
{kind=link}
Since COVID-19 was officially declared a pandemic on March 11, unsurprisingly much of the material written for this blog has focused on the science and pseudoscience of COVID-19. In particular, we have covered medical misinformation, urban legends, astroturf disinformation campaigns, and conspiracy theories being spread in what is sometimes called a COVID-19 “infodemic”, as well as the regulatory and public health issues regarding proposed COVID-19 therapeutics and vaccines. However, there is one disturbing false (or at least highly distorted) narrative that we haven’t really addressed, at least not directly. I’m referring to a narrative that started very early on in the pandemic that nutrition and lifestyle can protect you against the coronavirus, or at least make it much less likely that you will develop life-threatening illness if you do “catch this cold“, as Del Bigtree so disturbingly and deceptively put it as he vastly understated the dangers posed by the virus and basically proposed leaving those at high risk for serious disease on their own during this pandemic. (I will be quoting him again later, near the end of this post.)
Of course, those inclined to distrust “Western medicine” and believe in so-called “alternative medicine”, or, as it’s increasingly called as it’s been infiltrating conventional medicine, “complementary and alternative medicine” (CAM) or “integrative medicine”, have long overemphasized the potential benefits of nutrition and lifestyle in preventing infectious diseases (or at least drastically ameliorating their symptoms to the point where they go from being potentially life-threatening to minor inconveniences that serve only to “strengthen the immune system”). Just as a reminder, I’ll cite an example over a decade ago during the H1N1 influenza pandemic. Then, HBO’s “politically incorrect” pundit Bill Maher, whom I had noticed spreading antivaccine talking points years before (and who’s still doing it), touted the benefits of nutrition and lifestyle and bragged that, because of it, he’d never catch the flu, even on an airplane. Indeed, Maher said, “I would never get the flu on an airplane”, presumably because his immune system is so healthy and, thanks to his lifestyle, there is no “swamp” there for the virus to breed in, leading his guest Bob Costas to retort in an exasperated voice, “Oh, come on, Superman!” (This was the best retort ever to Maher’s antivaccine nonsense, with the possible exception of Bill Frist basically calling him the “crazy person” when it comes to vaccine pseudoscience.)
Maher is just one of the more amusing examples of antivaxxers and quacks implying (or outright claiming) that nutrition can do a better job of preventing infectious disease than vaccines. I could quote many others, given that I’ve been following the antivaccine movement since the early 2000s. One particular favorite is a common antivaccine claim that, because children in Third World countries are much more likely to die when they contract measles than children in First World countries, nutrition and sanitation are far more important in preventing measles than vaccines, the idea being that better nutrition makes for a “stronger immune system”. Basically, it’s a good example of how antivaxxers take a pebble of truth (certainly poor nutrition does impact the immune system) and try to turn it into a boulder of an unsupported claim or outright lie (e.g., that nutrition can do as well or better, in “strengthening the immune system” to prevent infectious diseases, than vaccines).
It’s not just infectious diseases, either. This fetishization of nutrition and food above all permeates not just the antivaccine movement but all of alternative medicine. Indeed, when alternative practitioner Toni Bark developed a deadly cancer, the cognitive dissonance was such that her son had to admit that she developed her cancer even though she had lived what he considered to be an incredibly healthy lifestyle and consumed a vegan diet. (Yes, there is considerable victim blaming among the “nutrition cures everything” crowd.) A corollary of the “food as medicine” mindset is a persecution complex, in which advocates like to claim that any suggestion that food can cure or prevent disease is dismissed by nasty scientists and skeptics as “quackery”. (It’s not; only overblown claims for the medical benefits of foods, nutrients, diet, and lifestyle are so dismissed.)
So it should be no surprise that similar claims are being made regarding COVID-19 and have been since very early in the pandemic, including claims that vitamin C (of course!) or an “alkaline diet” (double of course!) can treat or cure COVID-19.
Which brings me to an article reviewing a book by Dr. Asseem Malhotra, The 21 Day Immunity Plan:
Winter is coming and the current spate of Coronavirus-related news is not encouraging: the pandemic is ravaging Europe, efficient cures are still just over the horizon, and many are prophesizing that the second wave will hit us even harder than the first one. But amidst this doom and gloom, Dr. Aseem Malhotra’s book, The 21 Day Immunity Plan (1), is a much needed breath of fresh air.
Malhotra is a familiar name for European Scientist readers – in one of our most read articles of the year, Covid-19 and the elephant in the room, Dr. Malhotra excoriated the mainstream media for their failure to notice the role nutrition has in the outcome of Covid-19 cases. Obesity, diabetes, and other metabolic diseases led to increased hospitalization rates, overwhelming the NHS:
The government public health message enhanced by the media to stay at home, protect the NHS and save lives has been powerful and effective. Given the speed at which health markers for metabolic disease improve from dietary interventions, an equally strong if not more significant population health message should now be to “eat real food, protect the NHS and save lives.”
Driving that point home, Malhotra has now followed up on this story with a solid 21-day program on how to optimise the immune fonction [sic].
To see where this is going, let’s first look at what we know about the factors that predispose to death or serious illness from COVID-19.
COVID-19 risk factors
Since the earliest major outbreak of COVID-19 in Wuhan, China, doctors have recognized certain risk factors that portended a higher likelihood of life-threatening illness and death from SARS-CoV-2, the coronavirus that causes COVID-19. Many of these risk factors have been confirmed over and over again in multiple studies in multiple countries.
Unmodifiable risk factors for death from COVID-19
The first—and by far the strongest—risk factor for serious disease and death due to coronavirus is unchangeable. Specifically, it is age. It has been known since very early on in the pandemic that, the older you are, the more likely you are to die if you contract COVID-19—and not by a little. The CDC has published a handy-dandy guide that tells you how much higher or lower your risk of death due to the virus is compared to the reference group (18-29 year olds). There is a dramatic increase in the risk of hospitalization and death with rising age, going from a 2x higher risk of hospitalization and 4x higher risk of death for 30-39 year olds to a 13x higher risk of hospitalization and 630x higher risk of death in those 85 years of age or older:
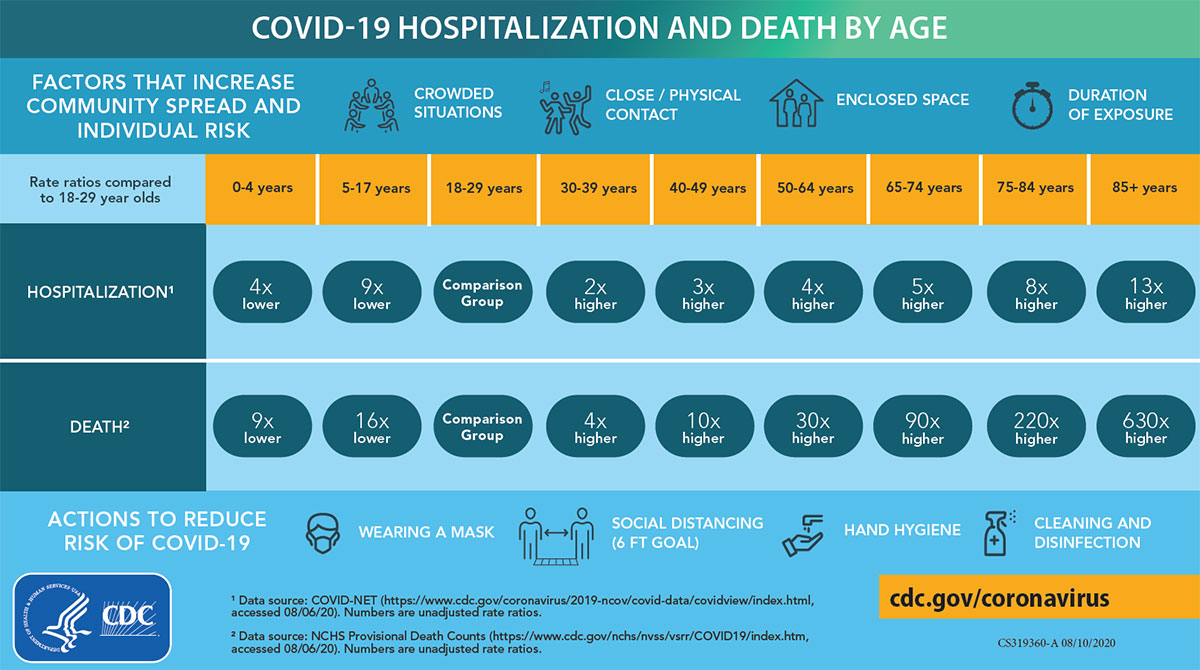
Hospitalization and death due to COVID-19 by age
In terms of absolute numbers, the reported case fatality rates (CFRs, or the risk of dying if you develop symptomatic COVID-19) range from 13%-20% for those over 80.
A recent study from PNAS shows this age effect most starkly:
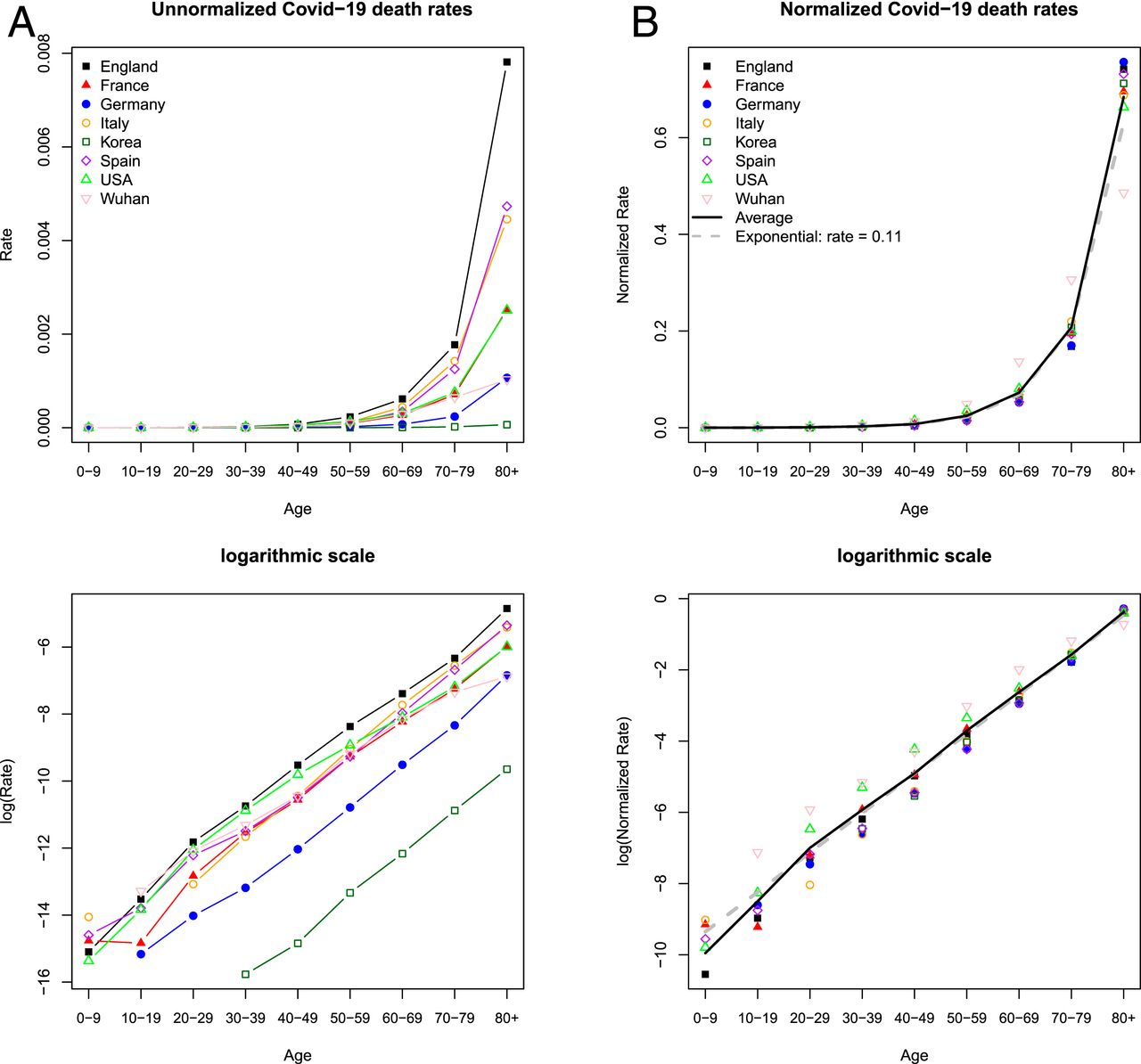
In terms of infection fatality rate (IFR), which includes all infections, including the asymptomatic, we know this
For every 1,000 people infected with the coronavirus who are under the age of 50, almost none will die. For people in their fifties and early sixties, about five will die — more men than women. The risk then climbs steeply as the years accrue. For every 1,000 people in their mid-seventies or older who are infected, around 116 will die. These are the stark statistics obtained by some of the first detailed studies into the mortality risk for COVID-19.
And:
“COVID-19 is not just hazardous for elderly people, it is extremely dangerous for people in their mid-fifties, sixties and seventies,” says Andrew Levin, an economist at Dartmouth College in Hanover, New Hampshire, who has estimated that getting COVID-19 is more than 50 times more likely to be fatal for a 60-year-old than is driving a car.
This preprint quantifies the risk. (Note that preprints are not yet peer reviewed.)
Another major risk factor for death is also unchangeable in that sex also matters. Men have a significantly higher risk of dying from COVID-19 than do women, as also shown in the preprint:
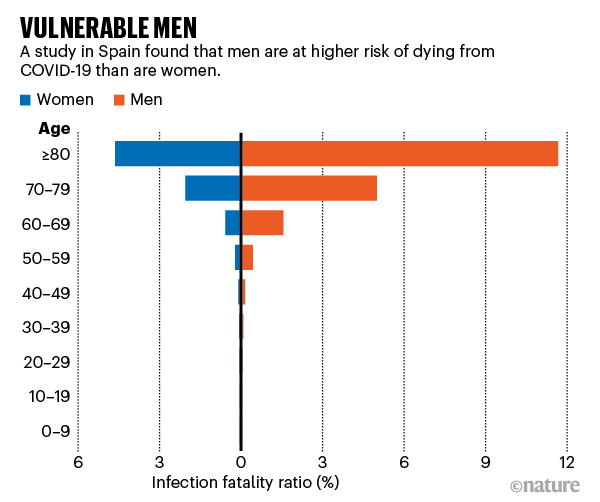
Deaths from COVID-19 in men vs. women
A recent correspondence in The Lancet suggests, though, that the relationship is not straightforward:
The overall male to female mortality sex ratio per 100,000 population was 1·4 (crude ratio 1·3). This ratio was not equal at all ages. For example, for people aged 0–9 years the ratio was 0·81. The ratio was 1·9 in the 40–49 years age group, 2·3 in the 50–59 year age group, 2·6 in the 60–69 years age group, and 1·65 in people older than 80 years (appendix p 1).
There was some variation across countries, although broadly the pattern was similar, and the numbers became too small for clear-cut interpretation (appendix p 3).
These data alter our understanding of male–female differences; the relationship is not straightforward, and efforts should now be made to understand risk based on the interaction of sex and age, along with other factors.
Unsurprisingly, ethnicity also plays a role. Of course, it can be difficult to separate socioeconomic factors from ethnicity, but we do know that there is a considerable racial and ethnic gap in terms of COVID-19 mortality, with Black people suffering death rates twice as high as white people, and Hispanic/Latino people somewhere in between. There is also evidence that Native American and Alaska Native people are at higher risk of death and severe disease as well.
Of course, we’re still early in our experience with COVID-19, and it will take considerably more research to tease out the reasons for elevated risk of severe disease and death in various populations. My point here is that there are at least two major risk factors that are not modifiable (sex and age) and at least one that might not be modifiable (race, if the increased risk is truly due to race and not more due to comorbidities and social forces that disproportionately affect Black populations and other minorities). No matter whether risk of death from COVID-19 can be decreased by “metabolic optimization” or not, if you’re 80 years old you’ll still be many, many times more likely to die of COVID-19 than if you’re 20 years old.
Modifiable risk factors for COVID-19
Another observation that was made early in the pandemic is that a number of chronic comorbid conditions correlate strongly with the risk of severe disease and death from COVID-19. Currently, these conditions include:
- Cancer
- Chronic kidney disease
- COPD (chronic obstructive pulmonary disease)
- Immunocompromised state (weakened immune system) from solid organ transplant
- Obesity (body mass index [BMI] of 30 or higher)
- Serious heart conditions, such as heart failure, coronary artery disease, or cardiomyopathies
- Sickle cell disease
- Type 2 diabetes mellitus
It’s also suspected that these conditions also predispose to severe disease from COVID-19:
- Asthma (moderate-to-severe)
- Cerebrovascular disease (affects blood vessels and blood supply to the brain)
- Cystic fibrosis
- Hypertension or high blood pressure
- Immunocompromised state (weakened immune system) from blood or bone marrow transplant, immune deficiencies, HIV, use of corticosteroids, or use of other immune weakening medicines
- Neurologic conditions, such as dementia
- Liver disease
- Pregnancy
- Pulmonary fibrosis (having damaged or scarred lung tissues)
- Smoking
- Thalassemia (a type of blood disorder)
- Type 1 diabetes mellitus
As you can see, these are a mixture of unmodifiable and potentially modifiable diseases and conditions. For instance, if you have cancer, chronic kidney disease, sickle cell disease, thalassemia, type 1 diabetes, or dementia, medical control can be optimized, but these can’t be reversed. The interesting question arises for conditions and diseases that can be impacted by lifestyle and nutrition, such as hypertension, obesity, and type 2 diabetes, the focus of the claims made by Dr. Malhotra.
Who is Dr. Aseem Malhotra?
Upon looking into his claims, I realized that I didn’t recall having ever heard of Dr. Malhotra before. It turns out that he appears (to me, at least) to be the UK equivalent to Dr. Mehmet Oz, a celebrity doctor known for promoting all sorts of dubious medicine, particularly diet advice. A quick search of this blog revealed that I had mentioned him before, as I had quoted him trying to explain away negative data on hydroxychloroquine for COVID-19. At the time, I had no idea of his reputation; so mea culpa.
In any event, Dr. Malhotra is a British consultant cardiologist best known for promoting a low-carb, high-fat fad diet known as the Pioppi diet, a diet that earned the “honor” of being named one of “Top 5 worst celeb diets to avoid in 2018” by the British Dietetic Association, along with the ketogenic diet, nutritional supplements, and a number of other fad diets, which characterized it as, in essence, a tarted up version of the Mediterranean diet that “recommends a higher fat diet than the traditional Mediterranean one” and notes that “adherents are encouraged to eat lots of vegetables, nuts, legumes, and fish and discouraged from eating red meat, starchy carbs, and sweetened treats.” It also encourages 24-hour fasting. Dr. Malhotra is also very much in the anti-processed sugar camp, having characterized sugar as “enemy number one in the Western diet.” To give you an idea of how anti-sugar he is, he recently made headlines by attacking Royal Free London NHS Foundation Trust for accepting a gift of 1,500 Krispy Kreme doughnuts sent to the staff as a gift for their work in dealing with the COVID-19 pandemic in the UK in March and April:
Absolutely disgraceful. Feeding junk food to already overweight and obese #NHS staff? I will forward this to CEO of @NHSEngland Simon Stevens personally and I can assure you he won’t be impressed especially as THESE foods a root cause of increased death rates from #COVID19 https://t.co/zAkIsyMJL4
— Dr Aseem Malhotra (@DrAseemMalhotra) April 22, 2020
And I’m going to tell your mother! Amusingly, Dr. Malhotra was dragged hard for his remark (and deservedly so!), as you will see if you click on the Tweet above and look at the responses, although there were also people who bought into this demonization of doughnuts.
Dr. Malhotra also seems to argue that modern medicine does more harm than good treating chronic conditions with medications, channeling Peter Gøtzsche in claiming that “too much medicine can kill you.” Of course, it is not in itself unreasonable to criticize too much medical intervention, but to me a brief perusal of Dr. Malhotra’s oeuvre gave off a seriously disturbing vibe that medicine doesn’t do any good for chronic illness. Unsurprisingly, he is a statin denialist, even having gone so far as to suggest that stopping statins might save more lives and that statins might not benefit anyone.
You get the idea.
So what is Dr. Malhotra arguing? I haven’t read his book, although the review makes plain that it’s basically a repackaging of his promotion of the Pioppi diet. Of course, any book called The 21 Day Immunity Plan that implies that you can basically “fix” your immune system with diet in 21 days is going to draw a lot of skepticism, and rightly so. For instance, how does he justify 21 days? Why not 30 days? Why not 14 days? Why not 60 days? According to the credulous review:
Of course, one will question the arbitrary choice of 21 days. Why would three weeks be enough? Well, as it happens, the number 21 is explained at length by the author, who refers to numerous studies (4) as well as his first-hand experience with the program. In the context of the book, this is justified by good pragmatic reasons such as:
- For most people it takes three weeks to break any habit, or for many what is a form of addiction to sugar and ultra-processed food. »
- Most people with adverse metabolic health will start to see marked improvements to their health and/or shape albeit to different degrees within three weeks, without having to count calories. »
- It is the need to change the narrative around the impact of lifestyle changes and show that their effect on health can be rapid and substantial. We should use this to motivate ourselves to continue to reap the benefits of improved health for life.
What’s Reference 4? Jean-Paul Oury, the reviewer, cites two studies without links or references to them:
A previous diet and exercise study carried out by researchers at the University of California involving 31 participants also revealed reversal of metabolic syndrome in 50 per cent of those that followed a low-fat, high-fibre diet combined with 45–60 mins of moderate intensity exercise per day. Markers of insulin resistance improved but again there was no correlation with weight loss suggesting an independent benefit on metabolic health. Similar rapid improvements in markers of metabolic health with reversal of metabolic syndrome in all participants were observed in a trial involving 7 obese children from a diet and exercise program within 21 days.
31 participants? Seven obese children? These are not particularly large studies. As for Dr. Malhotra’s “first hand experience with the program”, you know what they say about anecdotes…
Still, one has to consider the possibility that, history of overblown claims for the dangers of processed sugar and pharmaceutical medicine and the benefits of a specific fad diet aside, it’s possible Dr. Malhotra could have a point. In fact, he probably does have a germ of a good point. It’s clearly just massively exaggerated.
Can “metabolic optimization” prevent or treat coronavirus?
The first thing to realize here is that, if you’re obese (particularly if you’re morbidly obese), losing weight is a good thing for your health. Even if it doesn’t do a thing to decrease your risk of life-threatening COVID-19, reaching a healthier weight can decrease your risk of any of a number of complicating conditions, including hypertension, heart disease, type 2 diabetes, certain cancers, stroke, fatty liver disease, and more. There is no doubt that losing weight to come closer to a healthy weight range is associated with improvements in many of these conditions, especially type 2 diabetes and hypertension, which can sometimes be reversed by weight loss to the point where medication is no longer necessary.
At the risk of “going anecdotal”, I know that this can be true. Over about a two to three year period, I changed my diet and started exercising regularly, ultimately losing 50 lbs. As a result, the dose of blood pressure medicine that I need to keep my blood pressure under control has declined markedly, and I might even be able to get off of blood pressure medicines altogether. (We’ll see. Given that I’m now at my target weight, with a BMI in the “normal”—whatever that means—range, I might well have maximized my benefit on that score, and my family history doesn’t bode well for my ever getting completely off of blood pressure medication.) Similarly, I might well be able to get off of statins, as my total, LDL, and HDL cholesterol levels are quite acceptable now. (As an aside, I look at studies suggesting that ACE inhibitors might decrease the risk of life-threatening COVID-19, and I wonder if I want to be off my ACE inhibitor altogether or not while the pandemic is still raging.)
The bottom line is that we have no strong evidence yet that “metabolic optimization” will decrease the risk of severe COVID-19, although it is certainly scientifically plausible that weight loss to bring oneself out of the obese range could well help. It’s also undeniable that weight loss and exercise are good things for one’s general health if one is obese, and that a healthier diet can impact type 2 diabetes, hypertension, and other chronic “lifestyle diseases”. On the other hand, it is possible that it might be that treating the “root causes” of metabolic syndrome might not lead to a decreased risk of severe COVID-19, a scenario that could happen if the “root cause” of metabolic syndrome leads to metabolic syndrome through a different mechanism from the one by which it increases the risk of severe COVID-19. Basically, we just don’t know yet. Moreover, where Dr. Malhotra goes wrong is in touting a fad diet as The One True Diet to fix one’s immunity in three weeks, a claim for which there is no good evidence. For example, how do we know his diet is a more effective, healthier way to “metabolic optimization” compared to all the other “healthy diets” out there? We don’t.
It’s particularly irritating to see these sorts of statements:
Dr. Aseem Malhotra : The best vaccine against Coronavirus is optimising metabolic health https://t.co/mWbew8aaER
— Dr. Jason Fung (@drjasonfung) August 28, 2020
In particular, there’s a distinct possibility of this:
More importantly, “optimizing metabolic health” takes time. It’s highly unlikely that 21 days would make a significant difference in decreasing your risk of severe COVID-19, and it’s unhealthy to lose weight too quickly. (We don’t know, but it’s not at all implausible that rapid weight loss could potentially actually be another factor for severe COVID-19.) It’s generally advised that you shouldn’t lose more than a pound or two per week. If you’re 25 lbs. overweight, that’s 12-25 weeks to get down to your target weight. Obviously, if you’re more overweight than that, it will be longer. Losing weight and changing your diet is also very, very hard. Many people can’t do it, or at least they have a lot of difficulty doing it. The reason I could do it is that I had several advantages, including:
- I have money.
- I don’t live in a food desert, where calorie-rich fast food is a main food source and it’s difficult to find vegetables, fruits, and other healthier choices for food.
- I can arrange my schedule so that I have time for exercise.
- I have a supportive wife.
- And many others.
Not everyone has these advantages.
There’s another pernicious aspect to this narrative. Even if nutrition could prevent coronavirus, Dr. Malhotra’s is a very privileged position that basically excludes those unable to “optimize metabolic health”. These “nutrition cures and prevents #COVID19” people labor under a delusion of privilege in that they have the time, resources, and luxury to “optimize their metabolism”. There’s also a subtext of victim blaming where it’s your fault if you get sick because you didn’t “optimize your nutrition”. And, make no mistake, victim blaming is rampant among these “nutrition prevents/cures COVID-19” propagandists. Indeed, Del Bigtree did just that when he urged his presumably “healthy” listeners to “catch this cold“. That’s why I’m going to quote him again extensively:
What is the group that is really at risk? Let’s be honest about this and say something that might get me some trouble here, but let’s be honest. That group is very well known. It’s people over the age of 65—not just because you’re over the age of 65, but you’re sick with other diseases. You have heart disease. You have COPD. You have diabetes. You have issues, many of those issues coming from the fact that you didn’t treat your body very well while you were on this planet. And I want to talk about this for one minute as we close this down. That 0.26% are the most sick among us, and I have nothing against you. Go ahead and bubble wrap your house. Lock yourself in your basement. Go and do what’s necessary.
But here’s the problem. When you were my age, you were most likely eating food and fast food and Doritos and drinking Coca-Cola, which you’ll never find in my home. You were eating that all the time. You probably were drinking a lot of alcoholic beverages and really liked to party and enjoyed your cigarettes and said to yourself, “You know what? It’s more about the quality of my life right now. I don’t care if I live to be 100 years old. I want to enjoy my life right now. I like the finer things in life. I like good rich food. I like smoking a cigarette once in a while. I like to drink my drinks.” And you know what? Good on you! That’s the United States of America. No problem, that, some of my best friends think like that. It’s great, and they’re fun to hang out with. That’s perfectly OK.
But here’s what’s not OK. When you reach that point in your life where now your arteries are starting to clog up, your body is shutting down, and the alcohol is eating up your liver, and you have diabetes, or you have COPD, you have asthma, you can’t breathe, all the cigarette smoking has finally caught up with you, you have heart disease because of the way you decided to live your life in the moment, here’s what you are now. You are pharmaceutical-dependent. You did that to yourself, not me. You decided that the moment mattered, and now you find yourself pharmaceutical-dependent, which is really what that 0.26% is, and that’s OK too. Thank God there’s drugs out there! There’s drugs that allow you to eat the Philly cheesesteak even though your body knows it hates it, but, go ahead, take the Prilosec. What difference does it make? Drug yourself! Drug yourself! Get through the day! Don’t exercise! Maybe just attach an electrode and see if a little electricity to the stomach will give you the abs you want.
Come on! Grow up! You made choices! And now that you’re pharmaceutically dependent, here’s what you don’t get to do. You don’t get to say I have to take a drug to protect you. That’s what this is. You don’t get to say I have to wear a mask and suck in my own CO2 to protect you. You don’t get to say I have to lock myself in a basement and destroy my career and take away my own ability to feed children because you are pharmaceutical dependent. You lived your life. You made your choice. And thank God we live in the United States of America so you don’t have to worry about grocery police standing outside a grocery store saying, “Really? You really need four liters of Coca-Cola? You really need four bags of Doritos or Chitos or Fritos or whatever the heck it is, little cupcakes with synthetic icing on them? You really need all that?” Because we could go there. We could go there. If we’re really going to get into each other’s schiznit, that’s what we could do.
Or could we live and let live? Eat all the Twinkies you want! Drink all the bourbon you want, and smoke as many cigarettes as you want, and when you find yourself pharmaceutical-dependent I will go ahead and say thank God the drug companies are there for you, but you do not get to make me pharmaceutical-dependent. You do not get to put me in the way of Heidi Larson, who wants to eradicate natural health and natural immunity and make us all pharmaceutical dependent.
Again, make no mistake. Dr. Malhotra’s message is simply a more genteel, less obviously judgmental version of the message that Del Bigtree is promoting. As I mentioned when I first dealt with Bigtree’s message, I once coined a term, the central dogma of alternative medicine, to describe the belief that we have near-total control over our health through lifestyle, such as diet, activity, exercise, and a Secret-like belief that wishing makes it so. It never seems to occur to them that age is a major risk factor for death from COVID-19 and that people can’t do anything about how old they were when the pandemic hit, nor can older men like myself do anything about the fact that we were older men when the pandemic hit.
Certainly, a healthy weight, exercising, eating a healthy diet are all good things for your health. Who knows? They might even lower your risk of severe COVID-19. However, don’t be fooled by overblown claims for what they’ll do for your risk of COVID-19, and don’t forget the judgmental implications behind advice like that promoted by Dr. Malhotra. He’ll deny it to high heaven, of course, and maybe he personally doesn’t intend to be judgmental, but judgment is there nonetheless.