
{kind=link}
Like most doctors, I detest ICD codes, and in particular I detest ICD-10. Of course, I realize that most non-physicians reading this are asking, “What the heck is an ICD code, and what is ICD-10”? Basically, ICD stands for International Classification of Diseases, and ICD codes are alphanumeric codes used to classify diagnoses. They system’s history dates back to 1893, and the World Health Organization has been responsible for its maintenance and updating since its founding in 1948, at which time ICD-6 was the most current version. Indeed, The WHO Nomenclature Regulations, adopted in 1967, stipulated that Member States use the most current ICD revision for mortality and morbidity statistics. The ICD has been revised and published in a series of editions to reflect advances in health and medical science over time. The most current version is ICD-10, which was endorsed in May 1990 by the Forty-third World Health Assembly and formally adopted by the WHO in 1994.
ICD codes started out as being a standardized list of diseases and conditions to be used on death certificates as causes of death. These days, ICD codes are used for a number of purposes, although most doctors encounter these codes when they use them for billing insurance companies, Medicare, or Medicaid for their services. However, ICD codes are also used for epidemiology, health management, clinical diagnoses, and death certificates. According to the WHO:
ICD is the foundation for the identification of health trends and statistics globally, and the international standard for reporting diseases and health conditions. It is the diagnostic classification standard for all clinical and research purposes. ICD defines the universe of diseases, disorders, injuries and other related health conditions, listed in a comprehensive, hierarchical fashion that allows for:
- easy storage, retrieval and analysis of health information for evidenced-based decision-making;
- sharing and comparing health information between hospitals, regions, settings and countries; and
- data comparisons in the same location across different time periods.
Uses include monitoring of the incidence and prevalence of diseases, observing reimbursements and resource allocation trends, and keeping track of safety and quality guidelines. They also include the counting of deaths as well as diseases, injuries, symptoms, reasons for encounter, factors that influence health status, and external causes of disease.
Normally, ICD codes were updated roughly every ten years, but ICD-10 is now nearly a quarter of a century old. As you might imagine, it’s getting a bit long in the tooth, no matter how long the US delayed in requiring its use. (The US, being ever so slow, didn’t switch from ICD-9 to ICD-10 until 2015, after most of the rest of the world had been using ICD-10 for decades. I could go on about how much fun it was to make that switch at the hospital and clinic level, given that I was in charge of creating new billing forms for our breast center in preparation for the adoption of ICD-10, but I doubt that it would interest most of you.) So ICD-11 is in active development, having undergone field testing in 2017, with a current goal of a version to be approved in 2018, as this report indicates. There’s also this:
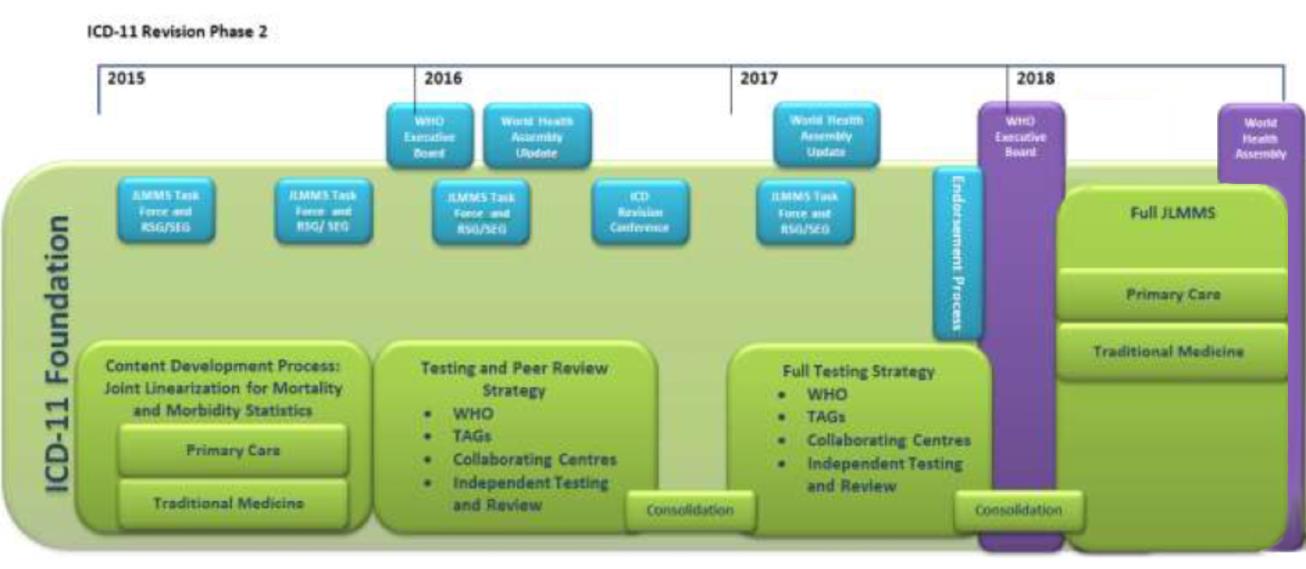
ICD-11 Project Plan
Do you see what I see all the way to the right of the timeline, near the end? Yes, it’s traditional medicine, and, yes, it is exactly what you think. Traditional Chinese medicine diagnoses are being incorporated into the ICD-11. Truly, the “integration” or “unification” of traditional Chinese medicine with science-based medicine is nearly complete. Let’s take a look. Soon (or maybe not so soon if the US takes as long to implement ICD-11 as it did to implement ICD-11), I will be able to code for liver yin deficiency pattern (ICD-11 code SF50) or liver qi stagnation pattern (ICD-11 code SF57). This is not the first time we have discussed the issue on SBM. Would that it were the last.
Quackery codes to be introduced in the ICD-11?
I decided to write about how quackery is insinuating itself into the ICD-11 because a reader sent me this link, which is a browser for the latest beta draft of ICD-11. You can scroll down to 26, which is Traditional Medicine conditions – Module 1, where the WHO describes this section thusly:
This chapter refers to disorders and patterns which originated in ancient Chinese Medicine and are commonly used in China, Japan, Korea, and elsewhere around the world. This list represents a union set of harmonized traditional medicine conditions of the Chinese, Japanese, and Korean classifications. For an extended list of traditional medicine conditions, please refer to the International Classification of Traditional Medicine (ICTM).
Oh, yes. There is an International Classification of Traditional Medicine (ICTM). I’ll get to that momentarily. First, let’s look at what the WHO has come up with for “integrating” traditional medicine into real medicine. In fairness, I will note that the introduction specifies this:
The use of the ICD-11 TM Chapter is optional for those who would like to record epidemiological data about traditional medicine practice. This chapter should not be used for mortality reporting.
Well that’s a relief! Of course, you and I know that, once ICD-11 is adopted, practitioners of traditional Chinese medicine (TCM), such as naturopaths, acupuncturists, and the like, will be lobbying hard to make sure that this chapter is used. But let’s look at what the WHO says about TCM:
A disorder in traditional medicine, disorder (TM)*, refers to a set of dysfunctions in any of the body systems which presents with associated manifestations, i.e. a single or a group of specified signs, symptoms, or findings. Each disorder (TM) may be defined by its symptomology, etiology, course and outcome, or treatment response. 1 Symptomology: signs, symptoms or unique findings by traditional medicine diagnostic methods, including inspection such as tongue examination, history taking (inquiry), listening and smelling examination, palpation such as pulse taking, abdominal examination, and other methods. 2 TM Etiology: the underlying traditional medicine explanatory style, such as environmental factors (historically known in TM translations as the external contractions), emotional factors (historically known in TM translations as the seven emotions), or other pathological factors, processes, and products. 3 Course and outcome: a unique path of development of the disorder (TM) over time. 4 Treatment response: known response to traditional medicine interventions. In defining a disorder (TM), symptomology and etiology are required. Course and outcome, and treatment response are optional.
A pattern in traditional medicine, pattern (TM), refers to the complete clinical presentation of the patient at a given moment in time including all findings. Findings may include symptomology or patient constitution, among other things. 1 Symptomology (as above). 2 Constitution: the characteristics of an individual, including structural and functional characteristics, temperament, ability to adapt to environmental changes, or susceptibility to various health conditions. This is relatively stable, being in part genetically determined while partially acquired.
Let’s take a look at some of the more…interesting…TCM diagnoses that ICD-11 will allow practitioners to code for:
SG26 Bladder meridian pattern (TM)
A pattern characterized by clashing headache and sensation that the eyes are being torn out. The nape of the neck is tight, there is pain in the spine, the waist arches backwards, the thigh cannot flex, the back of the knee has lumps and there is a sensation that the calf is being split apart. Symptoms and signs also include excess lacrimation, nasal congestion, pain in the head, neck, back, waist, sacrum, back of the knee, calf and foot, and impaired use of the little toe. It may be explained by Bladder meridian dysfunction.
I do like the addition of “impaired use of the little toe.” It’s such a nice little detailed touch to the otherwise nonspecific. That’s the symptom that cinches the diagnosis, I bet. Of course, if you have a headache so severe that it feels as though your eyes are being torn out, along with pain in the spine and all these other symptoms, I’d be worried about either a brain tumor or meningitis, among other potentially life-threatening conditions. Of course, adding all these other symptoms just makes the whole thing a mess. But you’ll soon be able to code for it!
I like this next one just for the name:
SG29 Triple energizer meridian pattern (TM)
A pattern characterized by deafness and tinnitus, swelling and obstruction of the throat. Symptoms and signs also include sweating, pain at the lateral corners of the eye and cheeks, pain behind the ear and along the shoulders, upper arms, elbows and outer border of the forearms and impaired use of the fourth finger. It may be explained by Triple Energizer meridian dysfunction.
I suppose this must be worse than the double or single energizer meridian pattern. Actually, there doesn’t appear to be such a diagnosis. Why always triple? Who knows. I do note, though, that there are various subdiagnoses, including upper energizer stage patterns (SG70), middle energizer stage patterns (SG71), and lower energizer stage patterns (SG72). Of course, you know this is an ICD classification, because even diagnoses based on prescientific mystical beliefs include something like triple energizer stage patterns (TM), unspecified (SG7Z). Doctors, nurses, medical coders, and others who use ICD-10 codes on a regular basis will get that joke.
Before I move on, I can’t resist listing a couple more. I mentioned that I’ll soon be able to code for liver qi stagnation, but what does that mean? It means exactly what it sounds like:
SF57 Liver qi stagnation pattern (TM)
A pattern characterized by distending and burning pain of the hypochondrium, along with restlessness, irritability, bitter taste, dry mouth, red tongue with yellow coating or a wiry rapid pulse. It may be explained by long-term stagnation of liver system qi induced internal fire factor that affects tissues and functions associated with the liver system.
Because I sure don’t want my qi stagnated by internal fire factor or qi stagnation producing internal fire factor. (I can’t tell which they mean from the rather garbled phrasing of that definition.) In any case, these Traditional Medicine codes are all based on several patterns. Here are several:
- Principle-based patterns: “Based on the analysis of symptomatology and constitution of a patient, patterns are categorized into eight principles which consist of four groups of opposing characteristics i.e. Yin & Yang, Heat & Cold, Deficiency & Excess and Interior & Exterior (and with the addition of three intermediate patterns). These principles constitute the most basic patterns which may be combined for pattern differentiation in more refined detail.”
- Environmental factor patterns: “This section comprises patterns with a shared explanation related to environmental factors (i.e. wind, cold, dampness, dryness, fire, summer-heat) and the presence of the pathogens, parasites or toxins.”
- Body constituents patterns: “This section comprises a range of dysfunctions of four body constituents, which is qi, blood, fluid and essence. These patterns are grouped together on the basis of their common etiology such as an abnormal flow of qi, blood, or essence or dysfunctional distribution of fluid.” (I note that this section has diagnoses like qi deficiency pattern, qi stagnation pattern, qi uprising pattern, qi collapse pattern, qi sinking pattern, and, of course, qi patterns, unspecified.)
- Organ system patterns: “This section comprises a range of Qi disturbance patterns grouped together on the basis of their having in common a demonstrable etiology in Qi, which means invisible action, function, or working that circulates throughout the body. Qi Patterns (TM) may be explained by a disorder of physical energy supply, mental disorder, or a [sic] autonomic nerve system disorder.”
- Meridian and collateral patterns: “This section contains a group of TM patterns caused by functional disorder of meridians consisting of twelve main meridians and eight extra meridians.”
- Six stage patterns: “This section contains patterns in accordance with the six-stage theory. A common characteristic of the Six-stage patterns included in this section is their relationship with the acute febrile conditions.”
- Triple energizer stage patterns: “This section comprises dysfunctional systemic patterns of coordination, assimilation, elimination and integration attributed to invasion and transformation of the dampness-heat factor on the three portions of the body cavity (upper energizer, middle energizer and lower energizer), through which the visceral qi is transformed.” And you wouldn’t want your visceral qi transformed, now would you?
- Four constitution medicine patterns: “Four Constitution Medicine Patterns are classified by each type of constitution: Large Yang Type (Large Lung Small Liver), Small Yang Type (Large Spleen Small Kidney), Large Yin Type (Large Liver Small Lung), and Small Yin Type (Large Kidney Small Spleen). Metabolic processes in Four Constitution Medicine can be divided into 2 categories: Qi-Humor metabolism and Water-Food metabolism. Large Yang Type patterns and Large Yin Type patterns are caused by disorder of the Qi-Humor metabolism while Small Yang Type patterns and Small Yin Type patterns are caused by disorder of the Water-Food metabolism. Patterns occurring for each type of constitution can be subdivided into three types: external TM disorder, internal TM disorder and external-internal combined TM disorder. External TM disorder is caused by imbalance of Seong (Innate Nature) and internal TM disorder is caused by the imbalance of Jeong (Emotional Disposition).”
I could go on, as I didn’t list all of them, but you get the idea. These diagnoses are not based in science or modern medicine, but rather in prescientific beliefs about the body and vitalistic mystical and religious beliefs dating back millennia. Such diagnoses have no place being included in a classification system that is supposed to reflect the latest in medical science. If you don’t believe me, I encourage you to go to the ICD-11 Beta Draft and peruse Traditional Medicine Conditions.
Why is the WHO “integrating” quackery with real medicine in ICD-11?
As I perused the ridiculous pseudoscientific “diagnoses” in the Traditional Medicine section of the ICD-11 Beta Draft, one question kept going through my mind: Why? Why is the WHO “integrating” quackery with real medicine in the official disease classification system used by basically the whole world? Why is it betraying the trust it was granted when the maintenance and updating of the International Classification of Diseases were first entrusted to it in 1948? It began with something I mentioned above, the International Classification of Traditional Medicine (ICTM), a project designed to classify the use of traditional medicine. The WHO justified starting the ICTM project by pointing to a survey of its member nations that showed that in some Asian countries, over 80% of the population depends on some form of traditional medicine. Of course, my response to that factoid would be that greater efforts must be made to get science-based medicine to these people, not that we should infect the ICD system with quack diagnoses, but that’s just me.
In any event, this is the WHO’s justification for developing the ICTM:
“We recognize that the use of traditional medicine is widespread. For many people – especially in the Western Pacific, South-East Asia, Africa and Latin America – traditional medicine is the primary source of health care,” said Dr Marie-Paule Kieny, Assistant Director-General of Innovation, Information, Evidence and Research at WHO. “Throughout the rest of the world, particularly Europe and North America, use of herbal medicines, acupuncture, and other traditional medicine practices is increasing. Global classification and terminology tools, for traditional medicine, however, have been lacking.”
And:
“Several countries have created national standards for the classification of traditional medicine but there is no international platform that allows the harmonization of data for clinical, epidemiological and statistical use. There is a need for this information to allow clinicians, researchers and policy-makers to comprehensively monitor safety, efficacy, use, spending and trends in health care,” said Kieny.
The classification will initially focus on traditional medicine practices from China, Japan and the Republic of Korea that have evolved and spread worldwide.
Believe it or not, I could support an international classification system for traditional medicine if its sole purpose were as a research tool and it were kept separate from science-based classifications. For instance, such a classification could be used to study herb-drug interactions, an area where there is a great deal that is still unknown. Also, if we knew who uses TCM, for what conditions, and why, we might be able to develop more effective strategies to encourage the use of effective science-based medicine in such populations. I am even sympathetic to one argument, which is that many indigenous peoples are essentially “invisible” to health statistics because they use only traditional medicine.
To address these problems does not require integrating such a classification system with ICD-11, and, such uses were never the intent for the ICTM, which was always intended to be integrated into ICD-11 from its very inception. Indeed, the WHO has been promoting traditional medicine use for a long time. I first became aware of it a few years ago, when the WHO participated in writing supplements for Science promoting the “integration” of TCM with science-based medicine. One of the supplements discussed the WHO’s Traditional Medicine Strategy (2014– 2023), highlighting the global scientific challenges and showing how a systems biology approach can be applied to traditional medicine like acupuncture.
Before that, though, in 2008, the WHO held a Congress on Traditional Medicine in Beijing and adopted the Beijing Declaration, which was basically a declaration to support the use of traditional medicine. You can read the whole declaration for yourself here, but here are some key statements:
I. The knowledge of traditional medicine, treatments and practices should be respected, preserved, promoted and communicated widely and appropriately based on the circumstances in each country.
Yes, you read that right. It gets worse, though. Here are three more parts of the Declaration:
III. Recognizing the progress of many governments to date in integrating traditional medicine into their national health systems, we call on those who have not yet done so to take action.
And:
V. Governments should establish systems for the qualification, accreditation or licensing of traditional medicine practitioners. Traditional medicine practitioners should upgrade their knowledge and skills based on national requirements.
VI. The communication between conventional and traditional medicine providers should be strengthened and appropriate training programmes be established for health professionals, medical students and relevant researchers.
This is nothing less than a call for the full “integration” of TCM quackery with science-based medicine. I can’t help but point out that the WHO’s own press release on ICTM in 2010 stated that its purpose was to “assist in creating an evidence base for traditional medicine,” as though the assumption was that traditional medicine works. As Ryan Abbott, director of research and project management for Nova Worldwide Consulting and a former member of WHO’s traditional medicine team, put it, “Inclusion in the WHO Family of International Classifications, a very conventional tool of mainstream medical care, would be a powerful endorsement of traditional medicine.” Abbott also noted that an additional impact might include greater insurance reimbursement for traditional providers and services.
Because of course it will. That’s a huge part of the purpose. Insurance companies, governments, and third party payers use ICD-10 codes and CPT procedure codes to determine reimbursement. Inclusion of traditional medicine diagnoses in ICD-11 would provide a powerful tool for quacks to use to lobby for reimbursement for their services.
Proponents also know what the purpose of ICTM and its integration into ICD-11 really is:
The ICTM can be used as an independent, stand-alone classification and could also be included as an additional chapter within the ICD, in part or as a whole. This will enable unification of the conventional and traditional medicine classifications for diagnosis and interventions. The project will establish links with the WHO Family of International Classifications (WHOFIC) network to enable the membership of ICTM as a derived classification of the WHO family.
That’s the real purpose of ICTM and the inclusion of a subset of it in ICD-11: The “integration” of quackery as an equal with science-based medicine. Yes, the WHO says that the traditional medicine module of ICD-11 is optional. For now. I predict that it won’t be long after ICD-11 is adopted and various nations begin to implement it that it will cease to be optional.
Somewhere Chairman Mao Zedong is smiling
I’ve written before, as have other SBM bloggers, about how the construct that we know today as “traditional Chinese medicine” was actually created by Communist dictator Chairman Mao Zedong in the 1940s and 1950s. Basically, Mao, seeing that he did not have the resources to provide real medicine to all his people, decided to tap into the various schools of traditional medicine. In doing so, he and his physicians and scientists essentially retconned the history of TCM to turn it into seemingly an intellectually consistent whole system, when in reality there were many forms of traditional Chinese medicine flowing out of many folk traditions. Meanwhile, Mao himself eschewed TCM, not believing in it:
…In The Private Life of Chairman Mao, Li Zhisui, one of Mao’s personal physicians, recounts a conversation they had on the subject. Trained as an M.D. in Western medicine, Li admitted to being baffled by ancient Chinese medical books, especially their theories relating to the five elements. It turns out his employer also found them implausible.
“Even though I believe we should promote Chinese medicine,” Mao told him, “I personally do not believe in it. I don’t take Chinese medicine.”
Yet in a 1950 speech, Mao proclaimed:
Our nation’s health work teams are large. They have to concern themselves with over 500 million people [including the] young, old, and ill. … At present, doctors of Western medicine are few, and thus the broad masses of the people, and in particular the peasants, rely on Chinese medicine to treat illness. Therefore, we must strive for the complete unification of Chinese medicine. (Translations from Kim Taylor’s Chinese Medicine in Early Communist China, 1945-1963: A Medicine of Revolution.)
Indeed, much of the reason why TCM spread beyond China to much of the developed world, to the point that major academic medical centers such as the Cleveland Clinic offer it, is because Mao aggressively promoted it. Indeed, if you want to know just how aggressively over how long a period of time Mao promoted the export of TCM, it’s worth it to read Kimball Atwood’s epic “Acupuncture Anesthesia”: A Proclamation from Chairman Mao, particularly part III, in which Mao’s efforts to unify TCM with “Western” medicine into a new “whole” are detailed. Indeed, it’s worth repeating Communist Party slogans about medicine from Mao’s era:
1945-50 ‘The Co-operation of Chinese and Western Medicines’
1950-8 ‘The Unification of Chinese and Western Medicines’
1950-53 ‘Chinese Medicine studies Western Medicine’
1954-8 ‘Western Medicine studies Chinese Medicine’
1958- ‘The Integration of Chinese and Western Medicines’
Lest you think that the above slogans are merely artifacts of history from 60+ years ago, think again. A little over a year ago, China passed a law requiring the “integration” of TCM with “Western” medicine, explicitly elevating its status with respect to the state to be on “equal footing.” It also goes a long way towards protecting the business interests of TCM industries, such as those that manufacture herbal remedies. So China is still in the business of promoting the export of TCM, even more than 40 years after Mao’s death.
I doubt that even Mao could have imagined such a triumph of completely integrating TCM into the very codebook for modern medical diagnoses, the ICD-11, but that triumph will soon be upon us. My only hope in the US is that we will be as slow to adopt ICD-11 as we were to adopt ICD-10.