
{kind=link}
I realize that I say it perhaps far too often, but, truly, since COVID-19 hit four years ago everything old is new again. It started out with everything old being new again in the world of antivaccine misinformation, complete with false claims of infertility, death, cancer, and the same old, same old “vaccine injuries” due to COVID-19 vaccines. Then, as predictably as night follows day follows night, “new school” antivaxxers started to embrace “old school” antivax tropes and became just antivax. Then, given the affinity between quackery and antivax, “new school” antivaxxers started embracing more general quackery, including cancer quackery, as they quickly “repurposed” drugs that they claimed as effective against COVID-19 (e.g., ivermectin) to treat cancer and then embraced other more general quackery, including even homeopathy. So it should come as no surprise that co-founder of that group of COVID-19 cranks known as the Frontline COVID-19 Critical Care Alliance (FLCCC Alliance), Dr. Paul Marik, is now promoting a very old narrative long promoted by cancer quacks that chemotherapy doesn’t work.
It’s so obviously the old narrative in that the claim goes further than that, to say that chemotherapy “only cures” 5% of all cancers. Sound familiar? It should. I’ve written about it before, although back in the day it was claimed that “only 2%” of cancers were curable with chemotherapy. That’s why, seeing this old trope again all these years later, I felt that I should see what new form it’s taken and what new, if any, evidence Marik cherry picks to try to promote this misleading impression, while being surprised that quacks have now admitted more than double the efficacy of chemotherapy compared to what they used to admit.
I had seen mentions of Marik’s earlier in the week, but what really tweaked me to write about this yesterday, as I was perusing my usual sources, was seeing former Trump administration HHS science advisor Dr. Paul “We Want Them Infected” Alexander promoting this claim in a Substack post with one of his characteristically annoying and lengthy headlines that read BOOM! 2nd Smartest Guy in the World (support this stack) again delivers a seminal piece with a hero of mine, Dr. Paul Marik on the fraud of cancer chemotherapy; never worked!
As an aside, what is it with the “BOOM!” in so many right wing articles and social media posts? Whenever I see that “BOOM!” I can’t help but be reminded of Marvin the Martian, because there usually is no “BOOM!” in these “exposés,” except in the deluded head of someone like Alexander:
But I digress.
It was the blurb for Alexander’s Substack entry that got my attention:
Just like the Malone Bourla Bancel COVID mRNA vaccine, it never worked, it worked in your head! Marik: “only “about 5% of all cancers are actually curable with chemotherapy.” not for 95%
And there you go. Sure, it’s not 2%, but it is only 5%. I was also amused, mainly because it very quickly became clear to me that Marik is not up-to-date with respect to cancer chemotherapy, given the claims that he spews. I am more than happy to slap him in the face with some actual data. Alexander, Marik, and the self-proclaimed “2nd Smartest Guy in the World” (2ndSGitW) also willfully misunderstand that most cancers these days are treated with multimodality therapy that can include a combination of any or all of modalities including surgery, chemotherapy, radiation therapy, immunotherapy, endocrine therapy, and targeted therapies, the exact combination and identities of which depend on the tumor type, stage, and overall health of the cancer patient. Few cancers, mainly hematologic malignancies, are treated with just chemotherapy anymore.
The article being referred to by Alexander and 2SGitW was published early last week by the disinformation spreader The Vigilant Fox under the title, Dr. Paul Marik Exposes the Truth About Chemotherapy, with the tagline, “You won‘t hear this from your typical oncologist.” Of course, there’s a reason you “won’t hear this from your typical oncologist,” mainly because it’s, to put it mildly, bullshit. Also, one can’t help but note that Marik isn’t even an oncologist or any specialist related to oncology. I mean, holy hell, as much as I can’t stand Dr. William “turbo cancer” Makis, at least as a nuclear medicine radiologist he did image cancer patients and use some targeted radiotherapies to treat some cancer patients back in the day before he lost his medical license. Marik doesn’t even have that tenuous link to oncology. I also note that there is what I would call a paucity of actual citations to the literature—or any sources other than Marik—in this article. There is, however, a link to the FLCCC page on The Role of Repurposed Drugs and Metabolic Interventions in Treating Cancer, where I hoped to find the “rationale” (such as it is) for Marik’s claims.
Paul Marik echoes cancer quacks going back at least 50 years
Let’s start the discussion of the “meat” of Marik’s claim (if you can call it that) by seeing what Marik says, at least in his interview with The Vigilant Fox:
Dr. Paul Marik, a renowned critical care physician, has shed light on the harsh realities of chemotherapy’s ineffectiveness in treating cancer. He revealed that only “about 5% of all cancers are actually curable with chemotherapy.”
This small fraction of cancers that are chemo-responsive includes testicular cancer, Hodgkin’s lymphoma, acute lymphatic leukemia, and a short list of others. (See image below)
The image is this:
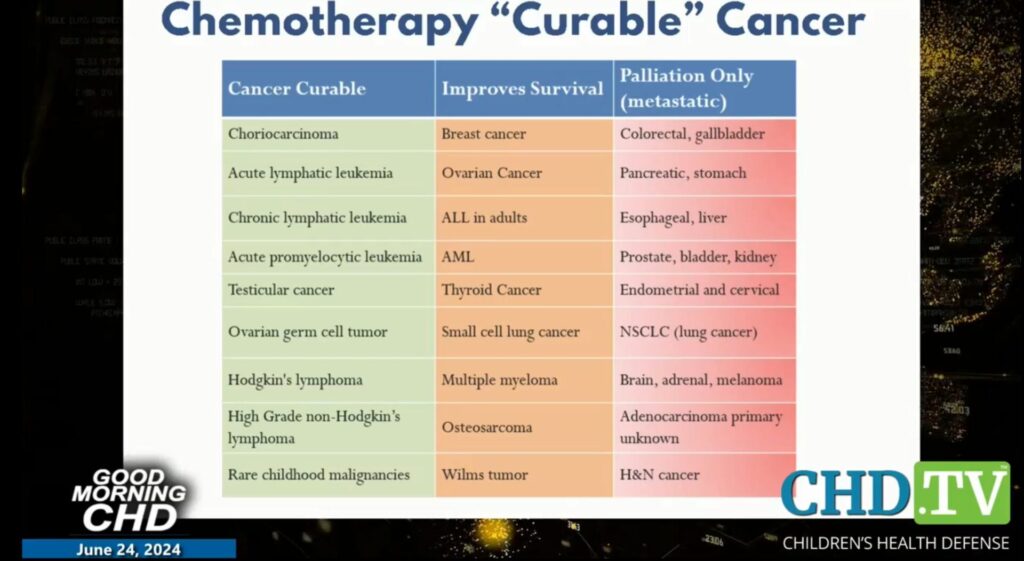
I tried to find a source to back up Marik’s claim, both in his e-book and slideset, and was unable to locate one. Quelle surprise. Marik also says:
But for the remaining 95% of cancer cases, the prognosis is far less optimistic. Dr. Marik stated, “Chemotherapy is palliative at best,” highlighting that while chemotherapy might prolong survival by one or two months, it comes with a significant cost to the patient’s quality of life.
And:
The truly sobering detail that Dr. Marik mentioned was that despite advancements in chemotherapy, immunotherapy, and surgical treatments over the past 30 years, the overall life expectancy of a cancer patient has been extended by a measly 3.9 months.
Again, this is highly deceptive, and Marik provides no citations. He also conflates the minority of cancers that are diagnosed when metastatic, for most of which chemotherapy is palliative and likely only to provide a survival improvement on the order of months, with the earlier stage, operable, treatable cancers that make up what most cancer patients are diagnosed with. Marik’s conflation of the two is highly deceptive.
As I’m sure that any actual oncologist reading this post will immediately recognize, this is an example of the misrepresentation and outright omission. First of all, it’s deceptive to include a column of metastatic disease in a slide about chemotherapy “curable” cancer, because, with rare exceptions (e.g., testicular cancer, for which even stage IV disease is still potentially curable with chemotherapy, surgery, and radiation—just ask Lance Armstrong), chemotherapy for stage IV disease is almost always palliative. Moreover, Marik’s antivax “thinking” is at play here, in that, just as antivaxxers seem to think that any endpoint other than death (e.g., severe illness) is not important with respect to COVID-19 interventions, he seems to think that palliation of advanced cancer is worthless. While palliative chemotherapy might not prolong survival by long for many of these cancers, contrary to this stereotype, it can prevent cancer-related complications and improve quality of remaining life.
There are also curious—and glaring—omissions and inclusions in the “prolongs survival” part of this chart. For example, chemotherapy most definitely does prolong survival when used as adjuvant therapy after surgery for colorectal cancer, which makes its omission from the “improves survival” group basically a lie by omission. For colon cancer that is stage III (or high risk stage II), chemotherapy is recommended and does decrease the risk of recurrence and prolong survival, even as scientists are further personalizing treatment. Also, multiple myeloma should be in the “potentially curable” column, as chemotherapy can result in long term survival. It is true, of course, that these days monoclonal antibodies (e.g., against CD38 or SLAMF7) play an important role in multiple myeloma treatment, but high dose chemotherapy and stem cell rescue (bone marrow transplant, BMT) can be curative for more advanced disease. (I have a childhood friend who underwent BMT for multiple myeloma and has been disease-free for years. I even recently bumped into her at my cancer center as she came in for a followup visit with her oncologist.) I was also puzzled by the inclusion of thyroid cancer in the “improves survival” column. Most thyroid cancer is treated with surgery alone, sometimes with radioactive iodine to ablate remaining microscopic disease. Chemotherapy is rarely used for thyroid cancer and, when it is, is usually palliative for a particularly nasty—and, fortunately, rare—subtype, anaplastic thyroid cancer.
Finally, let’s look at the cancer that I treat routinely, breast cancer, the second most common cause of cancer death in the US in women. Approximately one-third of all breast cancers are either triple-negative (they do not make estrogen or progesterone receptor proteins) or HER2(+) (they have amplified HER2 oncogene). For these cancers, as I like to say, the oncologists might be putting us surgeons out of business. Here’s what I mean. Using the KEYNOTE-522 regimen (neoadjuvant chemotherapy plus immunotherapy) before surgery for triple-negative breast cancer, we see a greater than 60% pathologic complete response rate; i.e., there is no viable cancer seen by pathologists in the resection specimens. Results are so good that there are now clinical trials being carried out to determine whether surgery is even necessary after a clinical complete response (tumor no longer detectable on imaging studies) and how to determine whether a clinical complete response equates to a pathologic complete response. Similar results are being achieved for HER2-positive cancers after treatment with chemotherapy plus the HER2-targeting drugs trastuzumab and pertuzumab, which produce pathologic complete response rates almost as high as KEYNOTE-522 does for triple-negative breast cancer. As I said, five or ten years from now surgery might not even be necessary for up to one-third of breast cancers. (Good thing I plan on retiring within a decade.)
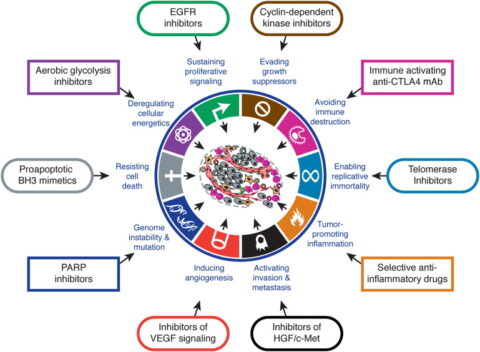
I could go on, but will for now leave finding additional errors, omissions, and dubious choices for this chart as an exercise for the reader, particularly my oncologist colleagues. Think of it this way. There are already so many errors, dubious placements, and questionable categorizations in the chart that it should make you doubt everything else that Marik says, given that he can’t even get this chart right. As for the chart itself, it didn’t take me long to see that it came from a Webinar slideset on the FLCCC website that so flagrantly mixes nonsense with facts that I could (and maybe should) do a series picking it apart, or perhaps picking apart, chapter by chapter, Marik’s cancer quackery e-book on the website, shown below with its cover and Table of Contents:
Does Marik’s claim have any validity? I suspect you know the answer: It’s a grain of truth distorted.
Paul Marik vs cancer science
Looking at all of this, I wondered where Marik got his figure of “only 5%” of cancers being cured with chemotherapy; so I subjected myself to the CHD podcast in which Polley interviewed him. It was less than three minutes in that Marik was repeating the straw man about cancer beloved of quacks, one that I’ve discussed so many times that Marik’s repetition of it probably caused injury to my extraocular muscles, so hard did I roll my eyes. In brief, Marik claimed that oncologists would say that cancer is caused by mutations and chromosomal abnormalities, when in reality it’s a “metabolic disease.” (And, yes, he did invoke Otto Warburg, who first proposed this idea in 1928.) Only a person who hasn’t been to a cancer conference or read the scientific literature on cancer seriously over the last 10-20 years could say something so out of touch with the reality of what oncologists and cancer scientists actually say about the causes of cancer. Seriously, just do a PubMed search for “cancer” and “metabolism.” It’s so well-accepted that metabolism contributes to cancer formation and progression that there are numerous review articles about it going back a decade. (If Marik really wants to have his mind blown, he should do a PubMed search for “cancer” and “metabolic reprogramming.”) Oh, sure, he concedes that we know that some people have genetic susceptibilities to cancer—who can deny that?—but blithely goes on to say that those genetic susceptibilities probably all cause metabolic changes that cause cancer.
To provide some perspective, I can’t help but interject here that Douglas Hanahan and Robert Weinberg even updated their classic “hallmarks of cancer” article from 2000 to include cancer metabolism (“deregulating cellular energetics”)… in 2011. As time has gone on, I’ve come to suspect that the reason quacks love to invoke “metabolism über alles” as the cause of cancer (and most other disease) is because that makes it much easier for them to argue for dietary interventions as the cure for all disease. Indeed, Marik even cites BRCA1 and BRCA2. Many of you might be aware that certain mutations in these genes can result in a lifetime risk of breast or ovarian cancer approaching 80% (for breast cancer). Moreover, BRCA1 and BRCA2 are tumor suppressor genes that code for proteins whose function is DNA damage repair. When they don’t work due to a mutation, cancer becomes much more likely because DNA mutations accumulate without being repaired, something that would seem to belie Marik’s claims that cancer is metabolic derangement über alles.
In a mind-bogglingly stupid statement, Marik does not state the function of the proteins produced by BRCA1 and BRCA2 (likely because doing so would undermine his entire claim that cancer is mainly a metabolic disease), treats the two as though they were a single gene “the BRCA1/BRCA2 gene” (which they most definitely are not), and then cites a claim that the risk of cancer in mutation carriers used to be “only” 50% 20-30 years ago, but now is 70%, which left me scratching my head. He also neglects to note that the risk is different depending on which gene has a mutation, with oncogenic BRCA1 mutations portending a much higher lifetime risk of breast cancer than oncogenic BRCA2 mutations. Seriously, Marik has no idea what he’s talking about here, but that doesn’t stop him from claiming that “something” else must be going on. OK, so what? Let’s say Marik is correct here. Even in that case, then a gene mutation can cause cancer 50% of the time, and “other factors” at most increase that risk by an additional 20%. He undermines his own argument that cancer is always a “metabolic disease” through his own misunderstanding. Moreover, I couldn’t find any citation or reference in Marik’s cancer e-book to support his misleading factoid. Also, it never seems to occur to him that newer and more intensive testing for BRCA mutations and better epidemiological studies might play a role in changes in estimates of lifetime risk of breast and ovarian cancer in mutation carriers. (These days, a lot more women undergo genetic testing than in the 1990s.)
Unsurprisingly, to support his claim that cancer is a “metabolic disease,” Marik cites Thomas Seyfried, one of the main proponents of the overblown claim that cancer is primarily a metabolic disease. It’s been almost exactly a decade since I last wrote about Seyfried, specifically his risibly overblown claim that ketogenic diets “beat” chemotherapy for the treatment of cancer. As I said at the time, a few years prior to my writing that post, the hypothesis that cancer is primarily a metabolic disease was all the rage in oncology, and I remembered attending several sessions and lectures on the Warburg effect and cancer at the AACR meetings. I also noted that, by 2014, interest in the hypothesis had been waning somewhat, most likely because it had thus far failed to deliver much in the way of therapeutic targets and strategies. I also noted that Seyfried had expressed pride at having been interviewed by Joe Mercola. Here’s a hint: If you’re science-based, you avoid Mercola like the plague. It was true ten years ago, and it’s even more true now, given that Mercola has recently fallen under the spell of a psychic medium grifter claiming to channel an ancient powerful entity even to the point of taking his advice on how to run his business and firing longtime associates, including even his sister, and ghosting friends. So far, not a great source.
Of course, the question of whether the metabolic changes cause the mutations and chromosomal changes seen in cancer or vice-versa is a longstanding debate that Marik glides by as though it were totally settled. As is the case with cancer quacks, he vastly oversimplifies cancer science in favor of one hypothesis and ignores the likelihood that multiple changes contribute to the development, growth, and progression of cancer cells, likely in different combinations at different times, depending upon the step in carcinogenesis that the cancer has reached. I like to cite my previous primary area of research, tumor angiogenesis, the ability of cancer cells to stimulate the ingrowth of new blood vessels to support their growth. You might recall that without that ability cancer cells can only form tumors the size of a small lump of cells, because diffusion of oxygen and nutrients limits their growth to that. Until a new cancer somehow flips the “angiogenic switch,” that’s all it can be, a lump of cells. However, once it starts stimulating the ingrowth of new blood vessels, it can grow almost unchecked. I also recall that back in the 1990s targeting tumor angiogenesis was viewed as a potential cure for cancer, or at least as a strategy that could turn cancer into a chronic, manageable disease like hypertension or diabetes through prolonged use of angiogenesis inhibitors. Unfortunately, it didn’t turn out that way, although angiogenesis inhibitors have taken their place in the multimodality pharmacological treatment of cancer as an incremental advancement—just like most new cancer therapies.
In fact, let’s take a look at a couple of classic figures from Hanahan and Weinberg’s 2011 “hallmarks of cancer” review, compared to the original “hallmarks of cancer” figure from their 2000 review:
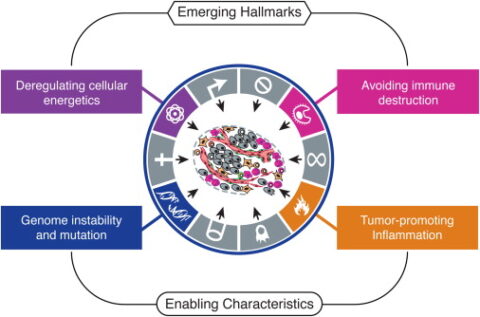
As I like to say, liberally paraphrasing what Douglas Adams said about space, cancer is complicated. You just won’t believe how vastly, hugely, mind-bogglingly complicated it is. I mean, you may think rocket science is complicated, but that’s just peanuts to cancer. That’s why it should be a huge red flag any time you see someone like Marik proclaiming just One True Cause of Cancer.
But what about the “5%” figure? I rather suspect that Marik pulled it out of his nether regions, or—shall we say?—”repurposed” the old “2% gambit” by making it less pessimistic. Given that I can’t find any new sources that I haven’t addressed before I will therefore refer you to my previous posts refuting the old and deceptive claim that chemotherapy “cures only 2%” of cancers and explaining how chemotherapy does work after all.
Chemotherapy vs. “repurposed drugs”?
One claim by cancer quacks like Marik that’s always irked me is that they are somehow the only people who have ever thought of “repurposing” drugs approved for other purposes to treat cancer. Seriously, I published a number of papers investigating the possibility of repurposing a drug for Alzheimer’s disease to treat cancer. My annoyance became very acute when I saw Marik flash this slide in his interview:
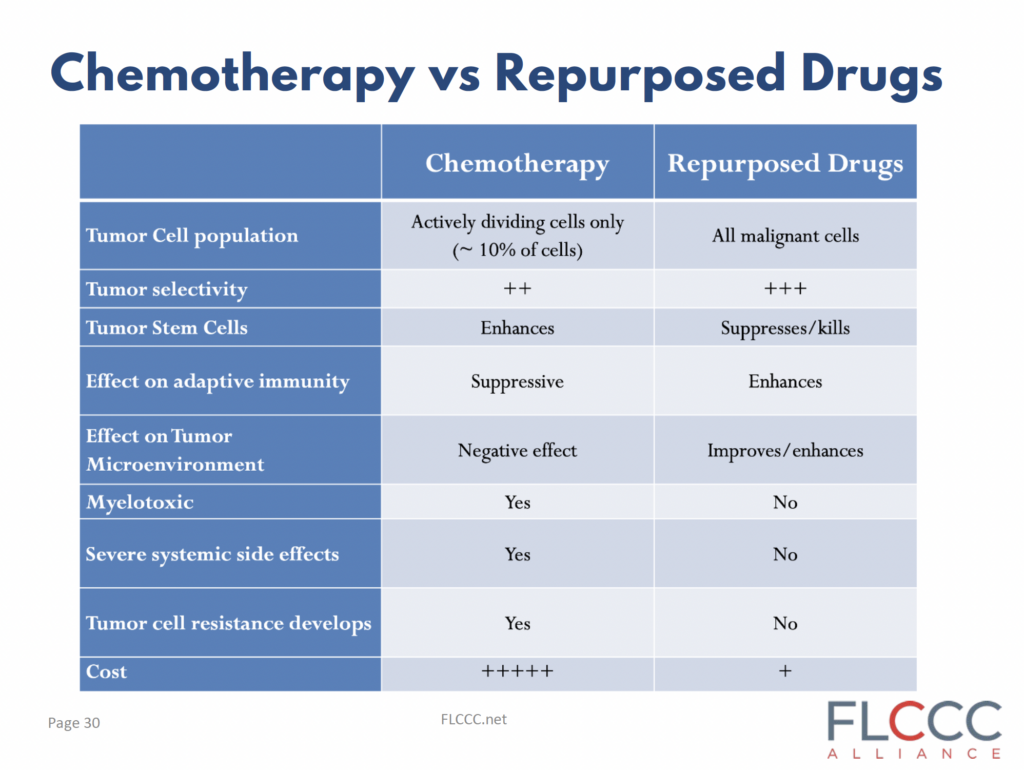
This is yet another of Marik’s deceptive tables. For example, the claim that repurposed drugs can affect “all malignant cells” is just nonsense. Different repurposed drugs can target different tumor cells, as such drugs work against certain cancers mainly because they target certain signaling or metabolic pathways that the disease for which they were approved has in common with those specific cancers. Similarly, there’s no good evidence that repurposed drugs in general—cough, cough, ivermectin—enhance adaptive immunity. And WTF does “improves/enhances” tumor microenvironment even mean? While it is true that tumor microenvironment (the cellular milieu, including immune cells, surrounding the tumor) can have a huge effect on tumor growth and progression, no evidence is presented that any of the “repurposed drugs”—cough, cough, ivermectin—has any effect on the tumor microenvironment.
Seriously, I laughed out loud at the claim that tumor cell resistance doesn’t develop against “repurposed drugs.” Here’s a hint for Marik: Tumor cell resistance can develop against pretty much any drug, chemotherapy, targeted therapy, immune therapy, or whatever. I remember in the 1990s how it was widely speculated that cancers would not develop resistance to antiangiogenic therapy because the therapy targeted normal vascular cells. Guess what? Just like in Jurassic Park, life (in this case, cancer, which is a particularly tenacious form of life) was not contained and did find a way. There are now known to exist multiple mechanisms by which tumors achieve resistance to angiogenesis inhibitors. The same will almost certainly be true for any repurposed drugs that, unlike most of what Marik lists, are shown to actually be efficacious as cancer treatments. Cancer finds a way, and resistance eventually develops. It’s a huge red flag for quackery when anyone claims otherwise, Marik’s claimed “deep dive into the literature” in which he supposedly personally reviewed “over 900 peer-reviewed” papers in one of his videos notwithstanding.
“New school” COVID-19 antivaxxers and quacks have now become just run-of-the-mill grifting antivaxxers and quacks, complete with the same claims of having “done their own research” in which they cherry pick the studies that they like, ignore the longstanding history of cancer research, and portray themselves as someone who has discovered something about cancer that “they” don’t want you to know about. The claim that chemotherapy “only cures 5%” ignores the difference between adjuvant chemotherapy and primary chemotherapy as treatment and that most cancers are now seldom treated with just one modality anymore. It is, in essence, a marketing tool in which the cancer quack disparages the competition in order to sell you something. In the case of Paul Marik, he’s selling ivermectin and other “repurposed” drugs for cancer, while in the case of The Vigilant Fox and 2ndSGitW, it’s the Joe Tippens protocol, which both include at the end of their articles featuring Marik.
The more things change, the more they stay the same in quackery world, and, of course, everything old is new again. Marik is just peddling the same old snake oil that cancer quacks have been peddling ever since chemotherapy started to enter the treatment regimens for various cancers, even as he portrays himself as promoting “integrative oncology.”