{kind=link}

Despite the marketing, there is no need for you to take most supplements. And no-one needs coconut oil chews.
As healthcare systems struggle to cope with growing and aging populations, there is renewed interest in eliminating wasteful, and possibly harmful, care. The Choosing Wisely campaign suggests that up to 30% of health care services may be unnecessary. Driven by the medical profession itself, Choosing Wisely is challenging both patients and health care providers to have an honest dialogue about the appropriateness of care. What is increasingly obvious is that ineffective and inappropriate medical care can’t be counted on to disappear naturally, even when the evidence is clear and is acknowledged by health professionals.
Dietary supplements are an enormously popular category of consumer products (I hesitate to call them health products), usually taken with the objective of promoting or supporting health. In the US alone, supplements are a $34 billion dollar industry. I’ve posted several times about trends in supplement use, looking at some of the larger studies to understand who takes supplements, and why. As a pharmacist who has worked in both community (retail) and hospital pharmacy practice, my own observations seem in line with what the evidence shows. The extent to which some consumers embrace supplements as part of their health activities is remarkable. I have seen people spend hundreds of dollars per month on dietary supplements based solely on the advice of a naturopath or other alternative medicine provider. And as a former hospital pharmacist responsible for doing medication histories with new patients, I would regularly encounter seniors taking dozens of different types of vitamins, over-the-counter medications, supplements and tonics, often with contradictory purposes: the “natural” laxatives with the anti-diarrheal medicine, or combinations of products for a single use, like melatonin and diphenhydramine for sleep. Cleaning up the supplement schedules to something rational (or at least safe) was one of the more challenging aspects of my role. Like medication, consumers can get very attached to their supplements, sometimes attributing beneficial effects to them that were highly implausible, and more likely reflected placebo effects. Convincing people that the supplements they’re taking are unnecessary, and even potentially harmful, can be difficult. Some have been so convinced of the merits of their (usually self-driven) supplement strategy that they would take suggestions very personally, as if I were questioning their own judgement. Such is the nature of the supplement industry: A triumph of marketing and an unquestioned boon for manufacturers, but billions in spending with little evidence that supplements have any real health benefits whatsoever.
We didn’t become widespread consumers of dietary supplements by accident. The growth in supplement consumption has been driven by highly effective marketing based around the invented idea that dietary supplements are necessary for good health. This message was given tacit approval by regulators who have traditionally used a light hand when it comes to holding supplement companies accountable for marketing products that are safe and effective. The Dietary Supplement Health and Education Act of 1994 (DSHEA) was an amendment to the U.S. Federal Food, Drug and Cosmetic Act that established the American regulatory framework for dietary supplements. It effectively excludes manufacturers of these products from virtually all regulations that are in place for prescription and over-the-counter drugs, and puts the requirement to demonstrate harm on the FDA, rather than the onus on the manufacturer to show a product is safe and effective. The goal was to eliminate barriers to sale, and it worked: Within four years of the DSHEA, supplement sales grew from $4 billion to $12 billion. And the market has almost tripled since then.
A new study looks at trends in supplement use over a thirteen year period. Published last month in the Journal of the American Medical Association (JAMA), “Trends in Dietary Supplement Use Among US Adults From 1999-2012” is from Elizabeth D. Kantor and colleagues at the Memorial Sloan Kettering Cancer Center. This is a cross-sectional study of National Health and Nutrition Examination Survey (NHANES) collected between 1999 and 2012, which examined American residents who were not in a nursing home. Data was collected via in-home interviews, and participants were asked about any supplement use in the past 30 days. Given the thousands of products sold as “supplements”, the investigators sought to categorize products in a similar way. Multivitamins and mineral supplements were defined as a product with >9 vitamins and/or minerals. There were also queries about individual vitamins as well as non-vitamins supplements. Consequently, an ingredient like vitamin C could be considered a multivitamin or a specific vitamin supplement, depending on how it was packaged. For each type of vitamin or supplement, the usage over time was examined and statistical significance was calculated. Data collected was also stratified by age, race/ethnicity, and education level.
Results
This was a large study, with almost 38,000 participants in total, or over 5,000 participants per two-year cycle. The mean age was 46 and the sample was 52% women. In 2011/12, 52% of adults reported using a supplement in the past 30 days. When looking at the stratified data, there are some interesting (but perhaps not surprising) observations. Older adults use more supplements. Women use more supplements than men. White adults use the most supplements. Those with the most formal education used the most supplements. And those with the highest-reported health status used the most supplements:
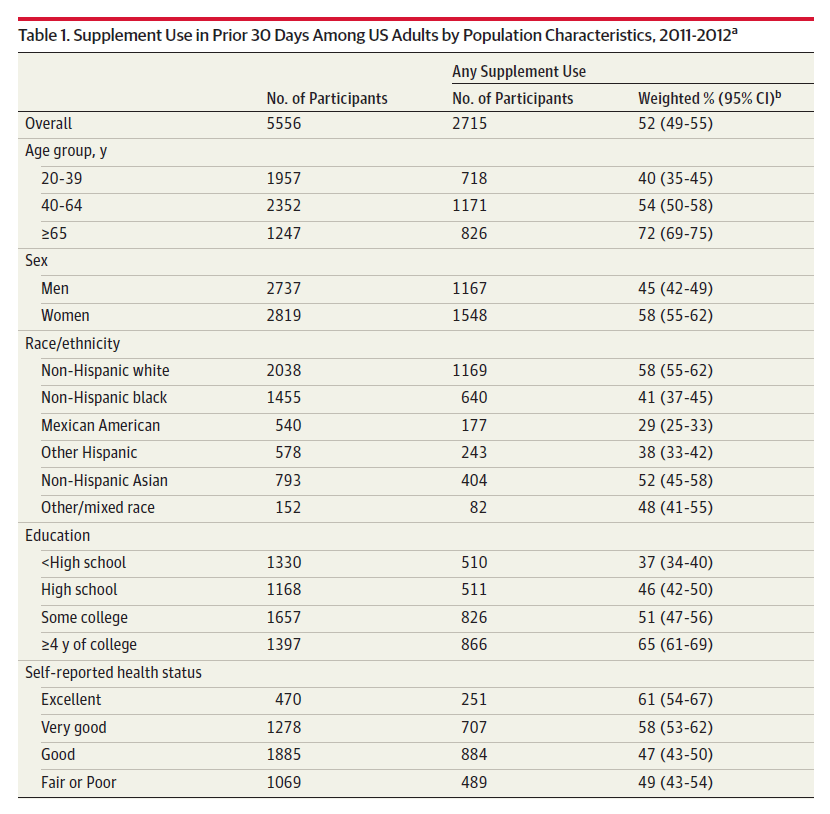
When you examine usage over time, it’s a bit like a time machine, where you can see changing trends which appear to have been driven by hype, but also (let’s hope) influenced by scientific evidence. There are tables and tables of data, and I’ve pulled out a few highlights. For example:
- Consumption of multivitamins had decreased overall (37% to 31%, comparing 1999/2000 vs. 2011/12), possibly driven by studies showing they are largely unnecessary and offer no meaningful benefit.
- Vitamin D usage as a single ingredient supplement has increased over time (5% to 19%), likely influenced by science, but also hype and buzz.
- Omega-3 fatty acids consumption has grown over time (1.9% vs. 13%, respectively), possibly influenced by greater awareness of expected benefits of fatty fish consumption, which has been translated by the supplement industry into marketable products.
- Decreases in the use of Echinacea, garlic, Ginkgo biloba and ginseng, likely influenced by studies which have shown these supplements have no real health benefits.
Trends in usage were also described, which shows some interesting features. For example, usage of supplements is decreasing among younger adults:

American supplement use trends by age, sex, ethnicity, and education (Kantor et al., click to embiggen).
Implications
A “glass-half-empty” perspective on this evidence would point to the widespread use, billions in expenditures, and no objective benefits, and question the effectiveness of health professionals’ efforts to help consumers choose more wisely. A more optimistic perspective might point to the flat overall usage and the declining usage in many categories of products, some of which may have been influenced by broader consumer uptake of the scientific evidence that has emerged. If it weren’t for growing usage of products like vitamin D and fish oil supplements (which are at least less likely to be harmful that many other supplements), the overall trend in usage might even be negative. This is what we should expect, given the state of the evidence for dietary supplements: There is little information to suggest that routine supplementation is necessary in most cases. There is also growing evidence to show that supplementation may be harmful, whether it’s acute supplement toxicity, or harms from chronic use. But this is still a $34 billion industry, and there are many areas were we could probably direct that health spending more effectively. Moreover there are choices we can all make that will be demonstrably more effective than any supplement ever marketed, and cost nothing, like getting more exercise.
An editorial that accompanies this study asks why usage is still so high, despite the evidence:
One factor may simply be that consumers are not aware of these negative results, and so continue to use the products they have been using for years. In these cases, the onus is on clinicians to inform patients when the evidence has changed. Other consumers might not have faith in the scientific process, in which case counseling is unlikely to result in significant changes in supplement use.
Another factor may be that these findings are counter-intuitive: avoiding a multivitamin seems to run counter to everything patients have been taught about the importance of consuming enough vitamins and minerals. Physicians can help remind patients that there is no benefit of obtaining vitamins from a pill rather than from conventional food.
A third factor is that the law affords manufacturers significant leeway to advertise supplements for a broad spectrum of conditions. DSHEA permits the promotion of supplements using “structure/function claims.” For example, claims such as “supplement X will preserve heart health” or “supplement Y will maintain mental alertness” are permitted without premarketing authorization from the FDA. Such claims must be accompanied by a disclaimer: “These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.” However, the disclaimer appears to have minimal effect on consumer understanding of the advertised claim.
Moreover, even after high-quality studies that show no meaningful clinical differences between supplements and placebos are published, the law provides manufacturers latitude to continue advertising their products based on earlier, low-quality data. For example, Ginkgo biloba continues to be sold “to support mental sharpness” despite a large, high-quality NIH-funded study that found evidence to the contrary. In the study by Kantor et al, when the consumption of some products declined over time, consumption of other products increased and made up for the deficit. It might be that companies refocused advertising from one supplement to another. In response to research findings showing no substantial benefit for garlic and glucosamine, for example, manufacturers may have turned to preliminary findings to promote coenzyme Q10 for heart health or methylsulfonylmethane for joint health.
Rx: Better education and more effective regulation
What are the key takeaways from this study? The first is that supplement use is very common and needs to be considered alongside prescription medications as products that can potentially be causing drug-related harms, or drug-supplement interactions. The second is that evidence seems to be having an effect, but doing the research and publishing it isn’t enough. We need better communication about the lack of benefits and the risks, recognizing that we’re up against a powerful marketing machine. To help, we need to create a more transparent market for consumers. We need better regulation to ensure that consumers can easily access and understand the scientific facts supporting any particular supplement. Moreover, we need health professionals (like pharmacists) to actively advocate for patient interests above the desire to sell anything, and to stop giving supplements a veneer of health legitimacy. There is a place for, and even a need for, dietary supplements as part of good health. But widespread access and a lack of good advice is contributing to billions in waste.