thought” but was unable to describe in any coherent detail what, exactly, were the shortcomings that led him to conclude that, despite being asked again and again, eventually just saying:
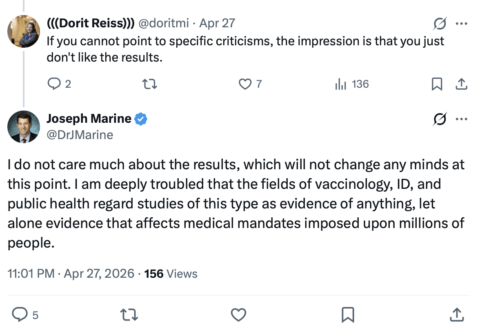
So, basically, Dr. Marine didn’t like the results and appears not to accept epidemiological studies as ever being sufficiently rigorous to guide public policy but, worse, doesn’t even care much about the actual results. Nor, apparently, does he care that the government blocked the publication of the results of government-funded and -administered science that had passed the usual longstanding pre-publication peer review steps required by the CDC before publication in its journal MMWR. Again, it’s difficult not to conclude that Dr. Marine is fine with the censorship of scientists, as long as it’s scientists he doesn’t like who are being censored and the censorship is being done by officials whose policies he does like. Indeed, he has resorted to a truly disingenuous argument:
Dr. Marine was so close to understanding why all the “censorship” against misinformation was not, in fact, truly censorship at all in any real sense of the world, but rather more akin to quality control and consequences for exercising one’s freedom of speech for spreading bullshit. Again, though, when establishment scientists do it, it’s “censorship,” and when people Dr. Marine likes do it, it’s “quality control.”
Perhaps even worse, the new culture of censorship by the medical, public health, and scientific authorities in the federal government is trickling down. Recently, the American Diabetes Association called the police to kick out of their yearly scientific conference several prominent members of the organization who were doing nothing more provocative than quietly passing out reprints of an article critical of NIH Director (and acting CDC Director) Dr. Jay Bhattacharya, an op-ed that had originally been published in the official journal of the ADA! Then it banned them from attending the rest of its official proceedings. Does that not bother Dr. Marine? When the government censors and threatens punishment against critics, it’s not uncommon for some organizations to start obeying in advance. True, the ADA did ultimately apologize, and some heads among its leadership did roll, but that it ever served as the goon squad to enforce the administration’s censorship in the first place is very disturbing. I don’t recall Dr. Marine ever having said anything about that. I’m guessing that it doesn’t bother him.
Let’s just say I would take Dr. Marine a lot more seriously in his concerns about “censorship” if he weren’t so blatantly one-sided in his criticisms.
Yet, under his third theme, Dr. Marine asserts that we must do this:
Embrace diversity in political viewpoints. A Washington Examiner column just before the pandemic showed that >99% of political donations from CDC employees went to one political party. That is a major problem. A CDC which is too biased toward one political philosophy or set of viewpoints will not be able sustain long-term public support. While 50% + 1 may serve as a successful formula for electoral politics, it is a prescription for failure in public health policy, which necessarily blends science with public policy. A public health approach which does not account for a range of political viewpoints will not be able to garner the broad public health necessary for successful implementation, particularly in times of crisis. CDC leadership must examine how certain political viewpoints have been systematically excluded from the CDC and the field of public health and work to broaden the base of political perspectives within the field.
Can Dr. Marine honestly say that the CDC—or NIH or FDA or any agency in HHS, for that matter—is “embracing diversity in political viewpoints”? Again, one of the great bugaboos of this administration is the dreaded “DEI” (diversity, equity, and inclusion), and Trump is actively trying to crush any vestige of DEI anywhere. At the NIH (again), even mentioning anything that sounds as though it might be even tangentially related to DEI is being suppressed. It is indeed rich that Dr. Marine complains about the pre-Trump 2.0 CDC “systematically excluding” certain political viewpoints from the CDC but says nothing about how Trump’s OMB Director Russell Vought trying to codify the exclusion of scientific and political viewpoints from HHS agencies that don’t “align with administration priorities.”
On a related note, as far as respecting diversity of scientific opinion, I would point out that Trump’s first CDC Director, Susan Monarez, was fired because she wouldn’t unquestioningly go along with RFK Jr.’s plans to change the vaccine schedule. Basically, she refused to go along with RFK Jr.’s attempts to promote unscientific and pseudoscientific policies at the CDC and would not fire the people he wanted her to fire. Her firing led to a mass resignation of several key CDC managers. Moreover, there are many reports out there that RFK Jr. does not consult with or listen to scientists with expertise in vaccines, infectious disease, epidemiology, and public health policy, preferring instead his own stable of cranks and quacks, some of whom he’s elevated to high positions in the CDC, FDA, and NIH. Does Dr. Marine think that RFK Jr. should listen to scientists who might disagree with him?
He claims to in one of his bullet points:
Consideration of expertise of others: Public health is also public policy, not just science. A public health program must include expertise in economics, childhood development, psychology, and other fields which are not part of formal public health training. Dr. Fauci famously disclaimed responsibility for understanding the economic and social consequences of pandemic policies as being outside his field of concern. This attitude is not acceptable in medicine or surgery, where practitioners are expected to fully understand the consequences of the treatments that they recommend. It should not be acceptable in public health practice.
Let’s just say that this is not a fair representation of what Dr. Fauci actually said. It’s a paraphrase of a Fauci quote that appears to have originated in an article in Reason commenting on an interview Dr. Fauci gave the New York Times. Here is what he actually said:
I certainly think things could have been done differently — and better — on both sides. I mean, anybody who thinks that what we or anybody else did was perfect is not looking at reality. Nothing was done perfectly. But what I can say is that, at least to my perception, the emphasis strictly on the science and public health — that is what public-health people should do. I’m not an economist. The Centers for Disease Control and Prevention is not an economic organization. The surgeon general is not an economist. So we looked at it from a purely public-health standpoint. It was for other people to make broader assessments — people whose positions include but aren’t exclusively about public health. Those people have to make the decisions about the balance between the potential negative consequences of something versus the benefits of something.
Certainly there could have been a better understanding of why people were emphasizing the economy. But when people say, “Fauci shut down the economy” — it wasn’t Fauci. The C.D.C. was the organization that made those recommendations. I happened to be perceived as the personification of the recommendations. But show me a school that I shut down and show me a factory that I shut down. Never. I never did. I gave a public-health recommendation that echoed the C.D.C.’s recommendation, and people made a decision based on that. But I never criticized the people who had to make the decisions one way or the other.
This is not an unreasonable stance. The purview of the CDC is public health, not economics, although the two can intersect. In a functioning government, the CDC would give its recommendations based on public health science, while, for instance, the job of analyzing the economic impact of the recommendations would fall to the Council of Economic Advisors and maybe the Departments of Treasury and Commerce, who would not be expected to comment on the scientific and public health recommendations. It would then be up to the President and the Cabinet, along with Congress, to weigh these recommendations and act upon them, balancing the costs with potential benefits. Dr. Marine is demanding that the CDC undertake a task that it is ill-equipped to do simply because he didn’t like the policies pursued by the first Trump administration and then by the Biden administration to control the pandemic. Dr. Marine’s other claim that “US pandemic leaders paid little or no attention to the massive collateral damage caused by policies focused exclusively on preventing every possible Covid infection” is also utter nonsense, nothing more than the usual claims that we’ve been hearing since 2020. In reality, he’s referring to one interview with former NIH Director Francis Collins, who said:
If you’re a public health person, and you’re trying to make a decision, you have this very narrow view of what the right decision is, and that is something that will save a life. Doesn’t matter what else happens, so you attach infinite value to stopping the disease and saving a life. You attach zero value to whether this actually totally disrupts people’s lives, ruins the economy, and has many kids kept out of school in a way that they never might quite recover from. Collateral damage. This is a public health mindset. And I think a lot of us involved in trying to make those recommendations had that mindset — and that was really unfortunate, it’s another mistake we made.
I would, of course, argue that this statement from Dr. Fauci rather belies Dr. Marine’s second theme, that we should “learn the mistakes of the COVID pandemic response.” No one—and I mean no one—argues that we shouldn’t critically study the pandemic response, what went wrong, what went right, and what were the unintended consequences. Only someone who hasn’t been paying attention to the medical literature or what public health officials have been saying over the last couple of years could so blithely claim that there “is too little of this happening on university campuses. The CDC could set the example for how to undertake this kind of reexamination, opening the door for more open discussion and debate in universities and other scholarly venues.” I mean, seriously. There has been a huge effort to understand what went wrong (and what went right) during the COVID public health response. Given the Brownstone Institute obsession with “lockdowns” as the root of all COVID evil, I can’t resist citing a systematic review of the unintended consequences of lockdowns from 2024 that examined a total of 132 studies on this issue and found, among other things, detrimental effects on mental health, obesity-related, and health-related social need outcomes. Another scoping review looked at the failures of the World Health Organization response. The research is being done. I myself made a modest contribution to this effort by co-authoring a study on the inaccuracies in the early seroprevalence studies. It’s not being swept under the rug. However, it serves the MAHA narrative that “They” won’t admit any error and that “They” are “hiding” the evidence of harm from lockdowns. If anything, the unrelenting hostility of MAHA to science-based public health will hamper a sober assessment of failures and successes managing the pandemic.
I’m underwhelmed by the rest
The rest of the bullet points under this new “ethical framework” in Dr. Marine’s first theme similarly read like the usual right-wing talking points and claimed victimhood of those who spread misinformation and portrayed any pushback as “censorship” or “persecution.” Let’s take a look at the rest of them briefly. First, Dr. Marine demands “respect for individual rights,” stating that public health practice in the US “must be consistent with our legal framework, traditions, and Constitution, including the Bill of Rights.” (I’m not sure where public health practice was not consistent with the Bill of Rights; Dr. Marine doesn’t give examples.) He also demands “free, voluntary, and fully informed consent for any medical or preventive treatment,” as if that were not already a principle of medical practice. Of course, how you define “informed consent” is very important, and Dr. Marine appears to be either ignorant of or intentionally ignoring a longstanding strategy of the antivax movement that I like to call “misinformed refusal.” What I mean by this term is how antivaxxers try to include in the “informed consent” nonexistent “risks” from vaccines, such as autism and sudden infant death syndrome, all while downplaying the vaccine effectiveness. The fact is, informed consent is already a bedrock principle of medical practice. What antivaxxers and COVID contrarians like Dr. Marine don’t like is that doctors are not required to include fantastical risks in their discussions with patients.
Dr. Marine also pontificates about “acknowledging uncertainty” and, later, “embracing nuance.” I laughed out loud when I read that, especially his admonition to be “careful not to draw overly broad or definitive conclusions, especially from studies of weaker design.” I mean, that’s what MAHA is all about, making overly broad and definitive conclusions from studies of incredibly weak design and execution. We’ve been documenting that sort of thing here for a long time, for example here. I can’t help but point to Dr. Marty Makary claiming that medical errors are the third leading cause of death based on a study he did of such breathtakingly poor quality that it was basically an insanely unjustified extrapolation from tiny numbers to the whole country. I would argue that neither Dr. Makary nor MAHA acknowledged the uncertainty about that estimate.
Other recommendations include improving the rigor of science and data quality, which is a recommendation that no one disagrees with. The devil, of course, is in the details of what exactly is meant by this. The current regime coined a term, “gold standard science,” that seems to mean whatever they want it to mean. Dr. Marine bemoans “weak” studies being used to drive public policy during the pandemic, and that did in fact happen. However, as much as I hate to quote former Defense Secretary Donald Rumsfeld, “You go to war with the army you have, not the army you might want or wish to have at a later time.” In 2020, COVID-19 was a new virus, and not a lot was understood about it, other than what we already knew about coronaviruses. The virus was washing over the world, and waiting for better data was not an option. Later in the pandemic, after there had been time to do better studies, then, yes, we should encourage better evidence and only act on the highest quality evidence. Unfortunately, not mentioned by Dr. Marine is how this administration’s gutting of the NIH and CDC, its ideological purity tests to receive scientific funding, and its willingness to censor and punish scientists who do not toe the administration line are not setting up the infrastructure to generate the highest quality evidence to help us forestall the next pandemic or to deal with it when it eventually comes.
Finally, the pièce de résistance:
Put infectious disease in context and embrace MAHA. In most years, infectious disease barely makes the top 10 causes of death in the US but plays an outsized role in public health policy and practice. The Make America Healthy Again (MAHA) movement has questioned a medical and public health establishment that has focused obsessively on the prevention of a few rare infectious diseases while largely ignoring environmental root causes of declining population health. Reconciliation can come through embrace of the key elements of the MAHA movement and incorporation into public health practice and CDC policy. Building a healthier population is an important component of pandemic prevention and mitigation. The CDC has an underutilized National Center for Chronic Disease Prevention and Health Promotion. The Center could be repurposed, reinvigorated, and redirected to facilitate this new preventive health agenda.
Of course, what MAHA (and Dr. Marine) neglect to mention is that a big part of the reason that infectious diseases are not among the top causes of death in the US anymore is because of a strong public health infrastructure and, yes, because of vaccinations. Basically, what Dr. Marine appears to be doing is parroting in a different form RFK Jr.’s proposal in 2023 during his ill-fated Presidential campaign that he would tell the NIH to “give infectious disease a break for about eight years.” While it is true that chronic disease can increase susceptibility to infectious disease, MAHA always overplays what “building a healthier population” can do in terms of resistance to infectious disease. After all, the one historical counterexample is the 1918 influenza pandemic, which originated in the US in army barracks full of healthy young men and tended to kill the young.
In any case, while one can make arguments for and against the contention that we haven’t paid sufficient attention to chronic disease, public health is all about the “environmental root causes” of disease and declining population health. In fact, the interest in the environmental causes of disease is about the only good thing that MAHA might offer. I say “might” because MAHA tends to exaggerate and to identify “environmental causes” not supported by science, such as all the horrors that it attributes to vaccines, including autism, neurological diseases, autoimmune diseases, cancer, and more. Basically, all Dr. Marine is doing here, whether he realizes it or not, is paraphrasing a common antivax trope that claims that healthy people don’t get sick from infectious diseases and that children who die of, for example, measles cannot have been healthy and must have had an underlying health condition. There’s a reason why I refer to MAHA as “soft eugenics” or social Darwinism. Seriously, Dr. Marine seems to think that the social determinants of health are actually important, and for that, if for little else, I applaud him. However, that makes his embrace of and apologetics for MAHA, which does its best to promote a highly individualistic, “health hacking” view of health that denies or downplays the social determinants of health, wildly discordant.
Dr. Marine is clearly a skilled cardiologist and well-published academic physician. In fact, it is that very career history that makes him a particularly good cautionary tale warning how none of that is sufficient to protect one against going down the rabbit hole, be it the rabbit hole of MAHA or other conspiracy theories. He probably thinks that he’s taking a reasonable “middle ground” embracing MAHA because he agrees with its thesis that too much of the health system has been, as he originally put it, “corrupted by corporate interests that have become increasingly misaligned with the public interest.” Unfortunately, what he doesn’t see is that MAHA isn’t really doing anything about those corporate interests. Rather, it’s just adding the manufacturers of supplements, snake oil, and “functional medicine” quackery to big pharmacy interests, while peddling pseudoscience under the name of “gold standard science.”