
{kind=link}
In June, founding Science-Based Medicine editor Dr. Harriet Hall posted a favorable review of a fearmongering and unscientific book about trans youth on this website. Ultimately, the post was reviewed and retracted for lack of evidence-based claims and was soon republished on Michael Shermer’s Skeptic.com. In addition to an explanation published by Drs. Novella and Gorski regarding the reasons for their difficult decision, Dr. Gorski invited Dr. Rose Lovell and me to write a series of posts backed by research addressing the misinformation presented in Shrier’s book. Our articles were met with controversy and uproar from some. This outrage was spearheaded by a journalist named Jesse Singal, who over the last couple of months has almost single-handedly led the charge against SBM’s decision, attacking SBM on social media and in a long Substack article about “19 errors” allegedly made by Dr. Lovell and me (that to him are so very, very, very egregious) as well as numerous Tweets directed at SBM and its editors Drs. Novella and Gorski, Dr. Lovell (who, as she pointed out, hasn’t used Twitter in years), and myself. Given that the vast majority of the substance of Singal’s criticisms is either off-base or just plain incorrect, after several weeks of this Dr. Lovell and I, encouraged by Dr. Gorski, reluctantly decided to respond, even at the risk of fueling another round of social media outrage directed at us by Singal and his allies, and another war in the comment section of this blog.
Contrary to his extravagant claims on social media about SBM’s decision to retract Dr. Harriet Hall’s positive review of Abigail Shrier’s book Irreversible Damage: The Transgender Craze Seducing Our Daughters and the equally extravagant title of his blog post, “Science-Based Medicine’s Coverage Of “Irreversible Damage” Included About 19 Errors, False Claims About Three Sex Researchers, Made-Up Quotes, And Endless Misinformation“, Jesse Singal’s criticisms of the articles by Dr. Lovell and me deconstructing the claims in Shrier’s book do not substantively refute the evidence-based research and conclusions we presented, despite Singal’s insistence that so many horrific errors by us must be “corrected.” (The “errors’ that were actually errors turned out, unsurprisingly, to have been minor and have long since been corrected.) Dr. Lovell has already addressed Singal’s claimed “errors” relevant to her original guest post. Here, I will take the opportunity to discuss the remainder of them, given that, proportional to the length of my guest posts, most of Singal’s claimed “errors” were attributed to me.
1) Jesse Singal’s incorrect term: “Biological Girls”
Singal writes in defense of Abigail Shrier’s use of the term “biological girls,” arguing that:
Shrier is simply using “biological girl” to refer to someone’s biological sex in a setting where it matters a great deal.
As I have discussed previously, contrary to the view espoused by Shrier and Singal, biological sex is not as simple as a binary, M/F system, and this sort of terminology is inaccurate to begin with. “Assigned female at birth/assigned male at birth” (AFAB/AMAB) is the current medically-accepted terminology to describe the sex assigned to a newborn based on a doctor’s assessment of the external genitalia. For most individuals, this assigned sex aligns with their gender. For those for whom this assessment does not necessarily align with gender, the term “sex assigned at birth” was initially coined to distinguish sex from gender, a critical distinction for trans people whose importance cis people often do not understand.(Here are more gender basics.)
Consistent with the extravagant title of his critique, Singal goes on to make some extravagantly nonsensical characterizations of Dr. Lovell’s post and my posts, for example:
Science-Based Medicine appears to be promoting the view that if a 14-year-old natal female announces they are a trans boy, they are no longer biologically female — after all, it can’t be “considered defamatory and inaccurate” to refer to them as such if the claim is true. If this isn’t what Eckert is saying, what are they saying?”
There is a name for this logical fallacy, namely a straw man argument, particularly since neither Rose nor I ever said anything about trans male adolescents somehow being “no longer biologically female” (although we did say that it is harmful to misgender them). Indeed, terminology such as “no longer biologically female” is inaccurate and, when you come right down to it, doesn’t even make much sense. No one, least of all Dr. Lovell or I, has denied the sexes that trans teens were assigned at birth, and Singal, for all his obsessiveness in seeking out the tiniest of errors, was not able to find convincing examples that fit this risible characterization, hence my assessment of his statement as a straw man.
Singal then continues:
It’s almost like the whole point of these ever-stricter language rules is to make it impossible for any of us to talk about biological realities. But those realities are quite important.
This is, of course, a typical appeal to “censorship” beloved of the “gender critical” crowd. In Singal’s world, apparently the medical use of language is not actually intended to convey greater precision, but rather to be used as a tool of “control” and “censorship.” I have to ask as well: What does Singal even mean by “biological realities”? From my perspective (and that of most trans people), an appeal to “biological realities” in such a context rarely represents anything more than determinism and, more importantly, such appeals are almost always dog whistles for transphobes. Those who continue to espouse this notion apparently believe that, no matter what trans people do to affirm themselves in their gender, they can never, ever escape their “biology”. This concept also creates a rift between cis and trans people, with cis people laying claim to being the real men and women, and trans men and women being somehow “fake,” or at least somehow less than “real” men or women.
Singal keeps going, unfortunately:
More specifically, you can’t give a child competent care unless they understand they are biologically (fe)male and that this means certain things with regard to what transition will look like, what will happen during puberty if they don’t or de- transition, and so on.
Singal, as is the case with many issues, appears confused about the healthcare system and the routine clinical care of patients, which is not entirely surprising given that he is not a physician. The term “AFAB” tells you what sex your patient was assigned at birth. Anatomic inventories are part of every patient intake and charting, and preventive healthcare follows this inventory. Indeed, gender markers (documenting sex assigned at birth) are part of every Electronic Health Record, and not something a doctor would (or could) “mess up.” Moreover, clinical diagnoses are required to code visits for purposes of insurance and billing. Questions specific to assigned sex at birth are asked at every interview because the AFAB/AMAB designation is useful in the medical setting, specifically to provide competent care. Additionally, most electronic healthcare records are binary and/or do not capture LGBTQ experiences at all, meaning that people are often mischaracterized under male/female labels that do not match their identity. Finally, there are several ways a doctor is informed about whether a patient is AFAB or AMAB and what organs they do or do not possess; the information is impossible to miss and, where applicable, necessary to know in order to provide competent care.
Bottom Line: Language is always evolving. Using the AFAB/AMAB terminology is appropriate in medical settings. However, its use nonetheless belies a binarism based on sex-at-birth characteristics.
2) The First Amendment
Another objection that Singal expresses to my take on Shrier’s book is to object to my observation that Shrier appeals to the First Amendment to defend misgendering her subjects, claiming that she makes no such appeal. This is, quite simply, untrue. First, I never suggested that this appeal appeared in the Author’s Note, as Singal implies. Rather, Shrier connects “transgender politics” (Irreversible Damage, p.12) and specifically misgendering (incorrect pronoun use) to the First Amendment as follows in her book:
You’re not supposed to pick favorites among the amendments, because it’s silly, but I have one, and it’s the First. My commitment to free speech led me into the world of transgender politics, through a back door. In October 2017, my own state, California, enacted a law that threatened jail time for healthcare workers who refuse to use patients’ requested gender pronouns. The First Amendment has long protected the right to say unpopular things without government interference. It also guarantees our right to refuse to say things the government wants said.
If this is not an appeal to the First Amendment to support her misgendering trans people, I don’t know what is. Shrier goes on to pontificate:
In America, the government can’t make people say things—not even for the sake of politeness. Not for any reason at all.
– (Irreversible Damage, p.12)
Shrier also sources a Fox News article full of alarmist, sensationalized statements about people being sent to jail for incorrect pronoun use. Unfortunately for her, Politifact noted that the claims were distorted and misleading. Shrier also sources an opinion piece by Josh Blackman, a controversial lawyer and associate professor of law. Blackman’s statements about fines for incorrect pronouns have also been debunked.
Bottom Line: Shrier did appeal to free speech and the First Amendment in her book as justification for her misgendering trans people, but if anyone still thinks I am overinterpreting her words in her book as her view, she also wrote more specifically about the Constitution protecting free speech in a Wall Street Journal article titled “The Transgender Language War“.
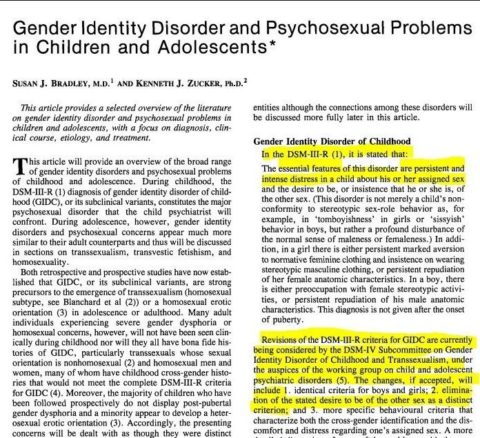
3) DSM-IV and DSM-5
Singal writes several paragraphs obscuring the differences between the DSM-IV and DSM-5. As with his other tired arguments, he has been engaged in this sort of rhetoric for years. I will summarize here, but have also written about the DSM-IV in my previous posts.
Singal states, along with his usual demand that we “correct the false claims”:
The DSM-IV did not classify “trans identity” as a mental illness. Unless I’m missing something and Eckert can provide evidence otherwise, Science- Based Medicine should correct the false claims that the DSM-IV categorizes trans identity as a mental illness and that Abigail Shrier endorsed it over the DSM-5 for that reason.
Let’ s just say that Singal is indeed “missing something.” As usual, he’s missing quite a lot, actually.
Gender Identity Disorder in the DSM-IV did reduce trans people who wanted to access gender affirming healthcare to a mental health disorder. Shrier connects the definition of GID in the DSM-IV to healthcare access, as she believes that only those with “traditional” (Irreversible Damage, pages 15, 16, 44, 55, 61) and “excruciating” (Irreversible Damage, page 112) gender dysphoria should garner mental health professionals’ attention “even perhaps by supporting medical transition” (Irreversible Damage, page 112). Shrier defines gender dysphoria as “characterized by a severe and persistent discomfort in one’s biological sex“. She sources the DSM-IV for this definition (Irreversible Damage, page 113).
As Singal notes, “being trans” does not equal gender dysphoria. However, diagnoses of GD and GID have been historically required for trans people to access care. Assigning a mental health disorder to a trans person for medical access is problematic. Additionally, a trans person without gender dysphoria deserves access to gender affirming hormones and/or surgery as much as one with GD.
Singal also claims that it is a “myth” that there is “some profound difference between the DSM-IV and DSM-5”. This is utter nonsense. The APA specifically states, as I mentioned in my review, the following:
With the publication of DSM–5 in 2013, “gender identity disorder” was eliminated and replaced with ‘gender dysphoria.’ This change further focused the diagnosis on the gender identity-related distress that some transgender people experience (and for which they may seek psychiatric, medical, and surgical treatments) rather than on transgender individuals or identities themselves.
Ironically, Shrier herself complains in her book about the difference between the DSM IV and DSM 5:
Interestingly, although the only relevant medical diagnosis is “gender dysphoria”, the APA guidelines talk about the treatment of “transgender” people. In other words, the APA has given up the vocabulary and perhaps even the methods of medicine in dealing with this population and entered the world of politics. It is worth asking whether a standard guided less by biology than by political correctness is in the best interest of patients.
– (Irreversible Damage, p.115)
There goes that appeal to “biology” again! Singal also states:
Eckert writes that “AFAB ‘tomboys’ and AMAB boys who liked to play with feminine-coded toys, and other children with gender non-conforming behaviors, were included in the GID category [in the DSM-IV].
The DSM-IV includes explicit language instructing clinicians not to diagnose merely gender nonconforming kids with GID.
Dr. Winters’ 2008 book, Gender Madness in American Psychiatry, written 5 years prior to the DSM-5 release, compiles short essays examining the diagnosis of GID in the DSM-IV. Winters notes:
GID is currently defined to favor gender-reparative therapies attempting to change one’s inner gender identity or suppress one’s outer gender expression…Diagnostic criteria for children were again broadened to place a greater emphasis on nonconformity to social sex stereotypes. These implicated children with no evidence of gender dysphoria as mentally ill…the clinical significance criterion failed to counter the stereotype that all gender variance is disordered. The criterion was brushed aside by Drs. Kenneth Zucker and Ray Blanchard (members of the Sexual and Gender Identity Disorders teams for the DSM-IV and DSM-V editions) as “muddled” and having “little import.”
The following are the DSM-IV-TR criteria verbatim:
The DSM-IV-TR Diagnostic Criteria for Gender Identity Disorder
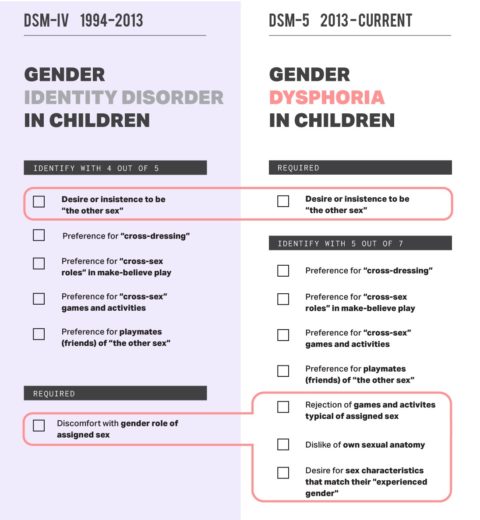
A. A strong and persistent cross-gender identification (not merely a desire for any perceived cultural advantages of being the other sex). In children, the disturbance is manifested by four (or more) of the following:
- repeatedly stated desire to be, or insistence that he or she is, the other sex
- in boys, preference for cross-dressing or simulating female attire; in girls, insistence on wearing only stereotypical masculine clothing
- strong and persistent preferences for cross-sex roles in make-believe play or persistent fantasies of being the other sex
- intense desire to participate in the stereotypical games and pastimes of the other sex
- strong preference for playmates of the other sex
B. Persistent discomfort with his or her sex or sense of inappropriateness in the gender role of that sex.
C. The disturbance is not concurrent with a physical intersex condition.
D. The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Under Part A Criteria, points 2-5 are examples of gender nonconformity. If a child met all of these, even without meeting point 1, they would be classified as having GID, since that child only needed to meet 4/5 criteria to qualify for a diagnosis. The diagnosis of GID did not require children to necessarily express a desire to be the opposite (only binary categories during DSM-IV) sex. To clarify, transgender people are those whose gender identity does not match their sex assigned at birth; gender nonconformity refers to behaviors and interests of an individual that challenge the stereotypes of the individual’s sex assigned at birth. Clothing/expression, play/fantasies, games, and playmates under Part A Criteria align with gender nonconformity but not necessarily with being trans and/or with gender dysphoria, while Part B Criteria allow for gender role discomfort to be categorized as GID, which could include, for example, AMAB children averse to playing with trucks or to rough play with other AMAB children. Part A criteria enforce narrow, dated sex stereotypes. Part D criteria do not distinguish between gender dysphoria stress and the stress induced by living in a society intolerant of gender nonconformity.
Zucker wrote the Gender Identity Disorder chapter in the 2000 Handbook of Developmental Psychopathology. In it, he notes that “parental tolerance of cross gender behavior,” or encouragement, and/or raising a child in a nonsexist environment can contribute to childhood gender dysphoria. He notes that boys who look more stereotypically feminine and girls who look more masculine are more likely to have GID. He states, “reductions in cross-gender identity during childhood may well lower risk for subsequent transsexualism.” These assessments found him conflating gender expression with identity.
In fact, as noted by trans historian and pioneer Cristan Williams, Zucker was instrumental in including non-trans gender nonconforming people in the GID .
Even the Endocrine Society notes that the DSM-IV-TR criteria for gender identity disorder were broad and may have included cisgender children with gender nonconforming behaviors, and the DSM-IV raised several concerns over the years it was implemented. The following schematic illustrates the fundamental differences in DSM versions:
{kind=link}
Bottom Line: Blurring the differences between the DSM-IV and DSM-5 further promotes a narrative of a high desistance rate by denying that gender nonconformity was included as a pathology in the DSM-IV and the countless flawed, inconsistent, and inaccurate research studies that followed the DSM-IV criteria. Denying differences in the DSM versions allows continued classification of gender dysphoria as a mental illness and provides a claimed justification for the use of conversion therapy to “fix” a disordered identity instead of correctly defining dysphoria as the distress that many trans people experience.
Finally, the reason that gender dysphoria is even still in the DSM is to allow trans people to access healthcare. Again, the APA states:
The ultimate goal would be to categorize TGNC [Transgender and Gender Non-Conforming] treatment under an endocrine/medical diagnosis.
4. 80% Desistance Rates
Singal writes that Shrier never mentions the 80% desistance statistic, pegging it at 70% instead, and arguing:
Science-Based Medicine should correct the false claim that Abigail Shrier writes that 80% of kids desist from a trans identity, clarifying that the figure she offers is 70%, and should also clarify that in citing this figure, she is referring to the resolution of gender dysphoria, not a trans identity per se. Eckert knows that these are overlapping but different concepts.
Singal sure does like lecturing us about “false claim[s].” (He also apparently likes to make a big deal about a 10% difference between what I said Shrier said and what he says Shrier said, as though it would make Shrier so much less wrong if she really did claim a 70%, rather than an 80%, desistance rate. Citing even the 70% figure would only make Shrier slightly less wrong and quoting slightly less bogus statistics.)
What about this particular claim, though? The 80% Desistance Myth is well-known in LGBTQ Healthcare. Indeed, almost everything Shrier says on the topic alludes to this myth; Shrier writes that gender dysphoria resolves in 70% of children who identify as TGNC, a statistic she attributes to Dr. Kenneth Zucker. I explained her confusion and the use of 70% in my review, and I never state that Shrier quoted the 80% figure. I also specifically discussed the 80% statistic in context of prior research, social/cultural awareness, and trans healthcare. It is amazing how confidently Singal repeats his same line about this in slightly different forms over and over.
In any event, Singal appears to be separating “trans identity” from “gender dysphoria,” even though he should be aware what the desistance statistic implies. As I noted in my review, the desistance myth is widely disseminated to raise questions about whether we should support the transgender identities of children. Indeed, today’s desistance/detransition discourse around trans people is yesterday’s ex-gay discourse around lesbian and gay people. Both seek to invalidate the existence of gender and sexual minorities.
From my perspective, it is disingenuous for Singal to suggest that Shrier even understands the difference between trans identity and gender dysphoria, much less that she would—or could—distinguish between the two. Is Singal really suggesting that a resolution of gender dysphoria in childhood does not mean a resolution of that child’s trans identity when the literature is clear in using these desistance statistics to delay healthcare to trans youth? What exactly does Singal think “desistance” means? What specific criteria would Singal use to decide which trans youths without gender dysphoria should and should not receive gender-affirming care? Inquiring minds want to know! And know specifically!
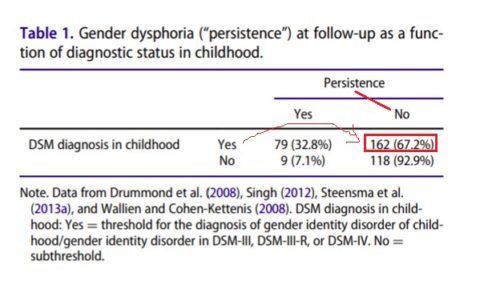
Bottom Line: The “desistance” statistic commonly cited by “gender critical” authors, whether quoted at 70%, 80%, or even 85%, is inaccurate and misleading. It has been discredited and comes from flawed, unreliable, and debunked research. In 2018, Zucker responded to (and Shrier sourced her statistic from his response) “A critical commentary on follow-up studies and ‘desistance’ theories about transgender and gender non-conforming children” by Temple Newhook et al., a journal paper that will come up again in this post, by saying:
But unless one wants to completely dismiss the validity of the childhood criteria, one must contemplate the fact that 67% of children who met the criteria in childhood were classified as desisters at follow-up.
Well, yes, that is rather the point. The validity of the childhood criteria should be dismissed because it is entirely flawed. 67% is a meaningless statistic steeped in false-positive bias.
5. No later-onset youth GD in “natal females” prior to 2012
Singal writes:
Unless Eckert can point to research suggesting otherwise, Science-Based Medicine should retract its claim that Shrier was wrong to suggest that prior to 2012, there had been no research specific to later-onset youth GD in natal females.
There are several issues with this (and Shrier’s) statement. “Late onset” gender dysphoria often only belies the delayed awareness and overall perception of the patient’s parents, especially for adolescent AFAB males. “Later-onset youth GD,” just like its newer iteration, ROGD, entirely ignores the insidious history of gatekeeping trans healthcare access. It is convenient to make a claim based in a faulty assessment. It appears Shrier is again sourcing Zucker, who writes in a 2012 article titled “Demographics, Behavior Problems, and Psychosexual Characteristics of Adolescents with Gender Identity Disorder or Transvestic Fetishism“:
What has also changed is an increase in the number of late-onset girls with GID, who were barely noticed in the clinical literature until quite recently.
Zucker’s statement refers to gender identity disorder and is entirely subjective, even though frequently repeated as fact. Late-onset dysphoria, dysphoria that occurs around puberty or later, is a complex qualifier. Some individuals knew they were trans in childhood but did not verbalize it to their parents or friends for lack of confidence and/or accurate terminology to define their gender; some do not recall signs of GD in childhood. An identity that is a surprise to those people around the trans person does not correlate with the onset of the identity for the person themselves. As aptly summarized by Zinnia Jones in reference to ROGD, “parental awareness is distinct from onset of gender dysphoria“. A formal comment on Littman’s study reports evidence that there is a low correlation between children’s self-evaluation of mental health and their parents’ assessment of their children’s mental health, especially as it pertains to non-observable states, such as emotions.
Though gender dysphoria often begins in childhood, some people may not experience it until after puberty or much later.
Adding “later-onset” or “rapid onset” to qualify gender dysphoria does not indicate a separate phenomenology or distinct diagnosis.
Bottom Line: There has in fact been research prior to 2012 on transmasculine youth with gender dysphoria disclosed in their teen years. The judgement calls made by researchers and clinicians on when GD developed are steeped in bias and misinterpretation, a common problem with the research that Singal cites.
6. Referral pattern shifts
Singal states, again with his extravagant “false claim” rhetoric:
Science-Based Medicine should correct the false claim that the Toronto clinic didn’t see the same natal-sex shift among adolescent patients as other clinics.
The study in question notes that Toronto reported a larger proportion of AMAB patients referred in childhood. For adolescents, the general trend of an inversion in sex ratios was also reported in Toronto. This is not clear in my review and has already been corrected appropriately.
The review should read:
The study found an increased ratio of adolescent referrals. Specifically, 32% were AMAB (assigned male at birth); 68% AFAB, which aligned with results from an Amsterdam clinic and Toronto clinic. The Toronto clinic did report a larger proportion of AMAB referrals in childhood.
Singal further writes:
In her references section, Shrier cites multiple gender clinics’ own reports about shifts in referral patterns. What else is she supposed to do? How is a clinic’s own data ‘anecdotal’ or ‘soft’? This is just a strange claim.
Since we are debating semantics, I’ll point out that Shrier sources four clinics to support the “shift in ratio” claim: one in Toronto, one in Amsterdam, one in the UK, and one in Sweden. To help alleviate Singal’s confusion, I will respond that “anecdotal” in this context means reporting observations and asserting causal relationships as factual. This makes the data ‘soft’ and it cannot be used to extrapolate a general trend. A broad sweeping statement about the predominance of transmasculine to transfeminine youth based on a few clinic reviews does not reflect a real change in ratios in the overall population of trans youth or apply to the general population. As bioethicist Florence Ashley notes,
Future researchers should resist the impulse to assume that shifts in assigned sex ratios reflect a change of ratio in the gender-diverse population. No evidence currently supports the thesis that the ratio of AFAB and AMAB youth has changed in the overall trans youth population.
Bottom Line: Regardless of speculation around sex ratio shifts, journalist Evan Urquhart makes the following salient points in his 2017 Slate article, “Why are Trans Youth Clinics Seeing an Uptick in Trans Boys?“:
Why has the ratio of transfeminine to transmasculine youth seeking treatment changed, and what does this shift mean? Unsurprisingly, the opponents of transgender rights have a theory: Blogs from this contingent weave a story that transness is a social mania that seeps into the minds of young “girls” and, Svengali-like, causes them to believe that they are trans. Of course, devotees of science and research-based medicine don’t have the same freedom to take an interesting phenomenon and spin a conspiracy around it…
…So should we, ultimately, care one way or the other about a trend towards a higher proportion of transmasculine youth seeking treatment in clinics that do this work? For individual trans people, the question of how and when and why people seek treatment for gender dysphoria is largely irrelevant to our personal decisions about our own medical care. For trans people who are in distress, the first concern should be treating that distress in ways that are ethical and take the most up to date research into account.
7. Littman and ROGD
Singal writes:
As is par for the course here, the linking is also confusing — that final claim about the poster includes two links that critique Littman’s research, but neither of which makes any mention of a ‘poster’ or the number 164. In the absence of accurate linking and citing, it’s effectively impossible to fact-check Eckerts’ claims.
It is quite simple to find the 2017 poster abstract. Let me refer Mr. Singal to a discussion of that poster “study” here, in which the undisclosed aspects of Littman’s study that produced bias are discussed. The history and origins of the “social contagion/ROGD” hypothesis are also quite interesting, and a detailed timeline was published here. None of this is secret or hidden or even all that difficult to find, contrary to Singal’s claims. If he was unable to “fact check” what I wrote, one wonders how good a journalist he is.
Bottom Line: The only thing Littman’s study actually elucidated was how widespread anti-trans sentiment was (and still is), to the degree that a disturbing number of otherwise logical and educated people, some even self-identified members of the skeptics movement, credulously fall for media-endorsed bias. On July 28, 2021, The Coalition for the Advancement & Application of Psychological Science released a position statement on Rapid-Onset Gender Dysphoria calling for:
…eliminating the use of ROGD and similar concepts for clinical and diagnostic application given the lack of empirical support for its existence and its likelihood of contributing to harm and mental health burden. CAAPS also encourages further research that leads to evidence-based clinical guidelines for gender-affirming care that support child and adolescent gender identity development. CAAPS opposes trainings that encourage others to utilize this concept in their clinical practice given the lack of reputable scientific evidence to support its clinical utility. Finally, CAAPS recommends expanding community education about these topics to reduce the stigma and marginalization that contribute to mental health burden.
This position statement was signed by many professional organizations in the field of mental health, including the American Psychological Association and American Psychiatric Association.
8. Slurs against SBM and my Gender and Life Affirming Medicine Program (GLAM) at Anchor Health Initiative
In his post, Singal gets personal and attacks my clinical practice with a straw man argument, writing:
This is concerning. Science-Based Medicine is platforming a youth gender clinician who is disseminating the idea that it is bad to require a clinical diagnosis prior to the administration of puberty blockers and hormones to young people. Again: What does this person’s practice in Connecticut look like?
My review actually states:
The belief that a diagnosis is clinically required to access gender affirming care, known as transmedicalism, can contribute to stigma and discrimination toward transgender individuals.
I did not say that it is “bad” to require a clinical diagnosis. I did not say “prior to”, I said “required to access,” which is very different in context, because many clinics employ an outdated model that requires a mental health provider to first assess a patient before the patient can begin any medical interventions. For someone who so frequently, for lack of better arguments, weaponizes semantics against those with whom he disagrees, Singal appears in this case to have demonstrated rather remarkable carelessness when it comes to his interpretation of my statements. Nonetheless, I’ll take this opportunity to educate Mr. Singal. The generally accepted diagnosis frequently used by gender-affirming clinics is “endocrine disorder, unspecified” (that’s ICD-10 code E34.9). Use of this diagnostic code eliminates the need to use an unnecessary and problematic mental health diagnosis.
My practice is fantastic, thank you for asking, and thanks for the Twitter follow! We won’t be following back. You can also follow us on Instagram, TikTok, and YouTube.
Singal also writes:
Science-Based Medicine is accusing a bunch of parents it doesn’t know of likely being physically abusive toward their kids, because they are skeptical their kids should go on blockers and/or hormones. Is this Eckert’s approach, in their own practice, to the inevitable disagreement that sometimes arises between parents and teens when it comes to hormones and blockers? Do they believe that when a parent has qualms about these treatments, that means they are at a high risk of physically assaulting their children? How does that affect the way they go about their job?
This is, unsurprisingly, another straw man argument. (Does anyone notice a pattern here?) My actual quote was:
Judging by the attitudes of parents surveyed, I would posit that their children were likely afraid to disclose due to minority stress factors including social stigma, fears of rejection, and very real concerns about violence.
I did not and do not say “physically abusive.” I did not refer to parents who are merely “skeptical” about placing their child on puberty blockers ± hormone treatment. (Indeed, most parents are “skeptical” at first.) What I wrote—and it is pretty clear—is that trans youth might well be afraid to come out to their parents based their perception of their parents’ attitudes and feelings regarding trans people. Given the incredible power that even parents who never employ even mild corporal punishment on their children have over their them, it should be clear to Mr. Singal that fear of physical abuse as a consequence of coming out is not a prerequisite for children to be afraid of their parents’ possible reaction to their announcing that they are transgender. Note also that I said “fear of rejection.” Being rejected by parents is a traumatic experience for any child, regardless of the reason for the rejection; rejection alone is greatly feared in and of itself even in households where there is no fear of physical violence.
Actually, speculation is unnecessary. In my practice—and Singal, not being a physician, needn’t worry about how his ridiculous claims affect my practice—there are clinical situations in which disagreements between family members arise. (It is, in fact, common.) To address these disagreements, I provide resources and references and also assess family dynamics. In brief, I provide support for patients and their families. I never say anything that implies that I see parents with qualms about gender affirming medical care as being likely to physical assault their child. I don’t say anything even close to that. It is absurd to imply that I do, and Singal’s characterization furthers a false narrative in which gender-affirming healthcare is easy to access, monolithic, and illogical.
9. A “real” trans person
Singal writes, with yet another tiresome demand to “correct” a claim that he incorrectly considers false:
But the version Eckert lays out, in which Shrier says something like People who A, B, and C are really trans, but people who X, Y, and Y aren’t doesn’t seem to appear anywhere. Unless Eckert can provide some evidence otherwise, Science-Based Medicine should correct this claim.
To answer this criticism, one has to do no more than refer Singal back to Irreversible Damage itself for its references to pervasive biological/gender essentialist beliefs; its use of made-up phrases such as “traditional dysphoria” (Irreversible Damage pages 15,16, 44, 55, 61) and disparaging comments toward transgender youth who do not embrace stereotypical masculinity. Examples of such disparaging comments from her book include:
- …they don’t want to ‘pass’
- …they reject the boy-girl dichotomy
- …they make little effort to adopt the stereotypical habits of men
- …they prefer feminine [tattoos]
- …they want to be seen as “queer”, definitely not as “cis men”
– Irreversible Damage, p.23)
- …(her) desire to be a boy was neither pronounced, severe, nor persistent
– (Irreversible Damage, p.32)
Shrier also states that gender-nonconforming people “threaten(s) to dismantle the rationale for transgender body alterations in the first place (Irreversible Damage, p.72), while describing gender-affirming therapists as blindly accepting a patient-reported gender identity, writing that therapists “must agree…that a male with gender dysphoria who identifies as a woman really is a woman” (Irreversible Damage, p.111). Shrier also characterizes transgender adults as those who “present as women and present as men”, not as men and women (Irreversible Damage, p.11).
Another egregious example occurs in Chapter 8, “The Promoted and the Demoted”, which opens with an anecdote about a mother taking her daughter bra fitting and being horrified because the lingerie specialist was a trans woman, whom she described as “six feet tall, pancake makeup blurring a stubbled jaw, two breasts grafted onto a muscular torso like add-ons”. After hearing this account from the mother, Shrier decides to go to the store and see this saleswoman herself, after which she reports “…there was no mistaking that this lingerie specialist was male” (Irreversible Damage, p.153).
Bottom Line: In Shrier’s words, in response to a YouTube video about not needing dysphoria to be trans: “those of us plagued with social anxiety are officially on notice: we’re probably ‘trans'” (Irreversible Damage, p. 61).
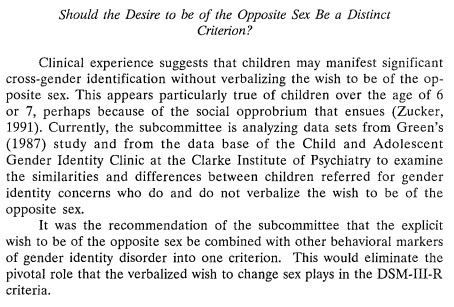
10. Zucker and Subthreshold GID
Singal sources his own widely criticized and controversial 2016 article to critique the External Review of CAMH’s Gender Identity Clinic:
[The External Review used to justify the closing] simply does not read, at any point, like a serious attempt to evaluate the Gender Identity Clinic, and it is riddled with sloppiness. From very early on, there are simple errors — CAMH’s legal counsel is described as “Kristen Sharpe” four times in the document, when her actual name is Kristin Taylor, and the reviewers note that the clinic has been around for “approximately 30 years” when it was actually founded more than 40 years ago, in 1975. More importantly, Zinck and Pignatiello quote Zucker as stating that “70% of the children we see are sub-threshold for [gender dysphoria].
He goes on to note in his critique:
Whether Zucker misspoke or the authors mistranscribed, this is exactly backwards — 70 percent of the children at the GIC did meet the clinical criteria for the condition (a statistic mentioned in [a] 2008 article and confirmed to me by former GIC clinicians). If the reviewers believed that just 30 percent of them met the criteria — they didn’t respond to an email about this — that would imply they fundamentally misunderstood what the clinic did and why it was treating most of its patients at all.
Eckert could have easily double-checked this with Zucker. I did.
The 70% statistic is indeed in the External Review, yet we are to accept Singal’s conjecture as truth. Singal treats his own assessment of the External Review as fact, even though the phrases “does not read…like a serious attempt” and “riddled with sloppiness” are hyperbolic speculation. The reviewers did not respond to Singal, which is not surprising. The belief in 70% would not “imply they (the reviewers) fundamentally misunderstood what the clinic did,” as Singal writes. He’s wrong about this. They were aware of what the clinic did.
Nonetheless, unfazed, Singal maintains:
It’s an internet rumor I debunked in 2016. Most of the kids in the Zucker clinic had what was then called GID — above 60% in every study I’ve seen. Science-Based Medicine is misrepresenting a body of research in a way that is staggeringly sloppy — you can really just check the studies themselves and see that Eckert gets this completely wrong.
And in a separate point that is the exact same argument, Singal states:
Eckert writes: “[I]nvestigators reviewed his patient files and found that 72% of the children treated by Zucker never met the clinical criteria for gender dysphoria[.]” Again, this is a very stale internet rumor that was debunked in 2016. There is no paper anywhere where Zucker says this.
Characteristically Singal appears to have the audacity to believe that this particular statistic has been definitively “debunked” on the basis of his biased, myopic article arguing against it. Singal’s article did not “debunk” the statistic. Quite the contrary, his article was “debunked“, if we are using Singal’s definitions. Here are some other “stale internet rumors”: Singal is an expert in transgender youth; gender diverse children can’t possibly know who they are yet (as bolstered by Zucker’s study purporting a developmental lag in children with GID and their gender constancy acquisition); and ROGD is real and not a completely fake, unscientific, transphobic theory.
Characteristically, Singal’s argument in this case once again hinges on conflation of the DSM-IV and DSM-5. As I noted earlier, gender nonconforming behavior was indeed treated as GID in many cases. Singal’s statement that over 60% of kids in Zucker’s clinic had GID is in itself a “stale internet rumor,” hinging on—again—the DSM-IV GID criteria that allowed for diagnosis without any “explicit wish to the of the opposite sex,” which, as Kelley Winters writes in her 2016 response to Singal’s claims, was “a loophole that sidestepped gender dysphoria”.
Brynn Tannehill notes that 90% of Zucker’s young patients were never trans in the first place, while Dr. Kristina Olson noted the following:
Perhaps the clearest evidence that most children in these samples were never transgender to begin with is that, when they were directly asked “are you a boy or a girl” as part of a battery of intake questions, an overwhelming percentage (more than 90 percent) of children in these clinics provided the answer that aligned with their natal sex.
A 2018 study concludes that research framed in the GID criteria has limited utility, as those children categorized under GID may have never asserted a trans identity or asserted a non-binary identity that was not identified as anything but desistance since it did not entail a binary transition, and the studies did not examine the harms of identity suppression.
Why would I double-check my research with a person whose approach is guided by the understanding that being trans is a mental illness instead of a normal variation and utilizes treatment that discourages gender nonconforming behaviors in order to avoid trans outcomes even though the scientific consensus is overwhelmingly in favor of the gender affirmative approach?
Singal recently tweeted out the same argument with the same poorly interpreted information:
Unlike Jesse Singal, both Dr. Lovell and myself have busy medical practices and responding to arguments that have been previously addressed and debunked or semantics that do not change the context of the posts is not a top priority for us. Mea culpa.
The full Twitter thread:
Singal is missing the context of the link. The link shows where Abigail Shrier lifted the 70% desistance rate number from: an article written by Zucker in response to criticism of desistance research.
Singal’s weird mathematics do not even apply here. I was including 70% as context for Shrier’s statement. If Singal has issue with the 70% number, he should bring it up with Abigail Shrier, who quotes it, attributed to Zucker, in her book. Similarly to Singal, though for very different reasons, I do not agree that the percentage of desistance is 70%; this has been thoroughly explained in my review.
Zucker does in fact state that 70% of children he saw at his clinic did not have gender dysphoria in the first place:
Zucker denies that he made this statement; we are apparently to take his denial as absolute truth. The full External Review (as sourced above) was removed and replaced by an executive summary following Zucker’s issue of a notice of libel against The Varsity; as noted in a 2016 article:
The content of the review has come under suspicion since its release. The CAMH summary alludes to the possibility that some statements included in the initial review may be been “erroneous.”
As noted earlier, Singal characterizes the External Review with the phrases “does not read…like a serious attempt” and “riddled with sloppiness.” Alluding to the possibility of erroneous statements does not discredit the entire report, and, without details on what was and wasn’t correctly relayed in the report, disavowing the entire Review is ludicrous.
Additionally, “met the threshold for Gender Identity Disorder” is different from having gender dysphoria. What Singal omits is that the DSM-IV, as previously discussed, allowed for those with differences in gender expression to be categorized under GID. These children did not have to have gender dysphoria and/or did not identify as trans yet were diagnosed with gender identity disorder. No wonder such a high percentage would “desist,” according to Zucker’s categorization. They were not trans to begin with.
Singal goes on for several more paragraphs defending Zucker, including the following:
To repeat, Zucker was later given more than a half a million Canadian dollars after his hospital acknowledged having libeled him during a demonstrably haphazard and sloppy ‘review.’ Of course SBM readers arriving to this controversy fresh will have no way of knowing that. It’s journalistically inexcusable to, in two consecutive articles in this series, simply leave out this fact. Now, does this fact, on its own, exculpate Zucker? Of course it doesn’t. But you can’t say “This guy was fired from his job!” without adding the very relevant followup “…and then his employer admitted to having done him wrong and paid him half a million dollars.” It’s just off-the-charts dishonesty by omission. And again: All the omissions, across multiple SBM articles, point in one direction. Zucker is one of Shrier’s sources and is treated credibly by her, so SBM readers need to know he is Bad, with zero countervailing evidence allowed in. The same pattern, over and over and over. Can’t be an accident.
Zucker was dismissed from his position. A petition calling for Zucker’s removal circulated for months before his dismissal. Many were concerned about Zucker’s practices years before his clinic was shuttered. Indeed, CAMH director Dr. Kwame McKenzie apologized for the clinic’s out of step approach and wound down clinic services.
Zucker filed a lawsuit in January 2016 against CAMH for defamation and wrongful dismissal. A 2018 CBC News article elucidates the reasoning behind the lawsuit:
The Toronto-based centre (CAMH) said the report wrongly stated that Zucker referred to a patient as “hairy little vermin” among other errors. It noted the report was made public without Zucker’s review or comment…CAMH apologizes without reservation to Dr. Zucker for the flaws in the process that led to errors in the report not being discovered and has entered into a settlement with Dr. Zucker that includes a financial payment to him.
Zucker did not actually win the lawsuit but entered into a settlement agreement. The minutes of the settlement have been posted on CAMH’s website. Following Zucker’s lawsuit and its settlement, CAMH released a statement including the following:
CAMH stands by its decision to close the child and youth gender identity clinic following an external review which concluded the clinic was not meeting the needs of gender expansive and trans children and their families. We believe our modernized approach to delivering services to youth better supports diverse patients through best practice and timely care.
Zucker has also filed legal complaints against those who have spoken out against the treatment of trans kids at CAMH’s Youth and Family Gender Identity Clinic. Pharmakontario, Journal of Social Justice, Mental Health, Psychedelics and Pharmaceuticals, published an article in 2020 that provides a timeline of the CAMH Gender Clinic controversy:
In 2015, Members of Rainbow Health Ontario, a provincial health promotion and navigation organization, approached the Centre for Addiction and Mental Health expressing their concerns regarding Zucker’s Gender Identity Service, alleging that there were cases of suicide of transgender youth which resulted from methods used by Zucker. Consequently, also in 2015, the Ontario provincial parliament introduced legislation banning gender reparative therapy, leading to changes to the Regulated Health Professions Act which guides the conduct of all doctors in the province. CAMH stopped the clinic from accepting new patients and initiated an external review of the clinic’s practices.
…The external reviewers, child and adolescent psychiatrists Suzanne Zinck of Halifax and Antonio Pignatiello of Toronto, invited stakeholders to comment on their experiences in the clinic. A former client, now an adult, claimed Zucker “asked him to remove his shirt in front of other clinicians present, laughed when he complied, and then referred to him as a ‘hairy little vermin’.”
…In fairness to Dr. Zucker, the claim made by the client who accused him of calling him a “vermin” later withdrew his accusation, which was reported as having been false. After the lawsuit, CAMH again apologized to Zucker, rather than to the general public, and settled for $586,000 in damages, legal fees, and interest.
Zucker is not “bad” because he is one of Shrier’s sources. Gender affirming healthcare, as I have stated and referenced ad nauseum, is, for all of its strengths and weaknesses, the current standard of care. Zucker and Shrier fundamentally disagree with this model of care, even though prior care models have been ineffective and demonstrably harmful to trans people. Also, Zucker has historically been one of the major proponents of the 80% desistance myth. Singal alludes to SBM favoring politics over science, a strategy exploited by conservative groups in defense of outdated treatment of trans people, such as conversion therapy.
Treatment for children with GID often proceeds on two fronts: 1) individual therapy with the child, in which efforts are made to understand the factors that seem to fuel the fantasy of wanting to become a member of the opposite sex and then to resolve them; 2) parent counseling, in which efforts are made to help the child, in the naturalistic environment, to feel more comfortable about being a boy or a girl. Treatment can address several issues: for youngsters who are quite confused about their gender identity, one can focus on the mastery of basic cognitive concepts of gender, including correct identification of the self as a boy or a girl; encouragement in the development of same-sex friendships, in which areas of mutual interest can be identified; and exploration of factors within the family that might be contributing to the gender identity conflict.
With parents, treatment issues include the following: limit setting of cross-gender behavior and encouragement of gender-neutral or sex-typical activities; factors within the family matrix that may be contributing to the child’s gender identity conflict; and parent factors, including psychiatric impairment, that may be compromising functioning in the parental role in general…
From a psychoeducational point of view, one rationale for limit setting is that if parents allow their child to continue to engage in cross-gender behavior, the GID is in effect being tolerated, if not reinforced. Therefore, such an approach contributes to the perpetuation of the condition.
As ER physician and transgender healthcare specialist Dr. Madeline Deutsch notes:
The reason there is such dislike of and distrust for Dr. Zucker in the community is because he holds a position of immense power. Since he publishes so widely, and edits an influential journal in the field, Zucker’s opinions matter. (His opinions) fail to incorporate the very real empiric findings and experiences of other experts in the field, experienced clinicians, and activists … and instead remain focused on attempting to prove his own theories.
Bottom Line: Regardless of any defense or reasoning, the report concluded that Zucker’s clinic was ‘out of step’ with modern healthcare. Singal states, “Surely genuine conversion therapy is harmful,” as if there is some distinction between genuine and not. (What does he even mean by “genuine” conversion therapy, anyway?) Any attempt to change or “fix” a sexual or gender minority identity is conversion therapy, a failed, harmful, stigmatizing practice.
11. Criticism of points related to A Critical Commentary on Follow-Up Studies and “Desistance” Theories about Transgender and Gender-Nonconforming Children
Next, Singal focuses on a critical commentary that refutes his ideological beliefs, and specifically on a statement from my review:
Research was limited to those children whose parents brought them to the clinic for diagnosis and treatment, believing that their child’s identity was a problem requiring psychiatric treatment.
The study itself states that “…research was limited to children whose parents chose to bring them to a clinic for diagnosis and treatment and thus may have believed the child’s difference was a problem, and one that required psychological treatment.”
Singal responds:
Science-Based Medicine should correct the much too strong, false claim that these studies were only conducted on kids who parents brought them into gender clinics because they believed their very identities required psychiatric treatment and should correct and address this minor instance of plagiarism.
The entire argument Singal makes here is based in speculation. He cannot know that the claim is false, especially in the historical context. We can correct a “minor instance of plagiarism,” a claim that factually changes nothing, although doing so is admittedly difficult when over the last two months neither Dr. Gorski, Dr. Novella, nor I have been able to figure out what has been “plagiarized.” (I’m sure that Mr. Singal will be more than happy to help us out, given his history of calling out “errors,” whether errors or not, in SBM’s writings about transgender medicine.) The point of the Critical Commentary article and my review is to debunk the myth of the high desistance rate, a rate that is used to promote a cautious and skeptical approach that does not trust youths’ asserted gender identities.
Singal counters that:
Setting aside the minor plagiarism issue (minor given that Eckert only steals part of one sentence, but to be clear this is plagiarism, albeit of the misdemeanor variety in which a traditional outlet would rush up an explanation that it was just a matter of a forgotten links or quotes or both), it’s worth noting the aforementioned response piece from the Dutch clinicians themselves:
[T]he two remaining [desistance] studies [being discussed] come from two clinics with very different social contexts. The Toronto and Amsterdam clinical populations are not similar. This is illustrated clearly by a number of comparative studies on the social and emotional functioning of children and adolescents who are referred to the two clinics: in all studies psychological functioning in children and adolescents (measured through parental, teacher and/or self-report) showed to be better in Amsterdam than in Toronto (Cohen-Kettenis, Owen, Kaijser, & Bradley, 2003; de Vries, Steensma, VanderLaan, Cohen-Kettenis, & Zucker, 2016; Steensma et al., 2014). As noted in the discussions of these papers, we believe that differences in the social climate regarding gender variance may be an important factor underlying the differences. A sociometric study on peer group status (Wallien, Veentra, Kreukels, & Cohen-Kettenis, 2010) underscores this point. It was shown that there were no differences between gender-referred elementary school children and their classmates in victimization or bullying. Parents who come to our clinic are concerned about potential harm for their child if they would not acknowledge the child’s gender experience. They are not focused on suppressing it, as the authors suggest by the sentence: [The sentence I quoted above.]
One might expect a journalist to know that “the authors suggest” is not the same as “the authors stated.” This semantic quibble obscures the point of the statement, which is that research was limited to those children seen in clinics (vs children who were not). The reasoning for writing “difference was a problem” aligns with the DSM-IV model, which was in use at the time. The logorrheic paragraphs Singal expends on this do nothing to elucidate the point the authors of the Critical Commentary are making – research data gathered in clinics can only study those children seen at the clinics. The authors of the article responded to Zucker’s response here.
Bottom Line: Regardless of Singal’s claims, approaches such as watchful waiting and conversion treatment are not up to the current medical standards. Of course, that appears to be Singal’s modus operandi: arguing semantics and presenting what on the surface look like “gotchas” to give the appearance of having invalidated research that does not fit his narrative.
As GLAAD notes, desistance is uncommon—rare, even. Emphasis on the few patients who demonstrate desistance undermines gender affirming approaches to healthcare. This is not the first time Singal has attempted to defend an unscientific stance on desistance. There are numerous reasons why Singal ended up on GLAAD’s Accountability Project (as has Shrier), a “resource for journalists and the general public which documents anti-LGBTQ words and actions from politicians, commentators, organization heads, journalists, and other public figures who are often quoted in mainstream media about LGBTQ issues”.
Trans activist, writer, and scientist Julia Serano has detailed her personal interactions with Singal in excruciating detail. Nor has she been Singal’s only target. There is nothing new to see in his most recent criticisms of SBM, many of which are based primarily on semantics and obscure good faith discussion and scientific evidence. It is mind-boggling to me that a cisgender journalist with no research background is apparently considered by so many to be a leading resource on trans issues, especially given his habit of ignoring the context of social issues that impact trans lives and the insidious history of pathologizing trans identities, while spreading harmful misinformation.
As Dr. Turban (another favorite Singal target) notes of studies claiming social contagion and ROGD:
What is the reason for this research? What does it hope to accomplish? The tireless search reveals a thinly veiled dogma: that being transgender is a pathology to be fixed. This belief not only harms transgender people but also undermines good science.
For all of its areas of uncertainty and ambiguity, gender-affirming medicine is the current standard of care for trans adolescents because it is based on the best existing science. That science has weaknesses and holes, as does all medical science, but Singal has not been able to demonstrate based on science that his preferred approach (that is, when he even articulates an approach other than to attack gender-affirming care) will result in better medical outcomes for trans youths. Unlike Singal, physicians caring for patients now rarely have the luxury of waiting for more rigorous science to decide how to act and have to do what they can for patients based on existing science. Fortunately, like all science, the science of gender and transgender care is ever-evolving (and, hopefully, progressing). As is the case with all science- and evidence-based medicine, when better standards of care for trans people are developed based on new and better scientific and clinical research, we will adjust our practices accordingly to conform with the latest scientific findings. That is how science- and evidence-based medicine works, something that Singal seems not to understand.