{kind=link}
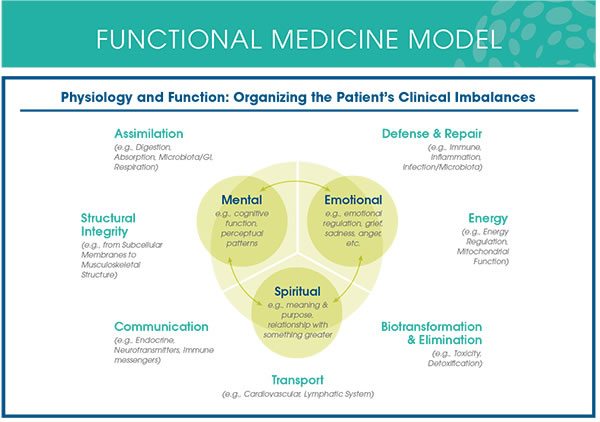
Functional Medicine practitioners like to make patients think that this diagram actually means something.
We at Science-Based Medicine often describe “integrative medicine” as integrating quackery with medicine (at least, I often do), because that’s what it in essence does. The reason, as I’ve described time and time again, is to put that quackery on equal footing (or at least apparently equal footing) with science- and evidence-based medicine, a goal that is close to being achieved. Originally known as quackery, the modalities now being “integrated” with medicine then became “complementary and alternative medicine” (CAM), a term that is still often used. But that wasn’t enough. The word “complementary” implies a subordinate position, in which the CAM is not the “real” medicine, the necessary medicine, but is just there as “icing on the cake.” The term “integrative medicine” eliminates that problem and facilitates a narrative in which integrative medicine is the “best of both worlds” (from the perspective of CAM practitioners and advocates). Integrative medicine has become a brand, a marketing term, disguised as a bogus specialty.
Of course, it’s fairly easy to identify much of the quackery that CAM practitioners and woo-friendly physicians have “integrated” itself into integrative medicine. A lot of it is based on prescientific ideas of how the human body and disease work (e.g., traditional Chinese medicine, especially acupuncture, for instance, which is based on a belief system that very much resembles the four humors in ancient “Western” or European medicine); on nonexistent body structures or functions (e.g., chiropractic and subluxations, reflexology and a link between areas on the palms of the hands and soles of the feet that “map” to organs; craniosacral therapy and “craniosacral rhythms”); or vitalism (e.g., homeopathy, “energy medicine,” such as reiki, therapeutic touch, and the like). Often there are completely pseudoscientific ideas whose quackiness is easy to explain to an educated layperson, like homeopathy.
Then there are modalities being “integrated” into medicine whose quackiness is not so easy to explain. Perhaps the most popular and famous of these is a specialty known as “functional medicine” (FM) whose foremost practitioner and advocate (in the US, at least) is Mark Hyman, MD, a man whose fame has led him to become a trusted medical advisor to Bill and Hillary Clinton. Perhaps Hyman’s greatest coup came in 2014, when the Cleveland Clinic Foundation hired him to create an institute dedicated to FM, an effort that has apparently been wildly successful in terms of patient growth. Never mind that around the same time Dr. Hyman teamed up with rabid antivaccine activist Robert F. Kennedy, Jr. to write a book blaming mercury in the thimerosal preservative that used to be in vaccines for causing autism, an idea that was shown long ago to have no scientific merit. Unfortunately, elsewhere FM has been pretty successful as well, to the point where there is even “functional dentistry.”
The problem with “functional medicine” is that at its core it is close to being as nonsensical as the more “obvious” forms of quackery. It just hides it better, given the number of fancy-sounding laboratory tests. It’s also incredibly difficult to pin down just what the heck it even is, as we’ve discussed many times in the past, starting with the late, great Wally Sampson’s plaintiff post, Functional Medicine: What Is It? It was a question he asked after referring to it as the “New Kid on the Block.”
That’s why I’m grateful to Jann Bellamy, who sent me a case study on the use of FM in oncology published in a journal that I had never heard of before, Integrative Medicine: A Clinician’s Journal (IMCJ). Even better, the case is a woman treated for breast cancer, my area of expertise, which allows me to discuss this in even more depth. Before we do that, let’s review a bit about FM as a prelude to diving into the specifics of this published case report. To be honest, I’m surprised that anyone would publish such tripe, as it’s incredibly embarrassing. Or at least it would be to any competent oncologist. What really scares me is that FM is now specializing. What we are seeing here is the birth of “functional oncology,” and it is terrifying to me.
Functional Medicine: What Is It?
I begin by asking the same question that Wally Sampson asked, lo those many years ago: Just what the heck is functional medicine, anyway? It has been a long time since any of us here has asked that question; so now is as good a time as any to ask it again. Indeed, I was curious to know just what has changed about functional medicine; so I even went back to the same source that Dr. Sampson used eight years ago, the Institute for Functional Medicine (IFM), an organization founded by the other big name in FM, Jeffrey Bland, PhD.
Like pretty much all of “integrative medicine” it claims to look at the real cause of disease:
Functional Medicine addresses the underlying causes of disease, using a systems-oriented approach and engaging both patient and practitioner in a therapeutic partnership. It is an evolution in the practice of medicine that better addresses the healthcare needs of the 21st century. By shifting the traditional disease-centered focus of medical practice to a more patient-centered approach, Functional Medicine addresses the whole person, not just an isolated set of symptoms. Functional Medicine practitioners spend time with their patients, listening to their histories and looking at the interactions among genetic, environmental, and lifestyle factors that can influence long-term health and complex, chronic disease. In this way, Functional Medicine supports the unique expression of health and vitality for each individual.
You could remove the word “functional,” replace it with “integrative,” and easily plop this paragraph down into just about any article written about integrative medicine by an apologist. It’s the same weasel words of woo, different branch of woo. Or actually it’s the same branch, just a different sub-branch. But what does this all mean? The IFM claims:
- Functional Medicine offers a powerful new operating system and clinical model for assessment, treatment, and prevention of chronic disease to replace the outdated and ineffective acute-care models carried forward from the 20th century.
- Functional Medicine incorporates the latest in genetic science, systems biology, and understanding of how environmental and lifestyle factors influence the emergence and progression of disease.
- Functional Medicine enables physicians and other health professionals to practice proactive, predictive, personalized medicine and empowers patients to take an active role in their own health.
You know, I hate it when woo-meisters liken things to “operating systems” while referring to “outmoded acute care models.” One thing you can be sure of, though, is that whenever someone like Dr. Bland refers to using the “latest in genetic science, systems biology, and understanding of how environmental and lifestyle factors influence the emergence and progression of disease,” you will be in for a heaping helping of abuse of those new sciences. We’ve seen it time and time again with, for example, epigenetics (which doesn’t do or mean what quacks think it does), placebo effects, the power of diet (which is often grossly exaggerated), and, of course, systems biology, which FM guru Mark Hyman himself abuses shamelessly in the service of his made-up specialty. Indeed, Hyman is an excellent example, as he’s mangled science in the service of FM in many areas, including cancer, autism (of course, given his latest foray into antivaccine propaganda), and, of course, Alzheimer’s disease and other forms of dementia. That’s just a sampling, of course. What’s worse, is that FM seems to value anecdotes over actual clinical studies. Basically, its form of “personalized medicine” appears to be a “bait and switch” designed to lower the standard of evidence required to justify a treatment.
Don’t believe me? Read it right from the horse’s mouth, so to speak. First:
Functional Medicine is an approach to health care that conceptualizes health and illness as part of a continuum in which all components of the human biological system interact dynamically with the environment, producing patterns and effects that change over time. Functional Medicine helps clinicians identify and ameliorate dysfunctions in the physiology and biochemistry of the human body as a primary method of improving patient health. Functional Medicine is often described as the clinical application of systems biology. [Emphasis in original]
But more tellingly, see what Bland says about the evidence base for FM:
When people ask to see the evidence for Functional Medicine, they often mean, “Where are your research trials, comparing Functional Medicine to conventional medicine in a clinical setting?” Unfortunately, current research models do not have a way to test each individualized, patient-centered therapeutic plan that is tailored to a person with a unique combination of existing conditions, genetic influences, environmental exposures, and lifestyle choices. Clinical trials do play a significant role in evaluating and comparing the efficacy of new pharmaceutical treatments, especially when it is important to rule out placebo effects, but they have many inherent limitations which constrain their ability to inform clinical decision making.
So let’s not even bother doing clinical trials, then, amirite? Basically, this is a manifesto for doing whatever the heck a physician wants in the name of “personalizing” care. Whenever I see such piece of utter nonsense used as a justification, I can’t help but point out that real doctors and scientists are trying very hard to figure out new clinical trial methodology in order to test precision medicine (which used to be called “personalized” medicine) in a scientifically rigorous manner. Yes, in the early “wild west” days (which we are only now coming out of), a lot of physicians made it up as they go along with respect to interpreting the results of whole genome sequencing to select cancer treatment, but that is increasingly frowned upon. If scientists can put together a trial as clever and complex as the SHIVA trial, I laugh at Jeff Bland telling me that FM can’t be tested because it’s two “personalized.” It’s a lame excuse—the very lamest—and exactly the same excuse that homeopaths, acupuncturists, and the like make for not doing clinical trials testing their quackery, though FM tries to “science it up” by rationalizing it with these seven principles:
- Acknowledging the biochemical individuality of each human being, based on concepts of genetic and environmental uniqueness
- Incorporating a patient-centered rather than a disease-centered approach to treatment
- Seeking a dynamic balance among the internal and external factors in a patient’s body, mind, and spirit
- Addressing the web-like interconnections of internal physiological factors
- Identifying health as a positive vitality—not merely the absence of disease—and emphasizing those factors that encourage a vigorous physiology
- Promoting organ reserve as a means of enhancing the health span, not just the life span, of each patient
- Functional Medicine is a science-using profession
That very first principle is FM’s “get out of jail free” card for basically anything its practitioners want to do. They can always find ways to justify any form of treatment, be it science-based or quackery, simply by invoking the “biochemical individuality” of each human being. Here’s the problem: Yes, human beings are individuals, and each human being is unique. However, we’re not so unique that our bodies don’t all work pretty much the same way. In other words, in terms of biology, physiology, and yes, systems biology, human beings are far more alike than they are different. If that weren’t the case, modern medicine, developed before we had the tools to probe our genetic individuality, wouldn’t work as well as it does. FM fetishizes “biochemical individuality,” not so much because humans are so incredibly different that each one absolutely has to have a markedly different treatment. We’re not. FM fetishizes “individuality” because it distinguishes FM as a brand from science-based medicine and, I suspect, because it makes FM practitioners feel good, like “total” doctors never at a loss for an explanation for a patient’s symptoms or clinical condition. As for the last bit about FM being a “science-using” profession, I like to say that FM “uses” science the same way that a drunk “uses” a streetlight pole or a wall: To hold himself up against the force of his inebriation’s effect on his brain.
Overall, there are some things that FM gets right, although they are no different than the things every primary care doctor should be getting right, namely emphasizing healthy lifestyles, good nutrition, enough exercise, adequate sleep, cessation of habits known to be deleterious to health (e.g., smoking). They tend to spend more time with patients, which is something that primary care doctors have a harder time doing these days. They emphasize prevention, which is a good thing but again something that good primary care doctors do anyway.
Where they go wrong is in what Grant Ritchey described as a major unstated premise. That premise is that FM really does address the root causes of disease better than conventional medicine. FM also encompasses a lot of quackery, such as acupuncture, chiropractic adjustments, and especially “detoxification” programs. There also seems to be considerable overlap between FM and orthomolecular medicine, as FM practitioners seem quite enamored of high dose vitamin C infusions. Indeed, one of the quackiest of the quackademic medicine centers in this country, the University of Kansas, emphasizes FM and orthomolecular medicine and is run by a woman who is very much a proponent of high dose vitamin C infusions for cancer.
One of the most prominent identifying features of FM is its reliance on laboratory tests, lots and lots and lots of laboratory tests. They use these laboratory tests to seek out each patient’s “biochemical” individuality and analyze his systems in these areas:
- Assimilation: digestion, absorption, microbiota/GI, respiration
- Defense and repair: immune, inflammation, infection/microbiota
- Energy: energy regulation, mitochondrial function
- Biotransformation and elimination: toxicity, detoxification
- Transport: cardiovascular and lymphatic systems
- Communication: endocrine, neurotransmitters, immune messengers
- Structural integrity: subcellular membranes to musculoskeletal integrity
This search for “biochemical individuality” leads FM practitioners to order incredible numbers of labs, as you will see, many of which, as Kimball Atwood pointed out a long time ago, are bogus and of no use, and many of which are routine lab tests that regular doctors order but often end up massively misinterpreted and abused. In particular, FM practitioners appear to like to order lab tests related to endocrinology. Of course, “normal” lab values are usually defined to be a certain number of standard deviations from the population mean, which means that by random chance alone a small percentage of “normal” people will have an abnormal value of a given laboratory test. When a clinician orders a bunch of laboratory tests on a patient, the likelihood that one of those tests will be “abnormal” will approach 100% the more tests are ordered. No wonder FM practitioners can always find lab abnormalities to chase. Of course, to correct those lab abnormalities, there are always many, many supplements to be sold. Indeed, arguably the IFM was founded as a means of marketing the supplements Jeffrey Bland sold. Mark Hyman, through his “Ultrawellness” brand, also sells a lot of supplements.
Functional oncology in action
This brings us back to the case report. The authors include Elliot T. Taxman, BA; Erin D. Conlon, BS; Alex Speers, BA; Kristin L. Dismuke, BS; Tonya S. Heyman, MD, FACOG; Thomas L. Taxman, MD, FAAP. It turns out that Elliot Taxman, Erin Conlon, and Alex Speers are all students at the National College of Natural Medicine, while Tonya Heyman is a gynecologist specializing in “integrated personalized medicine” and Thomas Taxman is a pediatric gastroenterologist and functional medicine practitioner. The physicians are located at the Cleveland Health Institute in Lyndhurst, OH, which is a suburb of Cleveland. Given that the authors are all affiliated in some way with an “integrative medicine” clinic, I wasn’t sure where the patient discussed was treated for real. (I mean real cancer treatment, as opposed to the quackery she was subjected to in addition to her cancer treatment in a “complementary” fashion.) Perhaps it was at the Seidman Cancer Center at the University Hospitals of Cleveland, given that Dr. Taxman is an assistant clinical professor at the Case Western Reserve University School of Medicine.
Be that as it may, here is the clinical presentation as described in the case report:
An 80-year-old Caucasian female patient presented to an integrative medicine clinic in December 2012 with a 1-month history of a tender right breast. Her history was significant for arthritis, obesity, hypothyroidism, chronic gastritis, and hypertension. Her current medications included hydrochlorothiazide and triamterene, quinapril hydrochloride, levothyroxine sodium, and esomeprazole. Her family history was positive for breast cancer (daughter at age 46 y and sister at age 70 y). Physical exam revealed an erythematous, warm mass with irregular borders and localized skin thickening palpated across both upper quadrants of the right breast. The mass measured approximately 15 × 10 × 5 cm. In addition, a prominent 1-cm right axillary lymph node was noted.
This presentation sounds like that of an uncommon and particularly nasty form of breast cancer known as inflammatory breast cancer (IBC). IBC is characterized clinically by more than half the breast being involved with an inflammation-like reaction and pathologically by tumor cells in the dermal lymphatics (the lymph vessels right under the skin). The standard treatment for this aggressive form of breast cancer is neoadjuvant chemotherapy (chemotherapy before surgery), a modified radical mastectomy (removal of the breast and the axillary lymph nodes), followed by post-mastectomy radiation therapy to the chest wall. By definition, IBC is at least stage IIIB. On the other hand, IBC is a clinical diagnosis. Absent a skin biopsy showing tumor cells in the dermal lymphatics, its diagnosis is purely clinical so this woman might not have had IBC. Still, from the description, it looks as though neoadjuvant chemotherapy was appropriate:
Mammography revealed increased irregular density in the central upper quadrants of the right breast. A subsequent ultrasound noted a mass in the right breast that was highly suggestive of malignancy and the accompanying guided biopsy concluded invasive ductal carcinoma, grade 3, with involvement of a right axillary lymph node. A magnetic resonance imaging (MRI) on January 7 confirmed the previous diagnosis and indicated that a small mass was found in the left upper outer quadrant of the left breast. A follow-up sonogram and mammogram of the left breast confirmed the MRI findings. She was given a Breast Imaging-Reporting and Data System (BI-RADS) score of 6 and her cancer was concluded to be ER/PR negative and HER2 positive.
A tumor that lacks estrogen receptor and progesterone receptor but does have amplified HER2 almost always gets neoadjuvant chemotherapy consisting of a regimen of cytotoxic chemotherapy combined with Herceptin, which targets HER2. The patient underwent a bone scan and PET-CT scan, the latter of which is bit of overkill, because PET-CT has never been shown to be superior to CT alone in the setting of breast cancer. Both were negative, which means that the patient was not stage IV and the title of the case report, “Chemotherapy and Functional Medicine in a Patient With Metastatic Breast Cancer: A Case Report,” shows that the people writing and reviewing it were clueless about breast cancer. This woman did not have metastatic breast cancer, at least not the way a breast cancer surgeon and oncologist look at it. Lymph node metastases are generally considered regional disease. Use of the term “metastatic disease” tends to imply there are metastases to distant organs (i.e., stage IV disease), which is why breast cancer specialists distinguish between locoregional and distant metastatic disease; the implications are very different if a patient has a metastasis in an axillary lymph node (or even several) than it is when she has a metastasis in, say, liver, bone, or lung. The former still represents potentially curable disease, the latter does not. Be that as it may, this woman was potentially curable and was clearly in pretty good shape for an 80 year old if they were willing to give her chemotherapy, even though she did have a fairly typical litany of diseases and conditions of the elderly (arthritis, obesity, hypothyroidism, chronic gastritis, and hypertension). On the other hand, it’s not as though there was much choice, given that the cancer was ER/PR-negative and therefore estrogen blocking treatments were not an option.
In any case, what sounded like fairly standard chemotherapy was initiated, including docetaxel (Taxotere), carboplatin (Paraplatin), and trastuzumab (Herceptin) and underwent a right modified radical mastectomy after six cycles, followed by radiation therapy. She also underwent a left simple mastectomy (no evaluation of lymph nodes) for reasons that were unclear to me. She apparently had had something spotted in the right breast on her preoperative MRI, but it was never biopsied, as far as I can tell, and therefore never proven to have been cancer. Given that there is no survival benefit in doing it in the absence of a deleterious cancer-causing mutation, it’s hard enough to justify a prophylactic mastectomy on the other side in much younger woman, say 50 years old, but to do this operation on an 80 year old, whose life expectancy (and thus time remaining in her life to develop another life-threatening invasive cancer) is so much shorter, is questionable. Yes, they did find a small focus of ductal carcinoma in situ, but that would have been very unlikely to have progressed to endanger this patient’s life in her remaining time. Of course, the choice of surgery was on the conventional breast surgeon, not the FM doctors, but I felt obligated to point this out, given that we’re talking about my specialty here.
Now get a load of this chart, which shows what she got overall (click to embiggen):
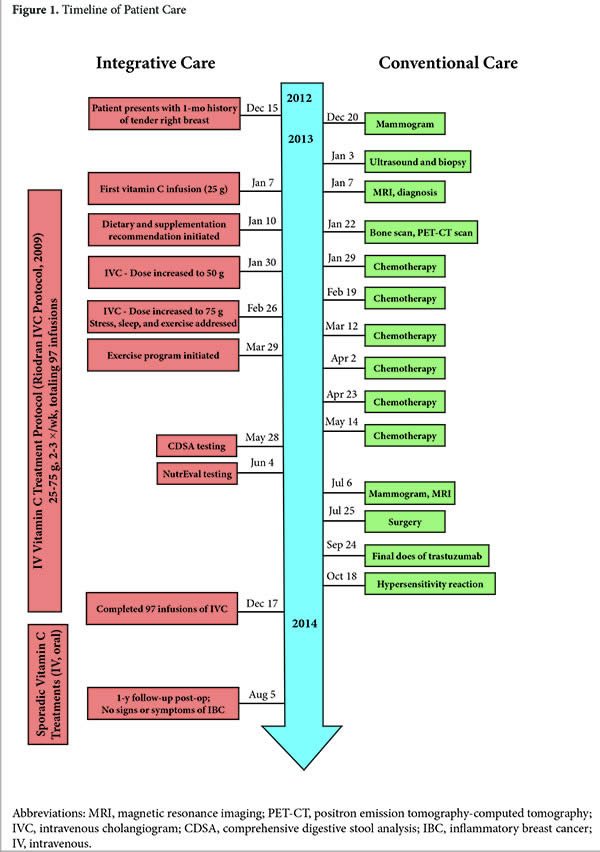
She received 97 infusions of vitamin C. Yes, you read that right. In the eleven months or so that her complete science-based therapy of her breast cancer required, this woman was subjected to 97 unnecessary and potentially harmful infusions of ascorbate. Afterward, she received “sporadic” doses of vitamin C up through to August 5, 2014, which was one year after her mastectomy. Fortunately, she was tumor-free. As I’ve written before many times, there is no good evidence that high dose IV vitamin C has a clinically useful antitumor effect. No, Linus Pauling has not been vindicated, although FM practitioners, naturopaths, and other believers have been trying for decades.
But that’s not all this poor patient received.
She was placed on a dairy-free, gluten-free, low glycemic index diet for…why? Who knows? There’s no good evidence that such diets have an anticancer effect. She was also placed on the following supplements:
- Melatonin: 20 mg QHS
- Digestive enzymes AC
- Probiotics: 60 billion CFU BID
- Lactobacillus acidophilus NCFM
- Bifidobacterium animalis Bi-07
- Medical food shake bid
- Vitamin D3: 5000 IU QD
- EPA:DHA: 6000 mg QD
- Wheat germ extract: 5.5 g QD
- Oral vitamin C: 18-24 g QD
- Standardized herbal inflammation relief supplement
One wonders why she was taking 18-24 g (that’s right, grams) of vitamin C per day in addition to the boatloads of vitamin C she was receiving intravenously three times a week. As for the rest, they probably don’t hurt, but there’s no reason to think they help. They add no detectable medical benefit, but they certainly do add cost. That’s not even counting the labs ordered. Chemotherapy patients get a lot of labs done, but look at the additional unnecessary labs ordered on this patient. The results take up more than two pages of the case report, and include amino acid levels, “gut immunology” markers, secondary bile acids, parasite tests, pancreatic enzyme levels, heavy metal levels, and, of course, the most beloved lab tests of FM practitioners and autism quacks, oxidative stress markers like glutathione and coenzyme Q10.
And I haven’t even listed them all. None of these tests were necessary. Almost certainly, none of them added any value to the patient’s care. Equally certainly, they added a great deal of cost to this patient’s care.
In fairness, what the FM practitioners added wasn’t all bad. An exercise program was started consisting of 10 minutes of bicycling a day working towards 30 minutes, Qigong classes, a sleep log, individual counseling and group support, and a part-time caregiver. None of these things, however, is the least bit “integrative” and could easily have been done by any oncologist, assuming the patient’s Medicare would pay for it.
The end result: Nothing
So what was the result after all of this? The patient survived two years, but the odds of her surviving five years were probably around 70% anyway with conventional therapy and probably 85% of surviving two years, based on her clinical presentation and final pathology, worse if she actually did have IBC. Try as they might, even the FM docs who wrote up this case report couldn’t make a case that what they did added anything to this patient’s care, other than getting her off of her hypertension medications, which could easily have been result of weight loss and exercise, coupled with a hypersensitivity reaction she suffered when her cardiologist changed her medications. Indeed check out the final paragraph:
This case is unique because of the integrated approach guided in part by nutritional and digestive evaluation (NutrEval) from a Clinical Laboratory Improvement Amendments (CLIA)-certified laboratory testing company (Genova Diagnostics, Asheville, NC, USA) that was used in the management of this patient with advanced ductal breast carcinoma.5 Because this is a case report from the real world practice of medicine, it is not possible to determine the responsibility of the treatments in this patient’s success in achieving remission. Nevertheless, the patient survived her cancer with minimal side effects during treatment and is now in her third year of remission. This case study highlights the potential benefits of integrative therapy in the comanagement of patients with invasive ductal carcinoma of the breast.
No, we can say with a very high degree of certainty that the only benefits this patient experienced came from exercise, a personal care giver, counseling, and perhaps her sleep log. The high dose vitamin C, the dozens of lab tests, and all the supplements did her no good but certainly cost a lot of money. I can’t help but shake my head at this. In particular, I am amazed that the FM doctors presenting this case actually seem proud of what they did. They should be ashamed.
I am, however, glad they wrote up this case report, as crappy as it is. It shows what FM really is when in actual use. All those high-sounding ideals and principles, all the claims that FM treats the “underlying cause” of disease are revealed to be delusions when you just look at what FM doctors really do when treating cancer patients. Harriet Hall’s aphorism about CAM in general fits perfectly: What’s good about FM is not unique, and what’s unique about it is not good. My conclusion about FM is, in addition to Harriet’s, that it takes “making it up as you go along” to a whole new level, and that’s not a good thing in medicine.